
Abstract
BACKGROUND:
The implementation of digital breast tomosynthesis has increased the detection of architectural distortion (AD). Managing this finding may be experienced as a clinical dilemma in daily practice. Breast Contrast-Enhanced MRI (CE-BMR) is a known modality in case of problem-solving tool for mammographic abnormalities. However, the data about AR and CE-BMR are scant.
OBJECTIVE:
The purpose was to estimate the benefit of CE-BMR in the setting of architectural distortion detected mammographically through a systematic review and meta-analysis of the literature.
METHODS:
A search of MEDLINE and EMBASE databases were conducted in 2020. Based on the PRISMA guidelines, an analysis was performed using the chi-square test of independence to determine if there was a significant association between the result of the test (positive or negative) and the participant condition (malignant or non-malignant).
RESULTS:
Four studies were available. The negative predictive value (NPV) was 98.3% to 100%. The result of the chi-square indicated that there was significant association between the participant test result and the participant condition for the included publications (X
CONCLUSIONS:
The high NPV could allow for deferral of a biopsy in favor of a short-interval imaging follow-up in the setting of a negative CE-BMR.
Introduction
Magnetic resonance imaging (MRI) is a valuable tool for the detection of breast cancer. Due to it having the highest sensitivity for the detection of breast cancer among current stand-of-care imaging modalities [1,2], its utilization in daily clinical practice has increased over the last several decades [3]. The current indications for contrast-enhanced breast MRI (CE-BMR) include screening of high-risk patients, to evaluate the extent of disease in the setting of a known cancer diagnosis, to evaluate tumor response to neoadjuvant chemotherapy, and for the additional evaluation of clinical or imaging findings after a problem-solving mammogram and/or ultrasound in the diagnostic setting [4].
Since the implementation of digital breast tomosynthesis (DBT), there has been an increase in the detection of architectural distortion [5,6]. Architectural distortion (AD) is defined as distortion of the breast parenchymal normal architecture without a definable mass visible [7], Fig. 1. AD represents the third most common imaging finding presentation of breast cancer mammographically, after a mass or calcifications [8]. DBT-detected architectural distortion without an ultrasound correlate is less likely to represent a carcinoma, compared to architectural distortion detected with conventional mammography [6]. Thus, managing the increased detection of AD with DBT is a clinical dilemma. Although the risks from needle core biopsy are much lower than an open surgical biopsy, complications are still possible [9]. Breast CE-BMR utilization as a problem-solving tool for the additional evaluation of mammographically detected AD has been reported in a few studies [10–12].
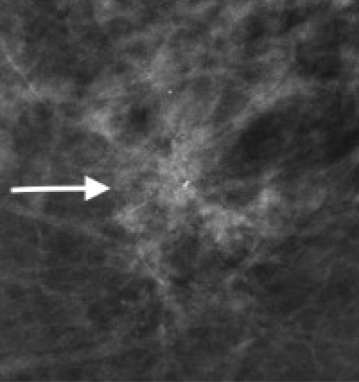
Left CC compression view showing persisting architectural distortion. No clear mass is identified within the architectural distortion.
The purpose of this study was to estimate the benefit of CE-BMR in the setting of architectural distortion detected mammographically through a systematic review and meta-analysis of the literature.
Guidelines for PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) were followed [13,14]. No ethical committee approval was needed for this retrospective meta-analysis study. No specific funding or support were received for this study.
Search strategy and study eligibility criteria
We performed a search of all studies within the Medline and Embase databases through June 2020. All the studies reporting the correlation of breast CE-BMR for AD detected mammographically were searched. In addition, the correlation of CE-BMR findings and definite pathology or follow up was performed. Malignant was defined as an invasive mammary carcinoma with or without ductal carcinoma in situ (DCIS) and DCIS-only. All the other pathologies were considered nonmalignant.
The search string for this study consisted of the following: “architectural distortion” AND “breast MRI” OR ‘MRI’ AND ‘article’. Only manuscripts written in English were considered for the analysis. Publications were selected on the basis of title and abstract by one reader (RF with 10 years of dedicated breast imaging experience). Once publication selection was performed, the full text of each study was assessed by both readers (RF with 10 years of breast experience, CMK with >20 years of dedicated breast imaging experience) alone and in consensus. The details regarding the number of AD lesions with correlation with breast CE-MR were analyzed, as well the reported outcomes (surgical pathology or follow-up) for each selected publication.
Data extraction
The two independent readers performed the data extraction. In case of disagreement, there was a mutual consensus approach. When possible, the following data were recorded for each selected study publication:
Year of publication Study design Number of patients and number of lesions Breast imaging modalities used Rate of AD managed with surgical excision and/or follow-up
Primary point
The primary and unique outcome was the correlation between CE-BMR findings and definite outcome for AD.
Quality assessment
The quality assessment of Diagnostic Studies-2 tool (Quadas-2 tool) assessed the search quality, risk of bias and applicability [15]. We followed the four following recommended categories (patient selection, index test, reference standard, flow) with the risk of bias as high, low or unclear.
Statistical analysis
Statistical analysis was performed by using commercially available software (Comprehensive Meta-Analysis, version 2.2.057; Biostat, Englewood, NJ). The chi-square test of independence was used to determine if there was a significant association between two categorical variables. For this analysis, we investigated if the result of the test (positive or negative) was dependent on the participant condition (malignant or non-malignant).
The hypothesis and rejection rules are defined below:
Null hypothesis: There is no association between the participant test result and the participant condition (i.e. they are independent). Alternative hypothesis: There is significant association between the participant test result and the participant condition (i.e. they are dependent). Rejection rule: Reject null hypothesis if the p-value < 0.05.
In addition, the Pearson Chi-Square test was performed to determine the dependency of variables and the Fisher exact test was used_to determine whether or not there was a significant association between two categorical variables.
Results
Literature search and characteristics of the analyzed studies
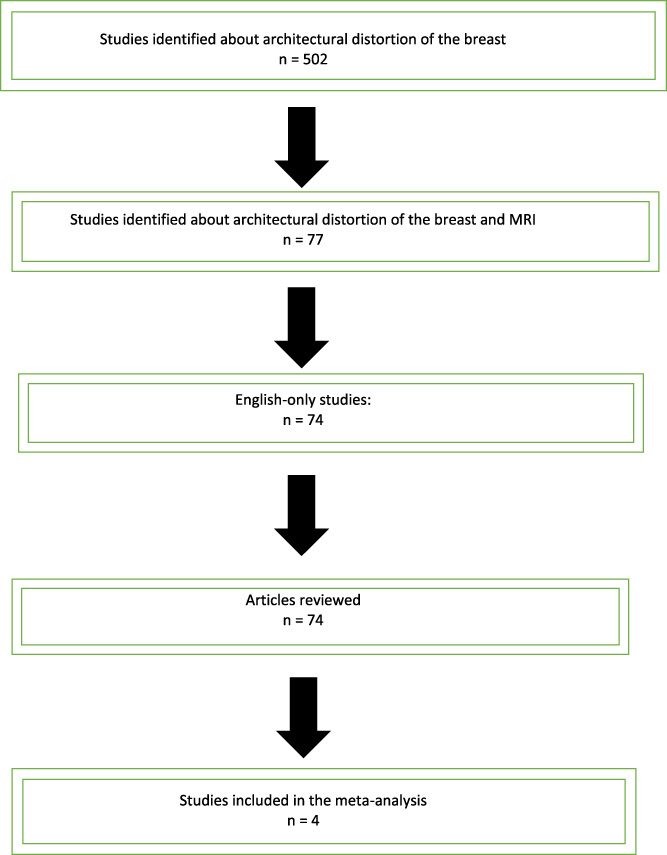
The literature search flowchart is demonstrated on Table 1. From 502 retrieved publications, only four (1.0%) matched the inclusion criteria and were analyzed.
Process for selecting studies
Process for selecting studies
The articles were published from March 2009 to January 2020 [9,16–18]. The characteristics of the analyzed studies are shown in Tables 3(a)–(d). Consequently, our study cohort consisted of a total 301 AD lesions that underwent breast MRI imaging.
We used the risk of bias and applicability of the included studies with the Quadas-2 tool (Table 2). The authors approved the studies to answer the research question. Otherwise, the risks were assessed to be low.
Graph showing risk of bias and applicability concerns for each study in this meta-analysis using the Quality Assessment of Diagnostic Studies-2 (Quadas-2 tool)
Graph showing risk of bias and applicability concerns for each study in this meta-analysis using the Quality Assessment of Diagnostic Studies-2 (Quadas-2 tool)
- Low risk. + High risk. ? Unclear risk.
Amitai’s analysis
a. 0 cells (0.0%) have expected count less than 5. The minimum expected count is 8.28. b. Computed only for a 2 × 2 table.
Lifang’s analysis
a. 0 cells (0.0%) have expected count less than 5. The minimum expected count is 7.37. b. Computed only for a 2 × 2 table.
Moy’s analysis
a. 3 cells (75.0%) have expected count less than 5. The minimum expected count is 0.08. b. Computed only for a 2 × 2 table.
Spick’s analysis
a. 1 cells (25.0%) have expected count less than 5. The minimum expected count is 1.82. b. Computed only for a 2 × 2 table.
Total cases analysis
a. 0 cells (0.0%) have expected count less than 5. The minimum expected count is 7.37. b. Computed only for a 2 × 2 table.
Results for each analysis are detailed in Tables 3(a)–(d). The sensitivity ranged from 94.8% to 100% and the specificity varied from 41.4% to 100%. The positive predictive value (PPV) was between 30.4% to 100% and the negative predictive value (NPV) was 98.3% to 100%. Since there was no expected cell count less than 5, the result of the chi-square indicated that there was significant association between the participant test result and the participant condition for the included publications (X
The result of the analysis showed that there was a significant association between the participant test result and the participant condition, that is, the participant test result was dependent on their condition for the studies by Amitai et al., Ligang et al., Spick et al., and all the whole cohort [9,16–18]. The result also demonstrated there was no significant association between the participant test result and the participant condition for the study by Moy et al.

Sagittal Fat SAT post gadolinium T1image of left breast showing an irregular mass correlating with the architectural distortion seen initially on mammogram.
Only two of the studies described the CE-BMR findings of AD [9,18]. Both reported AD presenting as mass enhancement in approximately 50% of their cases [46.4% (32/69), 50% (14/28)] [9,18]. The mass characteristics were reported by as irregular in shape with non-circumscribed margins with the majority displaying washout or plateau features [9,18], Fig. 2. The remaining enhancing lesions in both studies were characterized as NME [53.6% (37/69), 50% (14/28)] [9,18].
Malignancy upgrade rate
The pooled malignancy rate of the studies evaluated was 18.5%. Only one study, reported a higher malignancy rate of 49.1% [18]. The disease prevalence was similar in three studies. (Tables 3--4).
Publication bias
The leave-one-out analysis was not influenced by a single study. There was no variation of the pooled NPV in the leave-one-out analysis.
Discussion
The differential diagnosis of AD includes both malignant and benign etiologies. The most frequent malignant lesion presenting as AD is invasive ductal carcinoma, 65% of cases [19–21]. The next most common malignancy is lobular carcinoma, 21% of cases [19]. In regard to benign lesions presenting as AD, the most common one is a radial scar (RS), 86% of cases [19–21]. A radial scar is a benign proliferation of epithelial elements [22]. Other common benign causes of AD include post-traumatic fat necrosis with or without a history of surgery (11%) and sclerosing adenosis (3%) [19–21].
With the implementation of DBT, there has been an increase in the detection rate of AD. Chong et al. reported that with the use of DBT that the number of incidental findings of AD increased by 26% [23]. Several studies have demonstrated that DBT-detected only AD with no ultrasound correlate has a lower likelihood of being a malignancy compared to AD detected on conventional mammography [24–26]. In a recent meta-analysis by Choudhery et al., they showed a pooled predictive positive value for malignancy of AD of 34.6% (339/557) [6].
Our study demonstrates a collective PPV of 44.6 % in patients with mammographically detected AD evaluated with CE-BMR. Because this value is higher than the 2% PPV threshold for a breast biopsy, the indication of biopsy is still warranted in these patients. Our findings confirm PPV variability in CE-BMR. It has been reported in multiple studies [27] that false positives (FPs) can be encountered in CE-BMR with normal breast tissue and/or benign lesions that mimic malignancies. Several studies have reported false positives rates with RS. In the study by Linda et al., they showed the lowest sensitivity with RS, i.e., 505 compared to other lesions (75%) (versus papilloma, lobular neoplasia, ADH) [28]. Of the 30 RSs excised surgically, 14 (14/30, 47.7%) were not associated with atypia/malignancy while atypia/malignancy was found in 16 (16/30, 53.3%) RSs. No significance difference was found. The study by Alsharif et al., reported that CE-BMR did not differentiate pure RS versus RS associated with atypia/malignancy [29].
Our meta-analysis data demonstrated a malignancy upgrade rate of 18.5% AD with the evaluation of CE-BMR. Several authors have utilized MRI to evaluate upgrade rates of other mammographically detected high-risk lesions. Tsuchiya et al. evaluated 17 patients diagnosed with atypical ductal hyperplasia (ADH) at conventional image-guided needle core biopsy and 9 were upgraded to malignancy. CE-BMR demonstrated suspicious enhancement at the site of biopsy in all upgraded patients for an upgrade rate of 53.0% [30]. Of the 155 high-risk breast lesions diagnosed at conventional image-guided needle biopsy and evaluated with CE-BMR by Londero et al, 28 (18%) of the high-risk lesions were upgraded to malignancy (9 papillomas, 1 radial sclerosing lesion, 11 lobular neoplasia and 7 ADH) [31]. The authors concluded that that absence of enhancement at dynamic MRI allowed reliable exclusion of invasive cancers among high-risk lesions diagnosed at needle biopsy.
CE-BMR has been reported to have a high NPV for problem-solving, reaching nearly 100% [16,27,31,32]. Our study results are within the range of previously published studies. Thus, with its high NPV, CE-BMR may have a role as an additional problem-solving tool in the evaluation AD without an ultrasound correlate in patients who do not want to undergo biopsy.
Our study has some limitations. All studies in this analysis were retrospective, which can introduce a bias with a variability in design and patient selection. Also, there was a low number of studies that assessed the predictive role of CE-BMR to assess AD. Some studies included other non-AD lesions in their initial evaluations. Another limitation was the low numbers of known AD DBT-only cases. Finally, a few of the included studies contained follow-up of AD, instead of a pathologic diagnosis for confirmation.
Conclusion
To our knowledge this is the first reported meta-analysis assessing mammographically detected AD with CE-BMR. The data demonstrated a high negative predictive value. Thus, this information may allow for the deferral of a biopsy in favor of a short-interval imaging follow-up in the setting of a negative CE-BMR. However, future prospective studies are needed to support these findings.
Abbreviation
Architectural distortion (AD) Breast Contrast-Enhanced MRI (CE-BMR) negative predictive value (NPV) Magnetic resonance imaging (MRI) digital breast tomosynthesis (DBT) PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) positive predictive value (PPV)
Footnotes
Conflicts of interests
None.