
Abstract
The 42-year-old patient, diagnosed with Stage IIA breast cancer, completed the postoperative adjuvant chemotherapy and radiotherapy. At the 11th year of diagnosis, a 3 cm tumor was detected in the pancreas and pancreatectomy was performed. Although the diagnosis of primary pancreatic adenocarcinoma was made at first, then the pancreatic metastasis of breast cancer was discovered. Pancreatic metastasis of breast cancer is extremely rare, and a limited number of patients have been reported in the literature. Here, we report an additional case of this rare tumor and the problems correlating with its diagnosis.
Introduction
Most tumors of the pancreas are primary pancreatic tumors. Pancreatic metastasis of other organ malignancies are rare and mainly includes renal cell carcinoma, non-small cell lung carcinoma, and colon carcinoma [1]. However, breast carcinoma accounts only for 5% of tumors that metastasize to the pancreas [2]. In this case report, we aimed to present the recurrence of a breast cancer patient with pancreatic metastasis.
Case report
Fifteen years ago, in 2005, a 42-year-old female patient was admitted to our hospital with a mass in her right breast. Amass lesion of 2 × 1.5 cm was palpated and a tru-cut biopsy was performed. In pathological examination, an invasive ductal carcinoma was diagnosed which estrogen receptor (ER) was found to be 90% (+), progesterone receptor (PR) 20% (+), and c-erbB-2 (−). Modified radical mastectomy and axillary lymph node dissection were performed. With the diagnosis of T2N0M0 invasive ductal carcinoma, 4 cycles of adriamycin+cyclophosphamide were administered as adjuvant therapy. The patient was followed up with tamoxifen for seven years when local recurrence was detected in 2012. Upon this, surgical resection was performed and following the postoperative chemotherapy of adriamycin+cyclophosphamide, paclitaxel treatment was administered. After chemotherapy, the patient was followed up with letrozole.
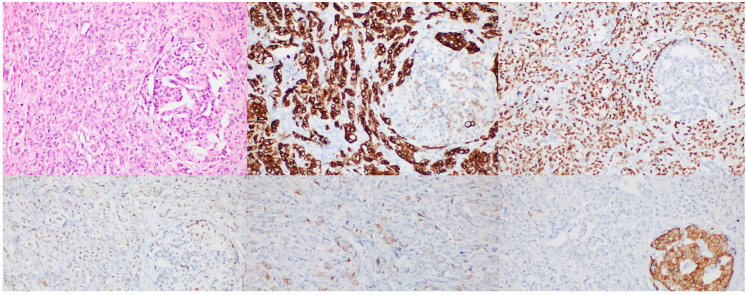
Metastatic infiltrative breast carcinoma within pancreatic tissue (residual Langerhans islet on the right) (A). Immunohistochemically: infiltrating tumor cells showed diffuse, strong, cytoplasmic positivity with CK 19 (B), diffuse nuclear and cytoplasmic staining with GATA-3 (C), mild to moderate, heterogenous nuclear staining with Estrogen Receptor (D) and focal moderate positivity with mammoglobin (E). Residual Langerhans islet cell were positive with synaptophyisin (F).
The patient, who was followed up with hormone therapy without any problem, developed a new onset jaundice and epigastric pain in 2016. Radiological imaging revealed a 3 cm mass at the head-body junction of the pancreas and the patient underwent a pancreatectomy. The operation of the patient and the pathological examination of the material was performed in another tertiary hospital. After the diagnosis of pancreatic adenocarcinoma, the patient was given adjuvant gemcitabine + capecitabine treatment with the diagnosis of this second primary carcinoma. Letrozole treatment was continued without interruption. Two years later, liver metastases were detected and metastasectomy was recommended to the patient. During the operation peritoneal carcinomatosis was detected. Omental biopsy was taken and the procedure was terminated. In the immunohistochemical staining of omentum biopsy, ER, GATA-3 and mammaglobin was found to be positive. Upon these results, capecitabine + cyclophosphamide treatment was given to the patient who was considered to have recurrence of breast cancer and the complete response was found in PET-CT applied at the 6th month of the treatment. Two years later, in 2020, the patient, who was followed up with hormone therapy, was found to have liver metastasis again. Liver biopsy was reported as metastatic breast carcinoma with GATA-3 (+), ER (+), PR (+), and c-erbB-2 (−) immune profile, similar to the previous one. Because the patient was diagnosed with pancreatic cancer, but recurrent intraabdominal breast cancer metastases were detected, the patient was re-evaluated with all archived data at the pathology-oncology clinical council. Meantime, the tissue blocks obtained from the pancreatectomy specimen of the patient were consulted to our pathology department and the infiltrative tumor in the pancreas was evaluated as invasive ductal breast carcinoma metastasis, since it was ER (+), PR (+), GATA-3 (+), and mammaglobin (+) (Fig. 1). Chemotherapy was discontinued in the patient, who was given 4 cycles of paclitaxel+cyclophosphamide with a partial response. Fulvestrant and ribociclib combination therapy was initiated; however, disease progression was detected in six months of hormone therapy. Then, ixabepilon+capecitabine treatment was started. The patient was followed up in the third month of ixabepilon+capecitabine treatment with an ECOG performance score of 1.
Pancreatic metastasis of breast cancer is extremely rare. In this case report, a breast cancer patient with pancreatic metastasis and a long-term follow-up is presented. Pancreatic cancer was considered as the second primary malignancy in a breast cancer patient followed up with remission and breast cancer metastasis was detected as a result of pathological evaluations.
When a solitary mass is detected in the pancreas, differential diagnosis should be made based on the patient’s history, imaging methods, and pathological evaluation. Definitive diagnosis can only be made by pathological evaluation and immunohistochemical staining has an important role in pathological differential diagnosis. Pancreatic cancer and breast cancer mostly have adenocarcinoma morphology and some immunohistochemical stains may be similar [3]. For example, both can be cytokeratin (CK) 7 (+) and CK 20 (−). Positive staining of breast cancer with hormone receptors can be used to distinguish between two malignancies [3]. However, many other tumors may be ER (+). GATA-3, GCDFP-15 and mammaglobin can be shown as breast cancer specific stains [4]. In our case, although pancreatic cancer was initially considered and treated accordingly, GATA-3 and mammaglobin were stained positively in biopsies taken from recurrent samples. When the pancreatic material was examined again, it was seen that it had a similar immunohistochemical profile and morphology. Histopathological evaluation with immunohistochemical staining explained the course of the disease and treatment was changed according to these results.
The follow-up and treatment of invasive breast cancer patients differ with pancreatic cancer. Gemcitabine-NabPaclitaxel or FOLFIRINOX treatment is recommended as the first line therapy for pancreatic cancer, however these chemotherapy regimens are not used in the treatment of breast cancer [5]. Therefore, correct diagnosis is the cornerstone in determining the treatment process. Detection of breast cancer metastasis to the pancreas will reveal the aggressiveness of breast cancer and will directly affect the clinician’s choice of chemotherapy or hormonotherapy. In our case, capecitabine and gemcitabine therapies used as adjuvant therapies are already effective agents in the treatment of breast cancer. Therefore, the patient was not deprived of effective treatment. Nevertheless, a detailed histopathological evaluation must be performed in a patient with a history of malignancy before making a second primary malignancy diagnosis.
As the review of the literature via PUBMED showed that only 28 breast carcinoma patients with pancreatic metastasis whose tumors were mostly of lobular phenotype, due to the limited number of patients reported, a standard treatment could not be determined in terms of favorable outcome. Contributing such case reports or series to the literature would prove useful to establish a standard approach for the treatment of those patients.
Most importantly, this case emphasizes the importance of being more perceptive in terms of finding the origin of metastatic cancer with a multidisciplinary approach, especially when the clinical course of a patient progresses worse than that of expected response under already ongoing treatment protocol.
Footnotes
Ethical approval
Informed consent of the patients relatives was obtained prior to the writing of the manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
No code available.
Funding
The authors received no specific funding for this work.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [Zekiye Küçükoğlu Geneş], [Osman Sütcüoğlu], [Berkay Şimşek], [Güldal Esendağlı], [Ahmet Özet]. The first draft of the manuscript was written by [Zekiye Küçükoğlu Geneş], [Osman Sütcüoğlu], and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.