
Abstract
Mammogram is the standard imaging modality for the early detection of breast cancer, and it has been shown to reduce disease-related mortality by up to 30%. Mammogram, however, has its limitations. It is reported that 10–30% of breast cancers may be missed on a mammogram. Delay in the diagnosis and treatment may adversely affect the prognosis of patients with breast cancer. We present a case of multifocal invasive early breast carcinoma, which was misinterpreted twice as intramammary lymph nodes, thus resulting in a delay in diagnosis for eighteen months. The tumors were detected incidentally after the patient presented to our Breast clinic for symptoms related to a concomitant benign lesion involving the same breast. We describe the tumors’ imaging features and discuss the possible reasons that likely led to repeated misinterpretation. Awareness of possible causes for missed breast cancer is necessary to avoid delay of treatment initiation that may adversely affect prognosis.
Introduction
Mammography is the standard imaging modality for the early detection of breast cancer that has been shown to reduce disease-related mortality by up to 30% [1,2]. The mammogram, however, has its limitations. Its sensitivity to breast cancer detection varies from 68–92% in most studies [3], whereas it has been reported that 10–30% of breast cancers may be missed at mammography [4,5]. About 10–15% of breast cancers are, however, mammographically occult and will not be detected on a mammogram [1]. Many missed cancers are retrospectively visible on prior mammograms [6] and were either overlooked or misinterpreted as benign lesions [7]. The interpretation errors may be attributed to factors related to the patient, the lesion itself, or technical and reader factors [7]. We present a case of multifocal invasive early breast carcinoma, which was misinterpreted twice as intramammary lymph nodes within eighteen months. We discuss the tumors’ imaging features and the possible reasons that likely led to the misinterpretation.
Case presentation
A 67-year-old woman presented to our Breast Clinic with a 3-week history of spontaneous bloody discharge from the right nipple.
Physical examination confirmed a single-duct bloody discharge from the right nipple, whereas the remainder of the physical examination was unremarkable.
The mammography, which had been performed two months earlier at another institution, had revealed a dense breast with the presence of two small nodules in the upper outer quadrant of the right breast. The mammographic appearance was the same in the previous mammogram that had been performed eighteen months before (Fig. 1). In both mammographic and ultrasonographic evaluations, the two nodules had been interpreted as intramammary lymph nodes. Unfortunately, no previous (before eighteen months) mammogram was available for review.
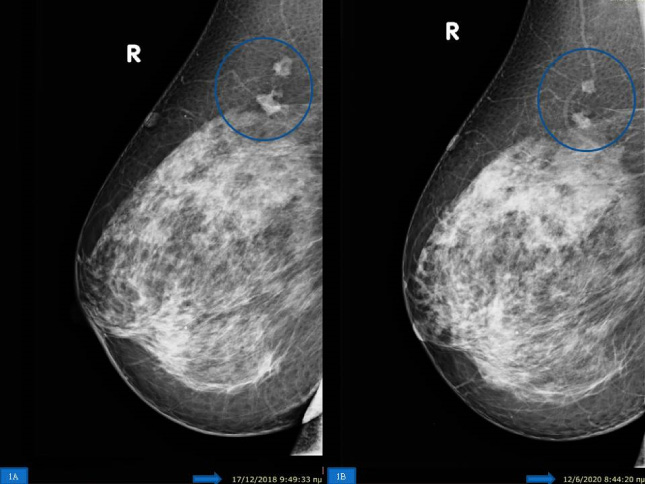
Right mediolateral (MLO) mammogram showing two nodules in the upper outer quadrant without any change for a period of eighteen months.
A spot compression magnification view was performed that revealed irregular borders of the two nodules (Fig. 2), whereas focused ultrasonography exhibited imaging findings highly suspicious for malignancy (Fig. 3). Following spot compression magification and ultrasonography the imaging characteristics were classified as BIRADS category V, and a Magnetic resonance imaging (MRI) was then performed which was indicative of multifocal malignancy in the upper-outer quadrant of the right breast. An ultrasound-guided core needle biopsy revealed breast adenocarcinoma in both nodules. A total mastectomy and sentinel node biopsy was performed. Histopathological examination of the specimen revealed two ductal invasive adenocarcinomas, measuring 1.5 cm and 0.8 cm respectively, of grade II according to the Bloom-Richardson grading system. On immunohistochemical evaluation, the tumor cells stained positive for ER and PR receptors, whereas the expression of HER2 was negative, and the ki-67 proliferation index was 13–15% (Fig. 4). A third tumor consisting of pure DCIS and measuring 1.5 cm, was also found. Two sentinel nodes were negative for metastases. A subareolar intraductal papilloma measuring 0.8 cm was also found, which was the cause of the bloody nipple discharge. The patient started endocrine treatment with an aromatase inhibitor and is currently well with no evidence of recurrence seven months after surgery.
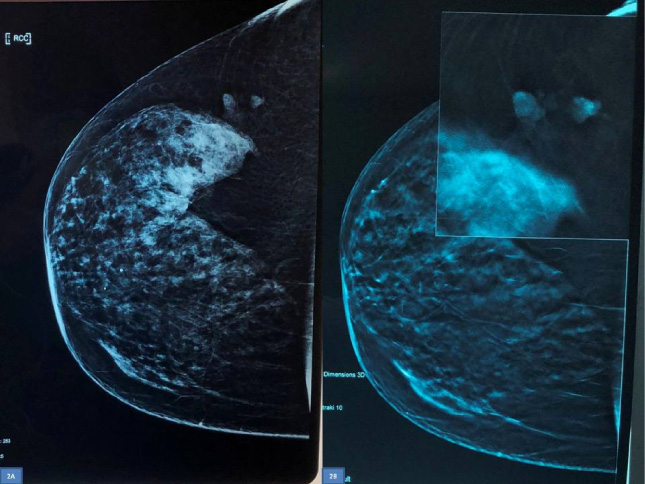
Right craniocaudal (CC) mammogram showing the nodules (2A). Spot compression tomosynthesis showing irregularity of their borders (2B).
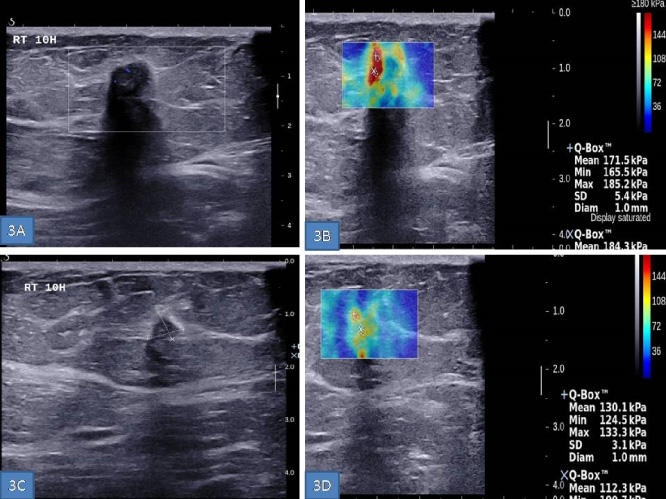
On focused ultrasonography, both nodules appeared as hypoechoic masses with irregular margins, desmoplastic reaction, acoustic shadowing, and high elasticity index on share wave elastography.
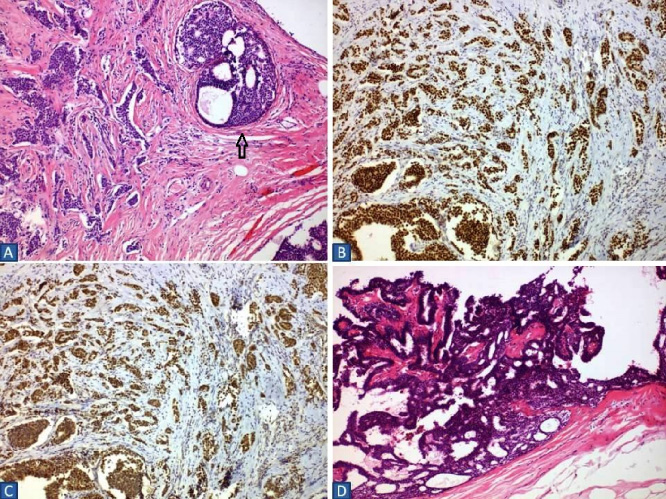
(4A) Photomicrograph showing invasive breast carcinoma. Tumor cells are of medium size, with eosinophilic and clear cytoplasm and nuclei quite atypical, often with eosinophilic nucleus and moderate mitotic activity. Associated DCIS is also evident (arrow). (H&E, ×100). (4B) Tumor cells stained strongly positive for ER (×100). (4C) Tumor cells stained weakly positive for PR (×100). (4D) Intraductal papilloma consisting of branching fibrovascular cores lined by columnar epithelial cells with round or oval nuclei and sufficient eosinophilic cytoplasm, without mitotic activity. Focal epithelial hyperplasia is also evident. (H&E, ×100).
The diagnostic and subsequent treatment delays adversely affect the prognosis in breast cancer patients [3]. There are several reasons why breast cancer may go unnoticed at the mammogram, such as dense breast parenchyma that obscures the tumor, perception errors, interpretation errors, subtle signs of malignancy, slow growth of the tumor, poor technique, and poor positioning [4,8]. In general, a breast cancer diagnosis may be missed due to tumor-related factors, as well as perceptual and interpretation errors.
Tumor-related factors represent the most common cause of missed breast cancer [9]. Tumor-related factors include cancers with subtle signs, very small cancers, cancers with well-circumscribed margins, such as mucinous and papillary carcinomas, focal asymmetric densities due to invasive lobular carcinomas, areas of architectural distortion, and diffuse nature of the lesion [4,9,10].
Perceptual and interpretation errors may occur due to several factors such as deficient training, lack of expertise, presence of an obvious finding, subtle features of the tumor, poor viewing conditions, inattention, fatigue, and distraction [3]. Low-grade carcinomas, as in our patient, may not exhibit obvious changes between consecutive screenings and may therefore go undetected [4].
The use of double reading, additional mammography views, ultrasonography, MRI, digital breast tomosynthesis (DBT), and spot compression magnification can improve diagnosis [2,4,9].
The double reading strategy can increase the detection rate of breast carcinoma by up to 15% [4,7], whereas the distance from the screen display may play a role in missing breast cancer at a mammogram [11].
The correlation between mammography and ultrasonography is essential for the diagnosis of lesions located within a heterogeneous background [10] and dense breast tissue [12]. However, suspicious mammographic findings should be further investigated even in the presence of a lesion that exhibits benign ultrasonographic features [1].
Spot compression magnification of a relatively well-circumscribed mass, as seen in our case, may reveal small areas of irregular margins or microlobulations, requiring therefore further evaluation [4].
DBT is an adjunctive imaging tool for further evaluation of the breast, with a 30% higher cancer detection rate when used in combination with digital mammography [13]. Breast cancer may, however, be missed with both techniques [14].
In the case presented herein, the two small carcinomas were misinterpreted twice as intramammary lymph nodes at another institution during the past eighteen months. Intramammary lymph nodes represent one of the most common benign findings on mammography, with a variable incidence of up to 48% of the mastectomy specimens [15,16]. Although they can occur in any portion of the breast, they are most commonly found in the upper outer quadrant [5,16]. On mammography, intramammary lymph nodes represent well-circumscribed oval or lobulated nodules with radiolucent hilum measuring less than 1 cm in diameter, whereas on ultrasonography they may appear as nodules with smooth or lobulated margin, hypoechoic cortex, and echogenic central hilum [5]. They do not exhibit changes in size in comparison to previous mammograms [15]. In rare cases, as in our patient, early small invasive breast carcinomas may mimic intramammary lymph nodes on mammography [17].
In our patient, the two small carcinomas were misinterpreted twice as intramammary lymph nodes, most likely because in the past 18 months they did not exhibit any change in consecutive mammograms. In the retrospective review of the mammogram performed 18 months before, the nodules had subtle signs of malignancy which went unnoticed, resulting likely in the misinterpretation of the two small breast cancers as intramammary lymph nodes. When a digital spot compression magnification was performed during the patient’s current presentation, highly suspicious signs were noted, and the malignancy was evident in the subsequent focused ultrasonographic and MRI evaluation. Additionally, the histological and immunohistochemical analysis revealed low-grade carcinomas, explaining probably why the tumors didn’t undergo any noticeable change between the two screenings. Our patient presented for a symptom that was not directly related to the carcinomas but was due to another concomitant benign lesion.
Radiologists should be aware of the subtle findings of breast cancer [12]. Comparison with prior examinations is essential to identify subtle changes such as parenchymal asymmetries, architectural distortions, microcalcifications, enlarging masses, and lymph nodes [18]. Studying the imaging features of missed cancers is necessary for the radiologist to identify potential factors that may lead to missed breast cancer [6].
Conclusions
Awareness of potential causes of missed breast cancers is necessary, and a thorough search for masses with subtle signs of malignancy on a mammogram is mandatory. Any breast nodule that is supposed to represent an intramammary lymph node, should be carefully assessed for minimally suspicious signs. Implementation of a double reading strategy is associated with a reduction of missing breast cancers. Further imaging evaluation with spot compression magnification views, digital tomosynthesis, focused ultrasonography, or MRI is necessary to avoid missing early breast cancers.
Disclosure of interest
The authors report no conflict of interest.