
Abstract
INTRODUCTION:
The management of complex cysts of the breast is an ongoing topic of discussion. The aim of this study was to determine the prevalence of underlying malignancy in radiologically diagnosed complex cysts, and to assess whether watchful waiting could be the preferred method to safely manage complex cysts of the breast.
SUBJECTS AND METHODS:
A single-center retrospective study was performed between May 2003 and November 2019 in the VieCuri Medical Centre. Women with a radiologically diagnosed complex cyst of the breast were included. Prevalence of underlying malignancy was calculated, as were absolute risk reduction and number needed to treat in order to diagnose malignancy. In addition, patient characteristics were compared to determine characteristics associated with malignancy.
RESULTS:
Of 78 radiologically diagnosed complex cysts of the breast, five (6,4%) were found to be malignant. The number needed to treat was calculated at 12,8 (absolute riks reduction 0,078). Age (P = 0,003) was associated with malignancy.
CONCLUSION:
Complex cysts of the breast could be managed more conservatively. Patient characteristics can be used to assess the eligibility for radiological follow-up. This, in turn, would lead to a lower NNT and possibly a decrease in disease burden and healthcare costs.
Introduction
The past decades have shown rising awareness of breast cancer. Breast cancer is diagnosed through breast imaging (i.e., mammography and ultrasonography) [1]. The increased use of breast imaging has resulted in frequent identification of (incidental) benign-appearing lesions. Among these so-called benign-appearing lesions are the frequently encountered cystic breast lesions.
These lesions of the breast can be classified according to The American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS) lexicon into uncomplicated cysts, clustered microcysts, complicated cysts and complex cystic and solid masses [2]. The prevalence of complex cysts is reported between 3,1% and 5,1% in previous literature [3,4]. These complex cysts are associated with a variety of pathologic diagnosis [5]. Furthermore, complex cysts are assumed to have a chance of being malignant. In previous studies, underlying malignancy was reported in 0,0% to 50,0% of radiologically diagnosed complex cysts [3,4,6–15]. For that reason, complex cysts are often classified as BIRADS 4 lesions and therefore a pathological sample should be obtained [5]. Because of the disadvantages of a biopsy, this frequently means surgical excision of the cyst. Not only does a biopsy cause the cyst to collapse, making the lesion difficult to find afterwards on radiological evaluation. A (cytological) biopsy is also prone to sampling errors.
However, most of the previous studies are outdated and therefore one may question if these percentages are still accurate with today’s improved radiologic techniques. Due to these improved techniques, the chance to find an underlying malignancy in radiologically diagnosed complex cysts may be much smaller. Meaning that surgical excision of radiologically diagnosed complex cysts could be over-treatment. In addition to this, the Dutch breast cancer guidelines state a complex cyst may be classified as a BIRADS 3 lesion if benign hallmarks are more present than malignant hallmarks [16]. This suggests a more conservative approach to complex cysts may be suited. Therefore the aim of the present study is to assess the percentage of malignancy in radiologically diagnosed complex cysts of the breast and to determine whether watchful waiting would be the preferred method to safely manage complex cysts of the breast.
Materials and methods
The study was approved by the institutional review board of the VieCuri Medical Centre, Venlo, The Netherlands.
Patients
In this retrospective study, women with the radiological diagnosis ‘complex cyst’ between May 2003 and November 2019 in the VieCuri Medical Centre, The Netherlands, were included. A search of radiology reports of the breast (ultrasonography, mammography, 3D tomosynthesis, computed tomography and magnetic resonance imaging) was performed in the hospital’s electronic patient system (HiX Productie 6.1, ChipSoft B.V., Amsterdam, The Netherlands). This search identified a total number of 147 radiology reports describing complex cysts in 119 patients. After selection using the criteria described in Fig. 1, 82 radiologically diagnosed complex cysts in 80 patients were included.
Baseline characteristics which are, according to the Dutch breast cancer guidelines, associated with an increased risk of developing breast cancer (i.e., menopausal status, age, history of breast disorders), were obtained from the electronic patient system [16]. The use of anticonceptives entailed both oral anticonceptives as hormonal intrauterine device. Family history was considered positive when at least one family member in the first or second degree had a history of breast, ovary, or prostate cancer. Patients could present themselves at the outpatient clinic through referral by a healthcare professional or the national breast screening program, or the patient was already in follow-up for another breast disorder. Lesion palpability and mastodynia were noted. Other clinical symptoms at the moment of presentation entailed any of the following symptoms: nipple discharge, nipple deformity, skin changes, or itching. The presence of microcalcifications in the lesion was noted, as were the presence of large calcifications or cystic lesions in the ipsilateral breast.
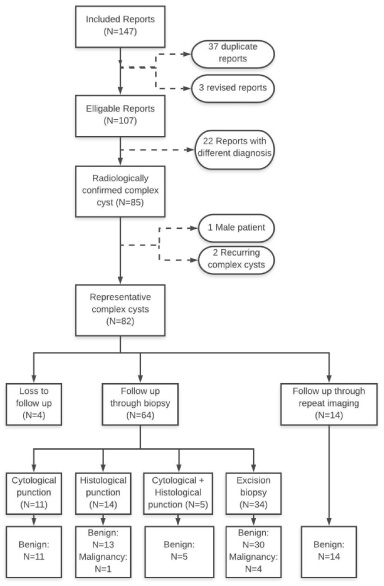
Inclusion flowchart.
In this study a complex cyst is defined as a cyst with a thick outer wall, thick internal septa or both, intracystic solid mural lesions, or a complex mass containing both cystic and solid components. Radiological diagnosis was based on ultrasonography, mammography, 3D tomosynthesis, computed tomography, magnetic resonance imaging, or a combination of these methods. Using these methods a BIRADS classification is assigned using the guidelines [2]. Pathological sampling was obtained by fine-needle aspiration (FNA), core needle biopsy (CNB), surgical excision, or a combination of these methods. For lesions which were first in follow-up but biopted later on, the original BIRADS classification was used.
For each biopsy procedure informed consent was acquired by the performing radiologist. Based on clinical presentation and imaging, the performing radiologist decided, in collaboration with the surgeon, on the method of biopsy or to follow up the patient radiologically. In addition, surgical excision was done in case of an inconclusive biopsy.
Analysis of the pathological samples was performed by an experienced pathologist. Cases with inconclusive or malignant diagnosis were discussed in the multidisciplinary meeting. Definitive diagnosis was based on the pathological sample or repeat imaging of the complex cyst.
Statistical analysis
The baseline characteristics were compared to determine significant differences between complex cysts with an underlying benign and malignant diagnosis, using univariate analyses. Adjustments for multiplicity were performed using the Bonferroni correction. Comparison according to age was done using the Mann-Whitney U test, and median and interquartile range (IQR) were used instead of mean and standard deviation so as to describe the range of age of the groups more representatively. Comparison of menopausal status, use of anticonceptives, patient history, family history, clinical presentation, and the presence of secondary radiological findings was done using Fisher’s exact test. Referring authority, BIRADS classification, and lesion size were compared using the Chi-square test. In categories with missing data the valid percentages were used.
Absolute risk reduction (ARR) and number needed to treat (NNT) were calculated. MedCalc Statistical Software version 16.4.3 (MedCalc Software b.v., Ostend, Belgium) and SPSS software (IBM SPSS Statistics version 24.0, Chicago, IL, USA) were used for statistical analysis. P < 0,05 was considered statistically significant (p < 0,0036 after Bonferroni correction).
Results
Eighty-two radiologically diagnosed complex cysts in 80 patients were included (Fig. 1). Four cases were lost to follow-up. In two of the cases the patients withdrew from further follow-up. In the other two cases the patients underwent a mastectomy for other reasons. In 14 cases (17,9%) follow-up took place through repeat imaging. No malignancies were found in these cases. In 64 cases (82,1%) the diagnosis was based on biopsy. Thirty-four of the 78 patients (43,6%) underwent surgical excision biopsy for definitive diagnosis. As shown in Table 1, five of the 78 radiologically diagnosed complex cysts turned out to be malignant (6,4%). In one case malignancy was diagnosed by CNB, in four of the cases by surgical excision (in two cases excision was performed initially, in two cases after inconclusive CNB). In 73 cases (93,6%) the lesion was benign. In only nine cases (12,3%) the definitive diagnosis was a complex cyst. In 31 cases (42,5%) an uncomplicated cyst was the definitive diagnosis. In the majority of the cases (N = 56, 71,8%), mastopathic changes were seen in the biopsy, although patients may have had multiple diagnoses upon pathological examination.
Definitive diagnoses in radiological complex cysts (N = 78)
Definitive diagnoses in radiological complex cysts (N = 78)
*Patients that underwent pathological sampling may have had multiple diagnoses.
Baseline characteristics of benign versus malignant definitive diagnosis
Values are median and interquartile range (IQR) and number (percent). Valid percentages were used in categories with missing data. A: Mann-Whitney-U test; B: Fisher’s exact test; C: Chi-square test.
Women with an underlying malignancy were significantly older than their counterparts with a benign diagnosis (P = 0,003). Other clinical features such as the use of anticonceptives, a history of malignancies of the breast, cystic lesions of the breast, breast surgery, a positive family history of breast cancer, or the presence of a palpable lesion, mastodynia or other clinical symptoms were not associated with an underlying malignancy. The referring authority was also not associated with an underlying malignancy. Radiological features such as BIRADS classification, lesion size, and the presence of microcalcifications, cystic lesions or larger calcifications were not associated with an underlying malignancy. Malignant lesions were in general smaller than benign lesions (80% < 20 mm) and were mostly (80%) classified as BIRADS 3 lesions (Table 2).
When comparing patients with a definitive benign diagnosis based on radiological follow-up with those that received pathological sampling, significant differences were seen (Table 3). Patients with radiological follow up had a significantly lower BIRADS classification (P = 0,001) when compared to patients with pathological sampling.
Baseline characteristics of pathological sampling versus radiological follow up
Values are median and interquartile range (IQR) and number (percent). Valid percentages were used in categories with missing data. A: Mann-Whitney-U test; B: Fisher’s exact test; C: Chi-square test.
Comparing patients with complex cysts that received radiological follow up with those that received pathological sampling, the ARR was calculated at 0,078. The NNT was calculated at 12,8.
The present study has shown that only five of the 78 radiologically diagnosed complex cysts (6,4%) were malignant. Age and postmenopausal status were the only clinical features associated with underlying malignancy. The NNT was calculated at 12,8, meaning 12,8 patients need to undergo pathological sampling in order to diagnose one malignancy [17].
Hypothetically, transferring patients from the pathological sampling group to the radiological follow-up group would have a direct effect on the NNT by exponentially lowering it. This indicates that the efficiency of the follow up of complex cysts could be improved by these transfers. Although 12,8 is an acceptable NNT for the diagnosis of breast cancer, it still means 11 patient underwent biopsy unnecessary. Therefore, if lowering this number is safely possible it should at least be considered. Identifying characteristics associated with malignancy could assist clinicians in assessing the eligibility of a patient for radiological follow-up. In this study, age was identified to be associated with malignancy, which is congruent with the results of previous studies [4,13]. In this study no radiological features associated with malignancy were identified, although several previous studies showed size of the lesion and the presence of both microcalcifications and large calcifications to be associated with underlying malignancies [3,4,12,13]. However, it is remarkable that all malignancies in the current study were found in the pathological sampling group. Therefore, one may wonder if there truly were no radiological features involved in the decision to perform pathological sampling.
Because of the retrospective character of the study, only patients with radiologically diagnosed complex cysts were included. Therefore, it was not possible to calculate sensitivity and specificity of the radiological test. However, by including all radiologically diagnosed complex cysts and not only pathologically diagnosed complex cysts, this sample does give an accurate image of the prevalence of underlying malignancies in all complex cysts. Despite the long follow-up of the current study, only a small sample of 78 cases is presented due to the low prevalence rate of complex cysts. However, the sample size of this study is comparable to the sample sizes of multiple previous studies [3,4,8,10,12,14]. In this study excision of the complex cysts was performed in 34 cases (43,6%), which is also comparable with previous studies [3,4,9,10,12,13]. The reproducibility of imaging acquisition and interpretation were not evaluated, we solely relied on the radiological reports. Although the BIRADS classification is steadily used, the application of the BIRADS score to complex cysts does present some difficulties, and inter-observer differences were noted. This can be explained by the fact that the implementation of the BIRADS classification was not as widespread and adhered to at the start of the inclusion period in 2003. This also demonstrates a major disadvantage of the BIRADS classification: it is prone to overestimation by only giving the breast the score of the most suspicious lesion.
The current trend in management of complex cysts is leaning towards the acquisition of pathological sampling. This is often rationalized because of the relatively high prevalence of underlying malignancies in the complex cysts. However, as suggested in a review by Houssami et al., there may be an overestimation of malignancy associated with complex cysts [18]. This seems to be congruent with the results of the current study, with a malignancy prevalence of 6,4%. This is notably lower than previously reported (median: 25,0%) [3,4,6–15].
Based on these results we believe that radiologically diagnosed complex cysts could be managed more conservatively by using patient characteristics (i.e. age and menopausal status) to assess the eligibility for radiological follow-up. This, in turn, would lead to a lower NNT and possible decrease in disease burden and healthcare costs.
Footnotes
Acknowledgements
The authors would like to thank Shannon Dieltjes and Lars Roks for their contribution in the assembly of the dataset and Frits van Osch for his contribution in the statistical analysis.
Conflict of interest disclosure
No conflict of interest was reported by the authors.