
Abstract
OBJECTIVE:
Description of breast pathology in adolescents.
METHODS:
A retrospective descriptive study of adolescents who were referred to the Gynecology consultation of a tertiary pediatric hospital for suspected breast pathology, in the period from the 1st June 2011 to the 30th December 2018.
RESULTS:
One hundred and two female adolescents (11 to 18 years old) with suspected breast pathology were referred (6% of the motives for consultation), with confirmation in 58 (56.9%), who were included in the study. The reasons for referral were breast masses (66%), anomalies in breast size or symmetry (29%) and infection (5%). Of breast masses, the most frequent diagnosis was fibroadenoma (76%), followed by fibro-cystic pathology (18%). In most cases, a conservative approach was chosen, with clinical and imaging surveillance. Surgery was required in 29% of these cases. Anomalies in breast size and symmetry were observed in 17 adolescents. Two adolescents were submitted to symmetrization, after 18 years of age. Infectious and inflammatory pathology occurred in three cases: two mastitis and one retroareolar cyst. The approach consisted mainly of antibiotherapy. There were no cases of malignant breast disease.
CONCLUSION:
Lumps or breast masses are the most frequent breast pathology in adolescence, and in the majority of cases surveillance was recommended, as they are a mere sign of hormonal oscillations at this age. Objective examination and/or breast ultrasound are usually enough to make the diagnosis. The approach must be mainly conservative, since malignancy is extremely rare in this age group.
Keywords
Introduction
Breast pathology in adolescence is rare and mostly benign. Despite this fact, it is likely to cause anxiety in the patient and their family, due to the fear of breast cancer. However, only 0.02% of breast masses excised in adolescents correspond to breast carcinomas [1]. It is essential to know the normal development and also have the ability to recognize breast lesions, for a correct diagnosis in this age group. Breast lesions can be categorized as developmental abnormalities, inflammatory or infectious conditions and breast masses. In assessing breast pathology in this age group, a detailed clinical history and objective examination is required. Ultrasound is the gold standard for diagnosis, due to its high accuracy and absence of ionizing radiation [2]. The majority of the conditions that affect teenagers are self-limited and do not require therapy. In addition, a conservative approach is always preferable, in order to avoid injury to the developing breast tissue.
In this study, we review breast pathology in adolescence, namely the incidence, diagnostic procedures and therapeutic approach.
Materials and methods
Retrospective descriptive study of female adolescents, aged between 10 and 18, who were referred to the gynecology consultation of a tertiary hospital for suspected breast pathology, from the 1st June 2011 to the 30th December 2018. The constitution and manipulation of the database, as well as the statistical analysis were performed using the SPSS program version 23. A descriptive analysis of the distribution of patients was carried out, considering various sociodemographic variables. Categorical variables are presented as frequencies and percentages and continuous variables as means and standard deviations or medians and interquartile ranges. The test for normal data distribution was performed using the Shapiro-Wilk test or by analyzing the values of skewness and kurtosis.
Results
In the period studied, 1635 female adolescents were referred to the Gynecology consultation. One hundred and two were suspected of having breast disease (6%). This diagnosis was confirmed for 58 of them (56.9% of the total and 3.5% of consultations), who were included in the study. The rest (44) were clinically evaluated in consultation and, after excluding breast pathology, were redirected to primary health care, where they will maintain surveillance.
The average age of the group included in the study was 15 years old (SD 1,738). The age distribution is shown in Graphic 1. All were in the post-menarche period. This occurred at a median age of 12 years (IQR 1).
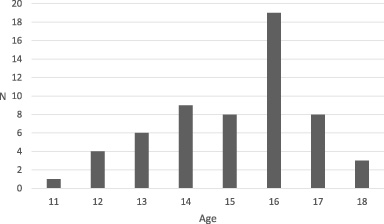
Age of patients.
The medical history is shown in Table 1. Since the consultation was carried out in a tertiary pediatric hospital, most children have associated comorbidities, with 45% of the sample being healthy. 24% had a family history of breast pathology.
Medical history
aAccording to International Classification of Primary Care-2.
The reasons for referral can be seen in Graphic 2.
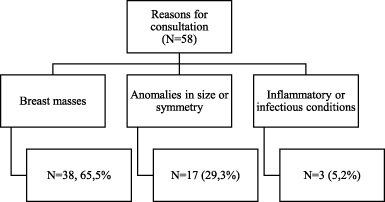
Diagnostic categories.
The breast masses found in this study, as well as the chosen therapy, are listed in Table 2. The majority affected the right breast (53%). On objective examination, it was found that all were unilateral and mobile, with an average size of 3 cm (SD 1,152). They were mainly single lumps (87%) and had a preferential location in the upper outer quadrants of the breast (31%).
Lumps/breast masses
Breast ultrasound was performed on adolescents who reported mass growth in the last few months, associated symptoms or where there were doubts about the objective examination regarding the consistency of the nodules (cystic versus solid). It was performed on 32 adolescents (84%). Assessment of imaging findings were based on the Breast Imaging Reporting and Data System (BI-RADS).
An example of a solid and cystic mass can be seen in Figs 1 and 2, respectively.
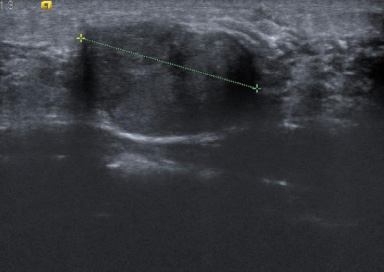
Breast ultrasound revealing a solid, well-defined, hypoechogenic nodular formation, probably related to fibroadenoma, in the lower and inner quadrant of the left breast, measuring 26.8 mm.
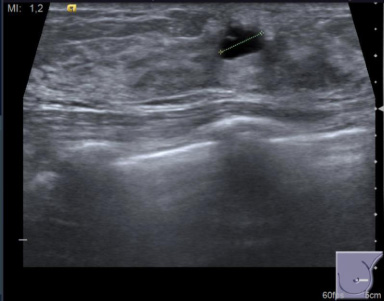
Breast ultrasound revealed a cyst of anechogenic content of the left breast, with a 9 mm greater axis.
Four adolescents underwent biopsy (10,5%). The criteria for biopsy were an increase in mass size, associated symptoms or a larger axis greater than 3 cm.
Surgical treatment was performed on 11 patients (28,9%): 1 patient had histological changes on the biopsy, which justified surgical excision (benign phyllodes tumor); 2 had lumps with a greater axis greater than 4 cm; 5 had lumps with a size greater than 3 cm and due to the anxiety of the patient and her caregivers preferred surgical excision; and the remaining 3 reported growth or associated symptoms (mastalgia).
Of all breast masses, the most frequent diagnosis was fibroadenoma (76%), immediately followed by fibrocystic changes (18%). The cysts were approached conservatively, with clinical and imaging surveillance, with no cases of excision. The patient with a benign phyllodes tumor was kept under clinical control, with no recurrence.
Inflammatory or infectious pathology
Anomalies of breast size and symmetry were observed in 17 adolescents, 12 cases of breast asymmetry, 3 of hypotrophy and 2 tuberous breasts. All had normal body mass index. Among the adolescents with breast hypotrophy, one had a history of neurological pathology, epilepsy and myasthenia gravis. The remaining were healthy. The approach consisted mainly of clinical surveillance (88%). Two adolescents with breast asymmetry were submitted to symmetrization surgery, after 18 years of age.
Inflammatory or infectious pathology occurred in 3 cases (Table 3). Physical exam showed unilateral involvement in all cases, preferably on the right side, with associated inflammatory signs. Ultrasound was performed in all patients, having diagnosed an abscess and an inflammatory retroareolar cyst (Fig. 3). The approach consisted mainly of oral antibiotics. None of the patients required hospitalization or surgical drainage. All of these cases were resolved with a conservative approach.
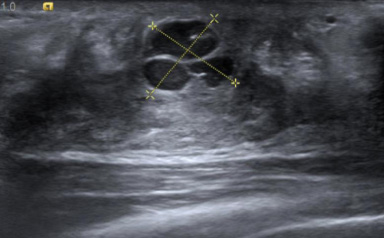
Breast ultrasound: there is an increase in the thickness of the right retroareolar mammary glandular tissue with an increase in the reflectivity of the subcutaneous adipose tissue and a 15 × 14 mm multiloculated liquid collection, which contains content with some suspended echoes, changes of a likely inflammatory/infectious nature.
The totality of patients included in the study, given the particularity of the age group, continued to be followed up in our consultation until adulthood (18 years).
Breast development is a hallmark of puberty and, therefore, the main changes in the breast occur during this period. The prevalence of breast pathology in adolescence is unknown. In this study, it was found that breast disease affected 3.5% of the adolescents referred to our consultation. As expected, the totality of cases corresponded to benign conditions, as the probability of cancer in this age group is extremely low [3]. Breast masses were the most frequent disorder in adolescents (66%). However, there are other possible causes of breast pathology in this age group, mostly self-limited [4].
Fibroadenoma and fibrocystic changes correspond in our study to 76% and 18% of the masses, respectively. Fibrocystic changes seem to be associated with an abnormal imbalance between estrogen and progesterone levels [2]. The therapy was expectant, although some authors recommend the administration of anti-inflammatory drugs or oral contraceptives for symptomatic improvement. Persistent cystic lesions can be submitted to aspiration, although this technique is rarely necessary in adolescents [5]. Fibroadenomas are the most common masses in adolescents, representing 30 to 50% of the total, in medical series, and 44–94% in surgical series [6,7]. These data correspond to our findings. They are characteristically asymptomatic, well-circumscribed and mobile masses. Its preferred location was the upper and outer quadrant, in accordance with the literature [8]. These masses can be diagnosed clinically. The approach to fibroadenomas generally consists of clinical and/or imaging surveillance, as most of it regresses and may even disappear [9]. In the diagnostic approach to a breast mass, imaging studies may be necessary to differentiate cysts from solid lumps. It should also be performed whenever this mass persists for several months or if there are associated symptoms. Breast ultrasound is preferred in this age group, due to increased breast density. It’s also not recommended because X-rays on the breast at this very young age is deleterious, and should not be performed. Thus, mammography is not recommended for the assessment of breast masses in adolescents. In the evaluation of imaging findings, the Breast Imaging Reporting and Data System (BI-RADS) was used. However, this evaluation system is not used frequently in pediatric age, as it aims to categorize diseases according to the potential for malignancy, which is rare in this population. Most breast lesions in adolescents are categorized as 2 (benign) or 3 (probably benign). Therefore, they usually only require regular follow-up [10]. Biopsy can be performed for diagnostic confirmation [11]. In our institution, it is performed whenever it has a diameter greater than 3 cm. It should also be performed in case of a family history of breast cancer, namely BRCA mutations, or if the adolescent had chest radiation in childhood. Excision is indicated if there is growth of the mass, if it is larger than 4–5 cm or whether there is associated pain [7]. In this study, 29% of adolescents with breast masses underwent surgery. The anatomopathological study revealed a case of phyllodes tumor and one of sclerosing adenosis. The phyllodes tumor is rare and usually affects older women. However, cases have been reported in adolescence. It can be classified based on the histological characteristics of the stroma. Most are benign, as it was found in this case [12]. The recommended therapy is surgical margin-free excision. The recurrence rate is around 10% [13]. During this study period, there were no recurrences. Sclerosing adenosis is a lobular lesion with increased fibrous tissue and intercalated gland cells. The risk of breast cancer is low and therefore no therapy is needed [14]. In this study, there was a case of sclerosing adenosis, whose form of presentation was a breast mass, having been surgically removed due to a progressive increase in its dimensions on ultrasound.
The anomalies in breast size and symmetry observed in this study were breast asymmetry, hypotrophy and tuberous breasts. Hypotrophy of breast tissue usually occurs secondary to weight loss, due to chronic diseases or eating disorders. In this study, most patients were healthy and none had a decreased body mass index. The tuberous breast is a variant of breast development, in which the base of the breast is limited and the nipple and areola are more developed. There were two cases in this study. The etiology is unknown. Breast asymmetry is a frequent complaint in adolescence, being more pronounced between Tanner stages 2 and 4. Despite improving with complete breast development, 25% of women maintain some degree of breast asymmetry [15]. An expectant approach to changes in breast development is preferable until complete development occurs, around 18 years old. If there is no breast growth and the woman is not satisfied, referral to Plastic Surgery may be necessary for eventual mammoplasty [16]. Two adolescents with breast asymmetry underwent surgery.
Mastitis in adolescents results from infection of the skin or the introduction of bacteria into the ductal system. It is more likely during puberty, when major changes and breast growth occur [8]. The underlying cause may be ductal obstruction or ectasia, immunosuppression or nipple injury. The diagnosis of mastitis is usually made clinically. The most frequent clinical features were swelling, erythema, warmth, tenderness, and induration of the breast. When the infection is deeper, it can cause an abscess. Staphylococcus aureus is the most common microorganism [17]. Breast ultrasound aided in the diagnosis of breast abscess. Empirical oral antibiotics should be performed during 7 to 10 days Surgical drainage may be necessary in case of an abscess [18]. However, there was no need in any of the cases in this sample. Inflammatory cysts respond more slowly to therapy and may persist for weeks or months.
As previously mentioned, breast cancer is rare in adolescents, with no case reported in this study. However, this diagnostic hypothesis must always be considered when making a differential diagnosis.
Lumps are the most frequent breast disease in adolescence, and in most cases are indicated for surveillance, as they are nothing more than the reflection of hormonal oscillations at this age. Clinical examination is usually sufficient to make the diagnosis. There was no case of malignant breast disease. The approach to breast pathology in adolescents is mostly conservative, with surgical indication reserved for well-defined situations.
Footnotes
Disclosure statement
The authors declare that they have no conflicts of interest related to this work.
Funding sources
The authors declare that there are no sources of financing.