
Abstract
BACKGROUND:
The present era of individualized treatment for breast cancer is influenced by the initial disease status including the anatomical extent, grade, and receptor status. An accurate preoperative staging is the basis of treatment planning and prognostication. Our study aims to determine the discordance between the preoperative clinical and the postoperative pathological stages of breast cancer patients.
METHODOLOGY:
The medical records of all non-metastatic breast cancer patients from January 2017 to December 2018 who underwent upfront surgery were reviewed. They were staged as per the eighth AJCC and the concordance between the clinical (c) and pathological T (tumor), N (nodal), and final AJCC stage was studied. A Chi-square test was used to determine factors that significantly correlate with disease discordance.
RESULTS:
A total of 307 breast cancer patients were analyzed. Among these, 43.3% were hormone receptor-positive, 30.6% were Her2 positive and 26% were triple-negative. Overall stage discordance was seen in 48.5% (n = 149) patients (upstaging in 22.1%, downstaging in 26.4%). The discordance rate was 48.9% for T stage (cT versus pT) and 57.4% for N stage (cN versus pN). Among patients with clinically node-negative disease, 53.4% were found to have positive nodes on histopathology, while 27.2% had vice versa. Overall, the factors associated with upstaging were ER-positive, Her2 positive and triple-negative status (all p < 0.05), while none of the factors showed significant association with downstaging.
CONCLUSIONS:
About half of breast cancer patients had discordance between clinical and pathological staging with higher discordance in the nodal stage. This changes the disease prognosis, and may also affect the offered surgical treatment and radiotherapy. Thus highlighting the need for a precise pre-operative staging. Also, this information will aid clinicians in discussions with patients, keeping in mind the likelihood of change in disease staging and management.
Introduction
Breast cancer is the most common cancer of women in India [1]. The treatment of breast cancer has evolved from the Halsteadian era of total mastectomy to breast conservation surgery with an important role of chemotherapy, hormonal therapy and radiation therapy [2]. The better understanding of tumor biology, prognostic and predictive factors in breast cancer have resulted in individualizing the treatment strategies for a patient. The recent AJCC staging includes not only the anatomical extent of the tumor but also grade, hormonal receptor status and gene expression assays whenever available to determine the final stage of the disease.
Till the early 20th century, mastectomy was the standard of care for breast cancer and by the 1970s, the role of breast conservation surgery (BCS) with radiotherapy emerged as an important alternative [3]. The early era of chemotherapy began with its use post-surgery to eliminate the microscopic disease. Fisher and Mamounas in 1995 conceived the idea of neoadjuvant chemotherapy (NACT), which led to randomized control trials and proved the significance of preoperative therapy in reducing the size of primary tumor and increasing the number of BCS [4]. Hence, the current management of breast cancer is a multidisciplinary approach with discussion on various treatment options like the use of breast conservation surgery (BCS) versus mastectomy, sentinel lymph node biopsy (SLNB) versus axillary lymph node dissection (ALND), and neoadjuvant therapy versus upfront surgery. To decide on the right modalities and their proper sequencing, there is a need for a meticulous pre-operative staging, lack of which would lead to missing the opportunity of using a treatment that could confer improved quality of life outcomes.
Discordance between preoperative and postoperative staging has been studied for various malignancies like renal cancer [5], NSCLC [6], endometrial cancer [7]. However, there is a lack of such data for breast cancer. In this study, we aim to determine the discordance rates between the clinical and pathological staging of breast cancer and the effect of various parameters on the likelihood of discordance.
Materials and methods
All female patients diagnosed with stages I–III invasive breast cancer from January 2017 to December 2018 at our institute were retrospectively identified. The patients who underwent upfront surgery were included for the analysis. The patients whose data lacked information on grade, hormone receptor status, and clinical staging (if operated at outside centers) and those with bilateral breast cancer or inflammatory breast cancer were excluded. All the patients included in the study had undergone investigations to rule out metastatic disease. Other pre-operative imaging like mammography, ultrasonography findings were noted. Clinical staging was based on physical examination and imaging. For pathological staging, the pathologist at our institute reviewed all the surgical specimens, including the patients who underwent surgery elsewhere. The approximate number of pathologists involved in the reporting process was 5.
The tumor size (pT), number of positive lymph nodes, total nodes identified, and extracapsular extension was recorded. The grade and receptor status was determined on the surgical specimen. Estrogen receptor (ER), and progesterone receptor (PR) status were defined based on the Allred scoring with positivity defined as a sum of three and above. Her-2 testing was done by immunohistochemistry (IHC) followed by in-situ hybridization (ISH) for an equivocal score. All the patients were staged based on eighth AJCC prognostic stage groups for this analysis.
The clinical T (tumor) and N (node), stage group and pathological T, N, stage group were considered concordant if the clinically determined stage remained the same after pathological assessment. Among discordant staging, the upstaging and downstaging was separately recorded (upstaged - pathological stage > clinical stage, downstaged - pathological stage < clinical stage).
Descriptive and inferential statistical analysis was carried out using the statistical software namely SPSS 22.0. Chi-square and Fisher Exact test were used to identify factors associated with upstaging or downstaging versus concordance. The studied parameters included ER, PR and Her2 receptor status and grade.
Results
Patient characteristics
A total of 307 female patients with upfront surgery for invasive breast cancer were analyzed after excluding the cases with inadequate data. The median age was 47 years (Range 22–86 years). All the patients presented with a breast lump except three patients; two presented with axillary swelling and one with nipple discharge. The median duration of symptoms was 3 months (Range 2 days–3 years). Education status showed more than half of the patients were illiterate. The majority of patients (95.7%) had invasive ductal carcinoma (IDC) and more than half (61.5%) had Grade 3 diseases. The pre-operative mammography and ultrasound of involved breast were available for 84.1% of patients (excluding those who had T4 disease as mammogram was not done for some of these patients because it would be a painful procedure), while all patients had contralateral breast imaging that was normal. The most common stage at presentation was stage III (63.5%) while only 14.3% of patients had stage I disease (stage IA-1.3%, stage IB- 13%). Sixteen (5.2%) patients had breast conservation surgery with axillary dissection and remaining had modified radical mastectomy (MRM). About 13% of patients underwent surgery elsewhere and had received adjuvant treatment at our center. The majority of patients were hormone receptor-positive (43.3%) followed by Her2 positive (30.6%) and triple-negative (26%). Other clinical and disease characteristics are detailed in Table 1.
Table showing clinicopathological details of patients
Table showing clinicopathological details of patients
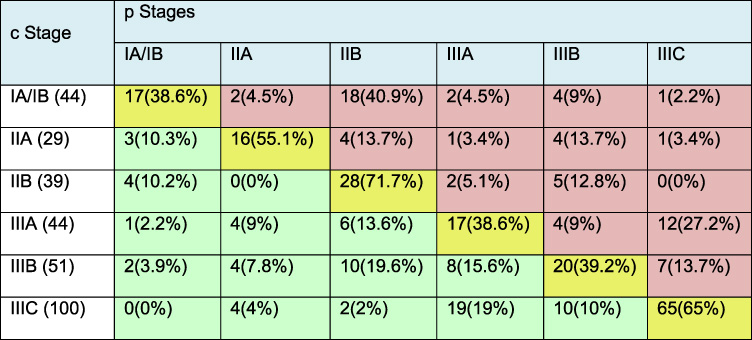
It shows the change in clinical to pathological stage for each stage group in our study population. The yellow shade represents the concordance, red represents upstaging and green shade represents downstaging for each stage group. c – clinical stage, p – pathological stage
Overall stage discordance was seen in 48.5% (n = 149) patients with upstaging in 22.1% and downstaging in the remaining 26.4% of patients. For the “T” stage, the clinical and pathological discordance was 48.9% (upstaged - 9.4%, downstaged - 39.5%) and “N” stage showed a slightly higher discordance rate of 57.4% (upstaged - 39.7%, downstaged - 17.7%). The nodal status was more commonly upstaged, while the tumor size was mostly downstaged in the pathological staging (Fig. 1).
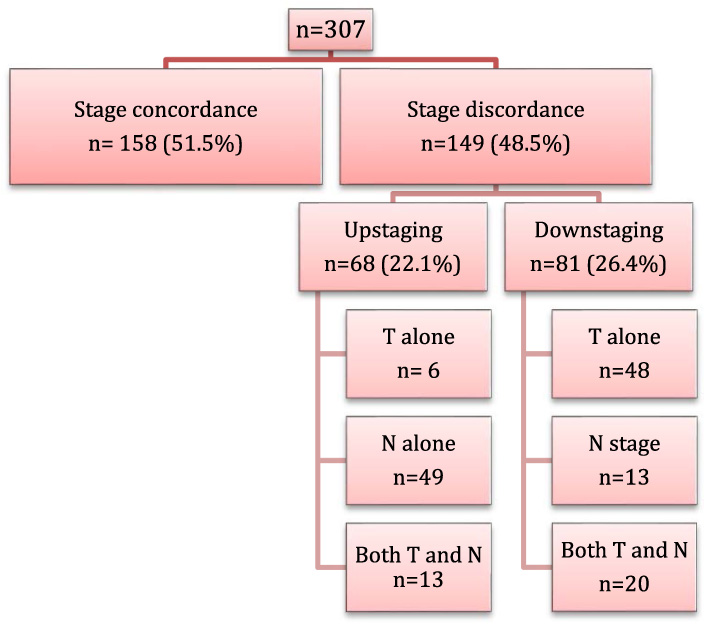
Flowchart showing the concordance and discordance rates for the entire study population. It also shows the separate contribution of the T and N stage in stage discordance.
There were 61.2% (n = 71) of cT3 patients downstaged to pT1/T2. The decrease in tumor size in the surgical specimen compared to the clinically noted T size was expected as during clinical measurement the surrounding edema and non-invasive component can’t be differentiated. Among patients staged clinically as node-negative, 53.4% (n = 70) were reported to have positive nodes on pathological evaluation, while among patients with clinically positive nodes, 27.2% (n = 46) did not show any disease on histology. Extracapsular extension was seen in 50.2% (n = 100/199) of node-positive disease.
There was a variation in concordance among different stage groups with the highest rates noted for Stage IIB (71.7%) and least for Stage I and IIIA (38.6%) (Table 2). Eight patients (5.8%) were upstaged to Stage IV post-operatively as they were found to have pathological T4 or N2/3 disease and underwent further evaluation with CT chest, abdomen, and bone scan that revealed metastatic disease. However, for analysis, only their T and N stage were compared.
Based on the receptor status, ER-positive (p = 0.005), Her2 positive (p = 0.04) and triple-negative (p < 0.001) tumors were associated with upstaging (versus concordance). Grade and PR status did not show any significant association. None of the factors showed any significant association with downstaging (versus concordance).
Breast cancer management has evolved over time to include a multi-modality approach, which has resulted in improved outcomes. The identification of molecular markers and subtyping based on hormonal receptor status, Her2 expression and gene expression assays has made breast cancer management a more individualized treatment. Improvements in surgical techniques, like breast conservation surgery and sentinel lymph node biopsy, have resulted in decreased morbidity. Thus, in the current era, all breast cancer patients should be adequately staged initially to understand the disease burden, prognosticate and devise a treatment strategy.
We sought to evaluate the gap between the clinical staging of breast cancer that guides the treatment plan and the final pathological staging that may influence the pre-discussed prognosis and therapeutic requirements. Our study was a retrospective study in a developing country with over 50% of patients illiterate and about 60% patients presenting with stage III disease. About 15% had no mammograms or ultrasounds during staging investigations. MRI and needle biopsies or FNAC, though not always useful, were not performed. Only 16 (5.2%) had lumpectomy, while the remainder had mastectomy. All patients underwent axillary lymph node dissection and no sentinel nodal biopsies were performed. In our study, we found that 48.5% of breast cancer patients who underwent upfront surgery had discordance between the clinical and pathological staging.
A study by Plichta et al. [8] has very well brought out the wide gap between the preoperative clinical staging and final pathological staging and how it affects the survival outcomes. They showed a discordance rate of 31.8% with 23.1% being downstaged, 8.7% being upstaged, and better survival outcomes for former compared to the latter group of patients. These discordance rates are lower than the rates observed in our study. This can be because of differences in the pre-operative investigations. About 15% of our patients (excluding T4 disease) did not undergo involved breast mammography and ultrasound, so their T stage was purely based on clinical examination. Many a times, for a patient planned for MRM, oncologists tend to skip involved breast mammography, as it is unlikely to add further information. Also, for 13% of patients, initial evaluation and surgery took place at non-oncological centers, where resources would have been limited and the examination might have been done by a non-oncologist, thus precluding clinical staging comparable to the western study population. A study by Kumar and Bhaskar, though conducted on a small number of patients, found that 24.5% of breast cancer patients were under-investigated [9]. This highlights the gap that exists between the trial based recommendations and the practical applications of the same in a developing country.
Physical examination is the most important aspect of clinical staging, but investigations like mammography and ultrasound augment the examination findings leading to more accurate clinical staging. MRI can be used as an adjunct to above imaging to improve assessment of primary tumor especially in suspected multifocal or multicentric disease, dense breast tissue, and invasive lobular histology. Boetes et al. compared different imaging modalities to look for the discrepancy in tumor size with histological analysis. They found that T size was underestimated with mammography (by 14%) and USG (by 18%) and not significantly different from MRI findings [10]. However, MRI is not routinely practiced in many countries because of added cost and lack of availability. Schalkwyk et al. tested the accuracy of clinical examination with histopathology of the surgical specimen. They included clinical assessment by a senior breast surgeon and found 68.6% concordance in T stage and 50% positive predictive value (PPV) and 83.6% negative predictive value (NPV) for axillary lymphadenopathy [11]. We reported 51.1% concordance for T stage and PPV and NPV for lymphadenopathy was 73.7% and 47% respectively. Thus, our study is also in agreement with their conclusion of the need to correlate examination and imaging findings to facilitate accurate preoperative staging. Using ultrasound and biopsy/FNAC for axillary staging is recommended by AJCC. It is essential in early breast cancer patients to decide between sentinel lymph node sampling and axillary dissection during the surgical process. USG has a PPV of 69%, and NPV of 86%, thus a valuable tool for staging a cN0 breast cancer patient [12]. Another study reported that in combination with FNAB, PPV and NPV is increased to 100.0% and 69.8% respectively [13].
A change in the stage of breast cancer has a significant impact on its management in the present era of precision medicine that includes treatment escalation and de-escalation based on the patients’ disease characteristics. Thus, we bring out the question that whether, as an oncologist, are we undermining the importance of pre-operative staging? Among the patients that were staged clinically as node-negative, 53% showed disease in the nodes on pathological evaluation. This was much higher than the 18% reported by Plichta and colleagues. As per the NCCN guidelines [14], this changes their treatment plan with the addition of locoregional radiation after adjuvant chemotherapy. Also, if the nodal burden is high with extracapsular extension (ECE), the radiation oncologist will need to include the axilla in the radiotherapy field. A study by Hetelekidis et al. showed ECE in one-third of operated patients. It correlated with disease burden in the axilla and was associated with a reduced DFS (disease-free survival) on univariate analysis [15]. The presence of ECE was one of the indications for axillary RT in our study and the incidence was 50% among node-positive patients. This increases the risk of lymphedema for the patients [16]. In cases with clinical node-positive disease, NACT can be considered upfront to reduce nodal burden, avoid axillary irradiation and to offer BCS with SLNB in selected cases. The meta-analysis by Pathak et al. has shown an increased breast-conservation surgery rates with NACT [17]. The role of neoadjuvant therapy has further widened with significance of pathological complete response (pCR) that can be a surrogate for PFS and OS (in certain subtypes) [18] and the role of adjuvant therapy in patients with residual disease.
Over one-fourth of the patients who were clinically node-positive turned out to have pathologically node-negative disease. They underwent ALND that can lead to complications like lymphedema, restriction of movement, numbness and pain [19]. BCS with SLNB would have been an adequate option for few of these patients [20]. Various meta-analysis has emphasized on improvement in the quality of life, better outcomes in body image with breast conservation surgery [21]. This stresses the need for proper pre-operative nodal staging using ultrasound and FNA. A systematic review on use of ultrasound for predicting a non-palpable axillary node involvement reported moderate sensitivity of 49% to 87% for size, 26% to 76% for morphology and 31% to 63% for ultrasound-guided biopsy with a high specificity of 100% [22]. Even with new imaging modalities, there is still a void in imaging for most accurate nodal staging. Also, the use of these investigations may not be feasible as routine practice in high volume centers because of cost and availability. It requires a judicious use of resources for improved cancer care.
Overall, the numbers of BCS in our country are much lower compared to western counterparts because of a larger proportion of patients presenting with locally advanced disease [23]. However, we believe there is a subgroup of patients that is not undergoing BCS due to a lack of accurate preoperative staging. We sometimes omit a detailed staging workup since most of our patients undergo upfront MRM. In the present era, improving the quality of life is an important aspect of cancer treatment; therefore the morbidity of each treatment modality should be considered. The option of downstaging, conservative surgeries, limited field of radiation therapy should be contemplated and certain minimum investigations should be done for breast cancer management. Also to the extent possible, maximum patients must be treated in dedicated Oncology centers.
There is also a likelihood of change in treatment due to upstaging to stage IV as we found in 5% of our patients. This doesn’t mandate upfront metastatic workup for all patients except those with stage III disease [24]. But a clinician needs to be aware of the likelihood of upstaging, as it will change the disease prognosis, patient counseling and plan of management.
The tumor biology is today an integral component of breast cancer staging. Plichta et al. demonstrated its association with stage discordance in their study. They showed that ER negative was associated with stage concordance and Her2 negative status was associated with upstaging and downstaging, while in our study ER positive, Her2 positive and TNBC was associated with upstaging and none of the factors were associated with downstaging.
Our study limitations include those associated with a retrospective study. Some patients were excluded from the study that lacked complete information on hormonal receptor status and grade of tumor. Second, the clinical staging was not done by the same oncologist for all patients and among those operated at non-oncology centers, the pre-operative staging may not be standardized and confirmed by a breast oncologist. The lack of uniformity would have affected clinical staging and thus concordance.
Conclusion
About half of non-metastatic breast cancer patients undergoing upfront surgery have discordance between their clinical and pathological stage, a much wider gap compared to the western series. This is a first-of-its-kind study reported from a developing nation where few centers cater to a large population stretching their limited resources for providing the best possible care to maximum number of patients. This makes it difficult to ensure uniformity in adherence to international guidelines and recommendations. However, in breast cancer disease where the treatment has been continuously evolving to improve outcomes with minimal possible morbidity, the importance of accurate clinical staging cannot be overstated. Our study particularly highlights how crucial it is to assign the correct nodal stage with the best possible investigation before planning for upfront surgery in breast cancer as it affects the complete planned treatment strategy and prognosis. This information will aid clinicians to be aware of the likelihood of both disease upstaging and downstaging and discuss the same with their patients to emphasize detailed workup before assigning the best possible treatment protocol.