
Abstract
Fever is a common feature in various pathological conditions that manifests a series of molecular events in the internal milieu. Much less attention has been paid to the clinical importance and the management of fever in breast cancer patients. However, several studies have reported an association between postoperative fever and poor treatment outcomes in breast cancer patients. The fever is a side effect of chemotherapy and a manifestation of cancer recurrence. The postmenopausal breast cancer patients experience another body temperature disturbance that is known as a hot flashes. Here, we reviewed the literature regarding postoperative fever and the possible underlying molecular and cellular mechanisms. Then the efficacy of non-steroidal anti-inflammatory drugs was discussed as a therapeutic option to control postoperative fever. Finally, we reviewed the chemotherapy-induced neutropenic fever and cancer vaccination-induced fever.
Introduction
The global incidence of breast cancer (BC) has been increasing last decades [1]. The BC treatment and the quality of life improvement are two critical issues for scientists and healthcare practitioners [2]. There are reports that showed the BC postoperative fever is associated with poor patient’s outcome and a shorter overall survival. The BC patients with natural or treatment-induced menopause experience the body temperature disturbance that is known as hot flashes [3]. Hot flashes reduce the quality of life in the BC patients [4]. Therefore, the monitoring of the body temperature is a desirable goal that promotes the overall survival and the quality of life in the BC patients. There are concerns about some challenging issues. The first is the differential diagnosis of body temperature disturbance because the BC patients experience the conditions other than fever. The second is the comprehension of possible underlying mechanisms because fever is a defense tool and an alarm signal against a pathologic condition while the underlying molecular events may lead to cancer progression [5,6]. Third is the simultaneous management of fever and underlying events, which is critical to improve the survival rate and the quality of life.
As well as, the fever is the common side effect of cancer vaccination and immunotherapy that may affect the treatment outcome. Chemotherapy induces the neutropenia (NP) and neutropenic fever (NF) which are associated with a higher mortality rate in the BC patients. The costs and efficacy of adjuvant therapy to overcome these challenges is another critical issue in breast cancer treatment.
To the best of our knowledge, there is no review article on the fever importance in the BC. Therefore, we discussed the issue regarding the importance and challenging aspects of fever in BC especially the postoperative fever (POF), chemotherapeutic agents-induced NF (NF) and vaccine induced-fever in detail.
History
Chawla et al.’s study is a pioneer work on the fever development in the BC patients, which showed that the fever is the first manifestation of the cancer recurrence and metastasis [7]. The findings of this study was confirmed by Drenth et al. who reported the fever, rash, and arthritis as the common sign and symptom of BC metastasis [8]. As well as, Reiman et al. showed that BC gastrointestinal metastasis leads to bleeding and fever simultaneously. They concluded that gastrointestinal tract bleeding and further fever may be a biomarker for diagnosis of BC metastasis [9]. On the other hand, in the most cases of BC who suffer from anemia, the red blood cell distribution width is changed and may consider as a biomarker [10]. Hence, metastasis-induced bleeding probably induces anemia and fever simultaneously.
Recently, Takada et al. reported a male case with a 67-year-old man with BC who referred to hospital with fever and pain. The patient has suffered pancreatic cancer and gynecomastia. Regardless of the primary source of breast cancer, once again the fever is introduced as a BC metastasis symptom [11].
Postoperative fever
BC therapy is a complex process and the treatment is dependent on cancer subtype, cancer stage, age, etc. However, in the most cases, a combined multidisciplinary approach is applied that including surgery, radiotherapy and systemic chemotherapy [12]. The surgery is a key step in the treatment of operable BC, which usually is used as the first-line therapy [13]. BC surgery has physical, psychological and social side effects [14]. Postoperative fever (POF) is one of the most common physical problems, which is observed after a surgical operation. Some studies have showed that the POF associated with cancer recurrence, treatment failure and poor overall survival. The POF is defined as a temperature higher than 38.3 degrees Celsius (101.3 degrees Fahrenheit) after surgery where patients experience it in a different severity, duration and time [15]. Based on the fever onset time, POF could be classified into early and delayed forms. The early POF initiates within 48 h after surgery and has non-infectious etiologies such as surgical trauma induced-inflammation, dehydration, the side effects of anesthetic drugs, etc. While, infection causes to delayed POF that appears about 3–5 days after surgery [16].
The extend surgical operation, or inappropriate anesthesia procedure or any other mis-care may display itself as an alarm or as a signal that it is fever. Two publications have investigated the possible role of POF on BC pathogenesis. Teucher et al. performed a retrospective study on 378 patients with primary BC with different stages and showed that the POF occurs in 45% of the patients including stage I 41%, stage II 45%, stage III 59% and stage IV 50% [17]. They found a significant association between POF and BC recurrence [17]. In another study, Yan et al. have reported that POF contributes in the node negative BC relapse. Kaplan Meier overall survival analysis showed a higher risk of recurrence in the patients who experience early POF [18]. Yan et al. introduced POF as an independent prognostic factor for overall survival and concluded that the changes in the host milieu may mediate the POF- induced cancer recurrence. The POF also was reported in the breast mastectomy in the male patients. Piggott et al. introduced an obese 15-year-old male patient with hypogonadism who underwent mastectomy due to gynecomastia that the patient has experienced a bilateral pulmonary emboli leading to POF [19]. In addition, it should be noted that the BC patients receive radiotherapy as a treatment regime after surgery that commonly leads to bronchiolitis pneumonia and may induce the fever in the BC patients [20]. Nevertheless, Huang et al.’s study showed that fever was not developed in inflammatory form of BC, a rare and aggressive BC subtype [21].
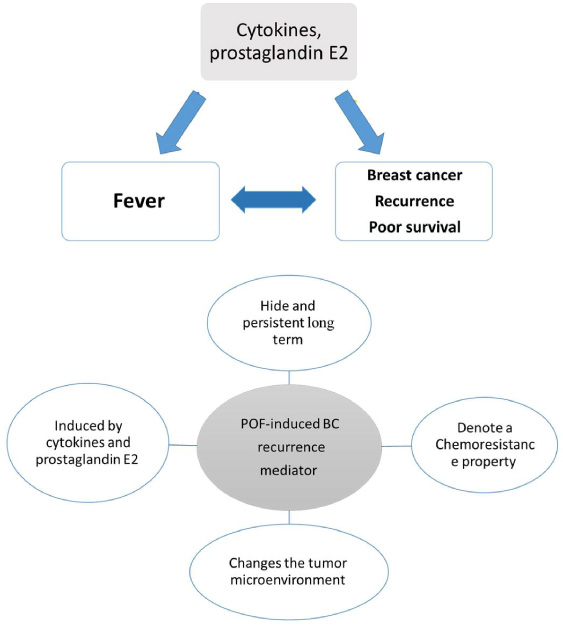
Fever, breast cancer reoccurrence, cytokine-prostaglandin E2 triangle; four properties of postoperative fever induce-cancer recurrence.
In general, POF etiology ranged from inflammation, the side effect of drugs to the life threatening necrotizing soft-tissue infection. The timing of POF may be helpful in the differentiation of the potential etiologies. Early POF occurs during the surgery or up to 1 hour following it and usually is caused by inflammatory factors [16]. In 80% of early POF cases, there is no infection in first few days after surgery [22]. In addition to trauma, other aspects of surgery can induce the host inflammatory response that including anaesthetic medication, analgesic drugs, hypothermia, blood loss, transfusion, pain and perioperative distress [23,24]. All of these may be involved in the POF development. Inflammation and pro-inflammatory cytokines are proposed as the underling molecular mechanisms of early POF and further POF-related shorter survival in the BC patients.
There is a controversial debate for POF-induced BC recurrence; it is not sensible that a short-term body temperature elevation (the fever) causes to cancer recurrence at long term because early postoperative fever disappear within few days but cancer recurrence occurs at least 1-3 years after the treatment. We propose that fever is a bystander event and there are other actors, which mediate the recurrence in the long term. What is the the main underlying mechanism? The main mediator is located in one angle of a triangle where the others is BC recurrence and the fever. This mediator should has several properties: first, the mediator should be a persistent factor and stow itself away for long time; second, the mediator should denotes a chemoresistance property to the cancer because the BC patients receive chemotherapy after surgery; third, the mediator should be induced by cytokines and prostaglandin E2, the main fever upstream players. Fourth, the mediator should change the tumor microenvironment in order to increase BC recurrence. See the Fig. 1 and the schematic representation of the triangle.
Cell senescence
Based on aforementioned criteria, we suggest cell senescence as a ultimate underlying mechanism. Pro-inflammatory cytokines have mutual role between fever and BC recurrence. Mettler et al. evaluated the effects of BC surgery on the expression of cytokines in the peripheral blood cells by focussing on the surgical methods. The results showed that serum pro-inflammatory cytokines are elevated in first day after surgery [25]. As a result of the overexpression of pro-inflammatory cytokines,surgical trauma induces POF. The elevated pro-inflammatory cytokines exacerbates the tumor microenvironment [26]. The pro-inflammatory cytokines are switched to a downstream mediator, prostaglandin E2, which affects brain hypothalamic temperature control center [27]. The cytosolic phospholipases A2 and cyclooxygenase-2 (COX-2),re the key enzymes are involved in the catalysis of prostaglandin E2 production. These enzymes are regulated by phosphorylation and transcriptional regulation, respectively. The elevation of pro-inflammatory cytokines and the fever result in prostaglandin E2 over-production [28].
The COX-2 overexpression and downstream prostaglandin E2 lead to cancer stem cell survival and proliferation[3]. The inter relationship between prostaglandin E2 and human breast cancer cells is well documented [4].
Some evidence showed that the non-steroidal anti-inflammatory drugs (NSAIDs), the well-known COX-2 inhibitors reduce the BC recurrence [29]. Therefore, pro-inflammatory cytokines and prostaglandin E2 is the first accused candidates of fever induced-BC recurrence. The changes of the cytokines and further prostaglandin E2 overproduction may affects the remained cancer and cancer stem cells. We suggest the cellular senescence as a underlying event at the cellular level that mediates the cancer recurrence ultimately. Cell senescence is defined as an irreversible cell cycle arrest with both oncogenic and tumor suppressive roles in the cancer pathogenesis [25]. It is rational that the cell proliferation and cell death (apoptosis, necrosis and other cell death type) could not mediate the cancer recurrence because cell death is associated with reduced-recurrence rate and do not running parallel to each other. While, the proliferative cells are targeted and eliminated by chemotherapy and the rest of the proliferative cells would promote the cancer recurrence more much more rapidly. In contrast, the cellular senescence denotes a chemoresistance feature to the cancer. The senescent cells remain metabolically active and contribute in the cancer recurrence and therapy resistance [25]. Sasaki et al. showed pro-inflammatory cytokines induce cellular senescence that is mediated via oxidative stress and the activation of ATM pathway [30]. The senescent cells have a secretory properties that exacerbates the tumor microenvironment in favor of cancer recurrence [31]. Figure 2 represents the possible mechanism molecular, cellular and physiological mechanisms of POF in BC pathogenesis schematically.
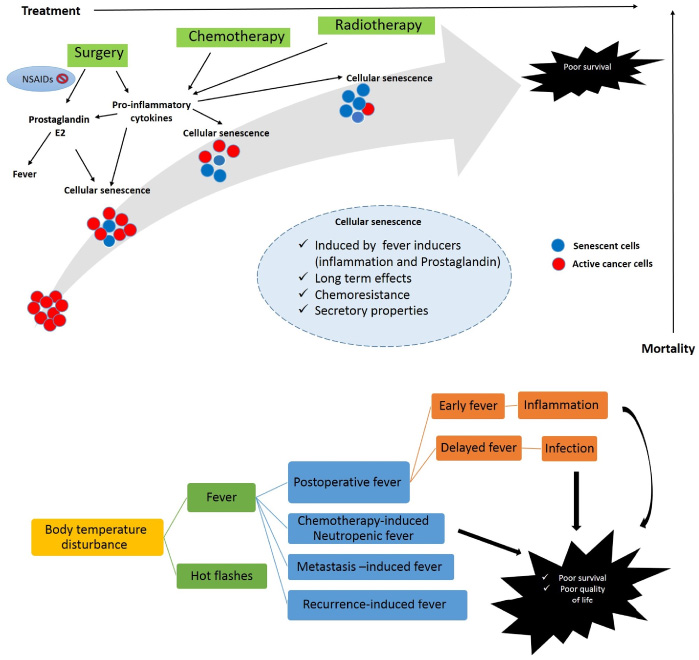
Schematic representation of the molecular mechanism of postoperative fever-induced cancer recurrence.
Narayan et al. summarized the principles of diagnosis and the management of POF and concluded that postoperative fever vary in its nature. The timing and analysis of infection biomarkers are necessary to rule out the life-threatening fever with infectious source [16]. Non-steroidal anti-inflammatory drugs or NSAIDs are common drugs that used as an analgesic and or antipyretic agents [32]. Literature review shows, NSAIDs have significant effects on BC cancer prevention and treatment but there is a controversy implying that NSAIDs efficacy is dependent on BC subtype and the administration time [33–36].
According to the current knowledge, it seems that NSAIDs prescription to pain alleviation and fever controlling, may mask the fever without amelioration and reversing the underlying molecular events [37,38]. The role of NSAIDs in the BC is homologous of antioxidant role in cancer pathogenesis. The consumption of antioxidants prevents cancer incidence before cancer initiation while it confers a chemoprotective feature during treatment [39]. A similar scenario has been observed for NSAIDs adminastration. A meta-analysis by Huang et al. showed that prescription of aspirin and NSAIDs after but not before diagnosis is associated with BC survival improvement [40]. Therefore, NASIDs may exacerbate the outcome of patients dependent on BC subtype and time of administration.
Neutropenic fever
Neutropenic fever (NF) is an important and common feature in the cancer chemotherapy. Several review articles discussed about NP and NF in the BC patients. There is a positive association between NF and the morbidity and mortality rate [43,46,47]. Although granulocyte-colony stimulating factor prophylaxis and other strategies are applied to control of NF but higher cost of drugs and poor recovery rate lead to disappointing outcome [43]. Therefore, NF prevention and management are crucial factors during therapeutic regime administration. Which drugs or which combined regime are able to induce the NF in the BC patients? The literature review showed, no original research has answered this question directly. While, during drug efficacy and safety analysis, the NF was reported frequently as a side effects. We summarized current knowledge about chemotherapeutic agent-induced NF in the Table 1. Generally, NP and NF are reported as a common side effect in about all chemotherapeutic agents. However the host immunologic condition, the drug regime types and administration protocols influence the rate of NP and NF significantly Table 1 show the NP and NF reports in the different drug regime that categorized into single, two-drugs and three-drugs regimes.
Chemotherapy and neutropenia and neutropenic fever, single, two and three drugs regime
Chemotherapy and neutropenia and neutropenic fever, single, two and three drugs regime
Mechanistically, bone marrow suppression in response to chemotherapy is responsible for development of NP and associated with higher mortality rate [48]. NP leads to higher infection risk and subsequent complications, which result in poor treatment outcome [47]. Fever is developed during either infection or non-infectious conditions. The infection has acute life threatening effects but non-infectious condition may promote the mortality rate in the long term. Fever may originate from chemotherapy induced-inflammation or NP per se [49]. Therefore, higher mortality rate may mediate by inflammation in a similar pattern as what was observed in the postoperative fever.
In some studies, reported the fever as a side effect of adjuvant and vaccine therapy. Co-treatment of the BC patients with G-CSF and MDX-210 (a combined antibody) induces the fever by production of IL-6 and TNF-alpha [50]. Trastuzumab safety assessment showed that the fever is the most common drug-related adverse events [51–54]. Keage et al. reviewed the trastuzumab efficiency and side effects and concluded that the most frequent adverse effects are fever and chills [55]. In phase- I clinical trial of survivin-derived peptide vaccine, the grade-I fever was observed when peptide is administrated with incomplete Freund’s adjuvant [56]. While, this vaccine has no adverse effect when is administrated according to other protocols. Prospective multicenter phase III clinical trial on pseudomonas jinanensis vaccine showed that the fever and local pain are the major adverse effects of the drug administration. The major adverse reactions of Pseudomonas Jinanensis vaccine prescription is fever in the BC patients and other malignancies [57]. Corynebacterium Parvum an adjuvant agent to the chemotherapy can induce the fever in the primary BC patients [58]. Dendritic cells vaccine and cytokine-induced killer cells injection is a immunocyte therapy that has several side effects such as insomnia, anorexia, joint soreness, skin rashes and ultimately fever, which is eliminated with antipyretic therapy [59]. TG1031 is a recombinant vaccine virus containing sequences coding of human MUC1 and the IL-2 that induces the moderate fever in the metastatic BC patients [60]. In another study, fever developed during co-administration of G-CSF and MDX-210, a product produced by linkage between fragments of HER-2/neu and Fc gamma [50]. The low-grade fever also was observed in stage III to IV of the BC patients after intramuscular injection of NeuGcGM3 in combination with outer membrane protein complex of Neisseria meningitides [61]. Taken together, fever is systemic adverse event following the vaccination-immunization and the cancer vaccination is not the exception [62]. The literature review shows pro-inflammatory cytokines are responsible for the fever development in the vaccine- immunotherapy. Manley et al.’s study and others demonstrated that acetaminophen and ibuprofen are effective medication to prevent the fever as the adverse reactions [63,64]. Therefore, the COX-2 enzyme and prostaglandins production seems to be the underlying molecular mechanism of vaccination induced-fever. As well as, vaccine-induced fever may affect the cancer vaccination outcome in a same way that what has been observed in the postoperative fever. Therefore, fever control and inhibition of underlying molecular events may increase the efficacy of BC cancer vaccination-immunotherapy.
Conclusion
In conclusion, fever is not proper biomarker for diagnosis of BC but it may predict the cancer recurrence and metastasis in the diagnosed patients. The postoperative fever and neutropenic fever is developed by two main life threatening underlying events including infection and inflammation and should be considered more seriously. The BC patients who receive chemotherapy or undergoes surgery exposed to higher infection risk and or inflammatory response that affects the treatment outcome and overall survival. It seem sensible that, before body temperature controlling by NSAIDs, the underlying molecular events be differentiated and be reversed by appropriate guidelines.
Footnotes
Acknowledgements
The authors would like to thank Urmia Branch of Islamic Azad University for the financial supports.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Author contribution
Shiva Mehran and Zafar Gholinejad reviewed the postoperative topics. Afshin Taravati, Esfandiar Baljani and Yousef Rasmi reviewed the other parts.