
Abstract
BACKGROUND AND AIM:
Traditionally lumpectomy as a part of breast-conserving surgery (BCS) is performed by palpation-guided method leading to positive margins and large excision volumes. There is no evidence suggesting that wide margin excisions decrease intra-breast tumour recurrence. Various perioperative techniques are used for margin assessment. We aimed to compare three commonly used techniques, i.e., ultrasound-guided surgery, palpation-guided surgery and cavity shaving for attaining negative margins and estimating the extent of healthy breast tissue resection.
METHOD:
A prospective comparative study was performed on 90 patients who underwent breast conservation surgery for early breast cancer between August 2018 and June 2019. Tumour excision with a minimum of 1 cm margin was done either using ultrasound, palpation or cavity shaving. Histopathological evaluation was done to assess the margin status and excess amount of resected normal breast tissue. Calculated resection ratio (CRR) defining the excess amount of the resected breast tissue was achieved by dividing the total resection volume (TRV) by optimal resection volume (ORV). The time taken for excision was also recorded.
RESULTS:
Histopathology of all 90 patients (30 in each group) revealed a negative resection margin in 93.3% of 30 patients in palpation-guided surgery group and 100% in both ultrasound-guided surgery and cavity shaving groups. Two patients (6.7%) from the cavity shaving group had positive margins on initial lumpectomy but shave margins were negative. TRV was significantly less in the ultrasound-guided surgery group compared to the palpation-guided surgery group and cavity shaving group (76.9 cm3, 94.7 cm3 and 126.3 cm3 respectively; p < 0.0051). CRR was 1.2 in ultrasound group compared to 1.9 in palpation group and 2.1 in cavity shave group which was also statistically significant (p < 0.0001).
Excision time was significantly less (p < 0.001) in palpation-guided surgery group (13.8 min) compared to cavity shaving group (15.1 min) and ultrasound-guided group (19.4 min).
CONCLUSION:
Ultrasound-guided surgery is more accurate in attaining negative margins with the removal of least amount of healthy breast tissue compared to palpation-guided surgery and cavity shaving.
Keywords
Introduction
Breast-conserving therapy (BCT) is defined as a surgical excision of the primary tumor and a margin of surrounding normal tissue followed by whole-breast radiation therapy (WBRT). BCT has now become the standard of care for early breast carcinoma with no significant difference in disease-free survival and overall survival compared with mastectomy [1,2].
The goals of BCS is to achieve local control of the disease and decrease local recurrence by obtaining disease-free margins at the final histological assessment as well as improving the cosmetic outcome by preserving healthy breast tissue.
Young age and involved margins are two most important predictors for local recurrences. Results of large meta-analyses suggest a twofold higher risk for local recurrence in patients with positive margins [3,4], whose rates extremely vary across literature, ranging from 20–40% [5], and re-excision or additional boost radiotherapy is considered for such patients [4,6].
The Society of Surgical Oncology (SSO) and the American Society for Radiation Oncology (ASRO) released guidelines in 2014, standardizing a negative margin after breast-conserving surgery (BCS) as “no ink on tumour” in patients with early breast carcinoma [7].
A recent meta-analysis showed that the re-excision rate after initial lumpectomy for invasive breast carcinoma declined significantly from 22 to 14% after publication of the SSO-ASTRO margin guideline [8,9].
Re-excision rate increases patient’s anxiety and incurred cost [10,11]. Effort should be made to further decrease the re-excision rate by perioperative margin assessment. Several perioperative margin assessment techniques such as gross examination of lumpectomy specimen, intraoperative specimen radiography, frozen section analysis, touch preparation cytology, cavity shaving margin and intraoperative ultrasound have been studied. Each technique has its merits and demerits [12,13].
Intraoperative pathological margin assessment technique includes imprint cytology and frozen section analysis, which has its own limitations. Firstly, it is labour intensive with decreased sensitivity of 65–78%. Secondly, it increases the duration of surgery thereby increasing the cost and, thirdly, it requires pathologist and cryostat machine on-site. There is also permanent loss of tissue for histopathological assessment [14,15].
Surgeons tend to overexcise healthy breast tissue, which result in large resections. A nationwide pathological study on surgical margins and excision volumes after BCS involving 10,058 patients reported one-third surgical failure rate when palpation-guided surgery was done as it exclusively depend on the tactile skills of surgeon [16,17].
Ultrasound-guided surgery helps excision of palpable breast carcinomas under direct visualization that result in a positive margin rate as low as 3–4% with significantly smaller resection volumes but requires the surgeon to be trained in using an ultrasound machine or that a radiologist be available in the operating theater for assistance [17,18].
Routine cavity shaving technique (all cut edges are shaved systemically after the excision of the primary tumour to remove any residual disease) reduces re-excision rate by 25–59% but may effect cosmesis due to increased resection of a healthy breast tissue [19–21].
Cosmetic outcome has been receiving increased attention in the past few years as it has a strong relation to the patients’ satisfaction and quality of life [22]. Approximately 30–40% of patients have unacceptable cosmetic outcomes following BCS, which is primarily due to resection of a large volume of healthy breast tissue along with the tumour [16,23,24].
Central excision of a tumour surrounded by a valid amount of healthy breast tissue should be the aim when performing lumpectomy for breast cancer. There is always an international debate on the surgical margin to be excised along with tumour. Less than 1mm margin is associated with 33.8% tumour involved margins [16]. However, there is no evidence that wide clear margins reduce local recurrences [4,7].
These results indicate that current surgical techniques and guidelines lack precision. An ideal perioperative procedure during BCS should avoid positive margins and decrease healthy breast tissue excision, which results in good cosmesis. Till date not many studies have prospectively compared more than two perioperative procedures together. The aim of this study is to determine which common perioperative procedure helps the most in attaining negative margins while resecting minimal amount of healthy breast tissue in patients with invasive breast cancer undergoing BCS.
Patients and methods
An approval from the Institutional ethical committee was obtained for conducting the study. The study population consisted of patients with early breast carcinoma diagnosed by fine needle aspiration cytology (FNAC) or core biopsy planned for BCS during August 2018 to June 2019 at Sri Shankara Cancer Hospital and Research Centre, Bangalore, India.
Exclusion criteria included clinically stage 3 and metastatic breast carcinoma, pre-operatively diagnosed duct carcinoma in situ (DCIS), presence of multifocal or multicentre tumours, use of wire-guided or radio-guided preoperative tumour localization, history of neoadjuvant therapy, previous surgical treatment or radiotherapy. Patients postoperatively diagnosed of invasive carcinoma with DCIS (i.e., unexpected DCIS) on histopathology were not excluded from the study. All patients provided their written informed consent.
Group size of 30 was decided based on previous records of the institution and patients undergoing BCS were allocated to any one of the three groups by computer generated random numbers. This was done till each group included 30 members. All patients and investigators were aware of study group assignments. The participating breast surgeons had a minimum 5-year experience in the field. A radiologist was also present in the operating theatre. The pathologist was blinded to which technique was used.
Procedures
The aim of ultrasound-guided, palpation-guided and cavity shaving surgery was to achieve complete tumour removal with gross healthy tissue margins of up to 1 cm. An optimum 1 cm margin was chosen arbitrarily based on previous studies [18,25,26].
Palpation-guided lumpectomy
Tumour excision was guided by the tactile skill of the surgeon in a standard manner. The index finger of the surgeon was used to palpate the mass, retract it and guide the dissection. The adequacy of the resection was based on the experience of the surgeon without objective imaging during the surgery.
Ultrasound-guided lumpectomy
Tumour excision was performed by the surgeon with ultrasound guidance in collaboration with an experienced radiologist using Philips CX 50 general imaging portable ultrasound machine with a linear probe with a frequency of 12-3 MHz. Before surgery, the radiologist carried out an ultrasound of the lesion. The tumour size, lesion-to-skin distance, and lesion-to-fascia distance was measured by the ultrasound. Dissection was guided by placing the ultrasound probe repeatedly in and around the wound at different angles to visualize the tumour margins continuously. After lumpectomy, an ex vivo ultrasound was performed to determine the accuracy of the complete tumour resection. The distance between the hypoechoic tumour edge and the resection margin was measured. If the distance was less than 1 cm, re-excision of the shave margin from the excision cavity was performed at the same time.
Cavity shaving technique
After palpation-guided lumpectomy, additional tissue resection was done. Superior, inferior, medial and lateral shave margins were mandated along with anterior and posterior margins if the resection had not extended to the dermis and pectoralis fascia, respectively. The volume of the cavity shaving was at the discretion of the surgeon, provided that the cavity shave margins encompassed the entire cavity.
According to SSO and ASCO guidelines “no ink on tumour” was considered as negative margins. All specimens were oriented with sutures. In patients showing positive margins, re-excision was performed. In the same session, axillary dissection/sentinel lymph node biopsy was performed for all cases while frozen section analysis was not done in any case. Postoperatively, patients received adjuvant systemic therapy and radiotherapy as per protocol.
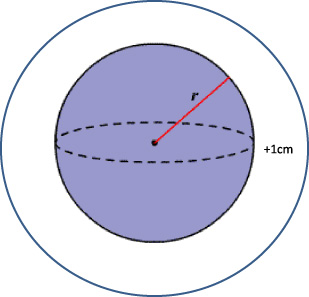
The tumour was defined as spherical. Optimal resection volume (ORV) calculated by formula 4∕3𝜋(r + 1 cm)3.
Tumour diameter and three dimensions of the surgical specimen were used to calculate the volumes. The tumour was defined as a sphere. An optimal resection volume (ORV) was calculated for each tumour as the spherical tumour (Fig. 1) volume plus a 1.0 cm margin of healthy breast tissue, calculated by the formula 4∕3𝜋(r + 1. 0 cm)3.
The total resection volume (TRV) was assumed to be ellipsoid (Fig. 2) and was calculated by the formula 4∕3𝜋(a ⋅ b ⋅ c) with a, b and c representing one-half of each of the three dimensions of the surgical specimen.
Calculated resection ratio (CRR) was defined to determine the amount of excess breast tissue resected and was calculated by dividing TRV by ORV (CRR = TRV/ORV).
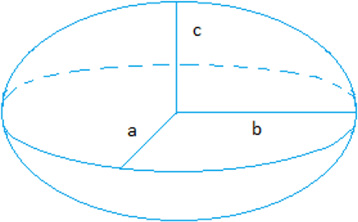
Specimen was assumed to be ellipsoid and TRV was calculated by the formula 4∕3𝜋(a
Excision time was defined in minutes as the time taken from the incision for lumpectomy to wound closure.
The primary outcome of the study was to compare the efficacy of ultrasound-guided surgery, palpation guided surgery and cavity shaving technique for obtaining negative resection margins. The secondary outcome was to estimate the excess volume of resection and excision time in all three groups.
The data were processed using the Microsoft Office Excel 2010 version and further analysed using STATA14.
For a descriptive analysis, the categorical variables were analyzed by using percentages and the continuous variables were analyzed by calculating mean ± SD.
For inferential analysis, The numerical data were analysed using ANOVA test and Kruskal–Wallis test in those cases that did not have a normal distribution, The categorical data were analysed using the chi-square test and p < 0.05 was considered statistically significant.
Results
Between August 2018 and June 2019, a total of 90 patients were enrolled in the study, 30 patients in each group. All three groups were well matched concerning demographic and clinicopathological characteristics (Table 1). The mean age of patients was 53.8 ± 11.2 years and the mean tumour size was 2.7 cm ± 0.9 cm. Unexpected Tumor-associated DCIS diagnosed on histopathological examination was present in 56 (62.2%) of 90 patients.
Patient and tumor characteristics
Patient and tumor characteristics
F = frequency, *p < 0.05 significant.
Table 2 shows the margin status of the three groups. Ultrasound-guided surgery group and cavity shaving group had a negative resection margin in all patients (100%). Two patients (6.7%) of the cavity shaving group had positive margins on initial lumpectomy but the shave margins were negative. 28 patients (93.3%) of the palpation-guided surgery group had negative margins. No statistical difference was observed between the three groups. Re-operation was done for the two patients in the palpation-guided surgery group with positive margins. DCIS was >1–2 mm away from the margin in all patients.
Margin status
*p < 0.05 significant.
Median ORVs, TRVs and CRRs of the three groups are shown in Table 3. Median ORV with a 1 cm margin was similar in all the three groups (44.6 cm3). TRV was significantly less in the ultrasound-guided surgery group compared to the palpation-guided surgery group and cavity shaving group. (76.9 cm3, 94.7 cm3 and 126.3 cm3 respectively; p < 0.0051). CRR was 1.2 in the ultrasound-guided surgery group compared to 1.9 in the palpation-guided surgery group and 2.1 in cavity shave group, which was also statistically significant (p < 0.0001).
The optimal resection volumes (ORVS), the total resection volumes (TRVS), and the calculated resection ratio (CRR)
Kruskal–Wallis test, *p < 0.05 significant.
Mean excision time was 13.8 ± 4.1 min in palpation-guided surgery group, which was statistically significant (p < 0.001) compared to 15.1 ± 2.4 min in cavity shave group and 19.5 ± 3.7 min in ultrasound-guided surgery group (Table 4).
Excision time
*p < 0.05 Significant.
BCT for early breast carcinoma is oncologically safe and is associated with improved cosmesis and quality of life. It is contraindicated in inflammatory breast carcinoma and when negative margins cannot be achieved without causing breast deformity.
A positive margin is an independent risk factor for local recurrence after BCS. Houssami et al. [4] conducted a meta-analysis of 33 studies to determine the association of surgical margins and local recurrence in women with early breast carcinoma and confirmed that positive and close margins (combined) significantly increase risk of local recurrence with odds ratio of 2.44 (p < 0.001) relative to negative margins in patients with invasive carcinoma.
Analysing the margins is important to avoid local recurrence and improve patient–surgeon satisfaction with overall results while re-excision is indicated in case of positive margins. To avoid surprises of positive margins on histopathology and re-operation, several perioperative methods of margin assessment have been proposed. There is still a debate about the ideal technique though.
In our study, the peak prevalence of breast cancer was seen in the fifth decade of life while the mean age was 53.8 ± 11.2 years. However, as a result of increasing awareness, breast carcinomas are being detected at an earlier, more treatable stage. The mean tumor size in our study was 2.7 ± 0.9 cm, which is slightly more compared to the tumour size in other Western studies where mean tumour size ranged 1–2.5 cm [27].
Ultrasound-guided surgery had attained negative margins for all cases with removal of the least amount of healthy breast tissue (CRR 1.2) compared to other groups. Intraoperative ultrasound helps in direct visualization of all margins during excision, which permits adequate margin clearance. Ex vivo ultrasound assesses the completeness of resection avoiding the need for secondary re-excisions, which in turn reduce cost and patient’s anxiety. There was a 6.7% positive margin rate in palpation-guided surgery group. Cavity shaving was found to be helpful in two patients as initial lumpectomy showed positive margins whereas the shaved margins were free of tumour.
One of the initial studies by Moore et al. [17] that evaluated intraoperative ultrasound reported a reduction in the incidence of positive margins from 29% to 3% with the use of intraoperative ultrasound. In 2013, a multicentre randomized controlled trial to compare the effectiveness of ultrasound-guided surgery with standard palpation-guided surgery (COBALT Trial) concluded that ultrasound-guided surgery significantly lowers the proportion of tumour-involved margins (difference 14%, 95% CI 4–25, p = 0.0093), thus reducing the need for re-excision [18]. Another study by Eggeman et al. [28] that analysed positive margins and re-excision rates in patients who underwent BCS with either palpation-guided surgery or intraoperative ultrasound showed ultrasound-guided surgery to be superior (81.1%) to palpation-guided surgery (17.9%) in attaining closest margins. The sensitivity and specificity of intraoperative ultrasound were 52.7 and 97.5% respectively, compared to 15.5% and 65.9% in palpation-guided surgery.
Limitations for the usage of intraoperative ultrasound include the availability of portable ultrasound machines in the operation theatre, its cost, requirement of a radiologist in the operating theatre and increased excision time. With a certain learning curve, surgeons can perform and interpret ultrasound images.
Palpation-guided surgery, which is performed by the tactile skill of the surgeon may sometimes result in the removal of excess breast tissue as it is difficult to define the extent of the disease, especially in dense breasts. There is a marked difference in tissue margins around the tumour with wide margins on some sides and narrow margins on the other side.
Cavity shaving technique is another effective way of attaining negative margins. It was initially introduced as a pathological biopsy technique to examine the incidence of residual tumour bed positivity. Positive margin in our study was 6.7% on initial lumpectomy, which is comparable with other studies. Gomma et al. [19] found that the percentage of positive margin reduced from 40% to 10% with shaving of cavity. A systemic review and meta-analysis by Ke Wang [27] and colleagues comparing lumpectomy alone versus cavity shaving plus lumpectomy reported a significantly lower positive margins with cavity shaving (16.4%) than with palpation-guided surgery (31.9%) while no significant difference between the volume of tissue excised in both the groups was seen. Another study by Chagpar et al. [20] comparing cavity shaving with no cavity shaving reported significantly lower positive margins in the cavity shaving group (19% vs 34%, p = 0.001).
Another important goal of BCS is a satisfactory cosmetic outcome. Important factors influencing cosmetic outcomes include the site of tumour (tumors on the inner half), volume of the resected breast tissue, postoperative wound complications and the amount of radiotherapy.
Of these factors, total lumpectomy volume has a key impact on the cosmetic outcomes following BCS and is considered as the main determinant. The literature shows that cosmetic failure rates are significantly higher when the lump exceeds 50–85 cm3, regardless of the size of the breast and larger excisions significantly influence breast and nipple retractions, lifting of the breast, breast volume and breast contour [16]. A way to quantify excess healthy breast tissue resection is by using the CRR and resection of a large amount of normal breast tissue may require local oncoplasty.
In our study, a significant median TRV (76.9 cm3) and CRR (1.2) were noticed in the ultrasound-guided surgery group, which was a result of least amount of healthy breast tissue resected by ultrasound guidance. COBALT trial [18], comparing palpation-guided surgery and ultrasound-guided surgery, also showed similar results to our study with significantly lower tumor involved margins (95%) and CRR of 1.0 with the use of intraoperative ultrasound as compared to the CRR of 1.7 in palpation-guided surgery.
Haloua et al. studied cosmetic outcome and patient satisfaction with intraoperative ultrasound guidance in BCS on the COBALT trial patients and found that ultrasound-guided surgery patients achieved better cosmetic results, with 20% excellence overall and only 6% rated as poor, whereas only 14% of palpation-guided surgery patients were rated excellent and 13% as poor [24].
A recent study by Gomma et al. [19] found that cavity shaving results in a lower positive margins with a median large resection volume of 120.0 cm3. Similarly, in another study conducted by Pata et al. [29], shaving cavity was associated with a median total resection volume of 131.9 cm3, which was comparable with the median total resection volume of 126.3 cm3 in the cavity shaving technique in our study.
Technically, a more feasible 1.0 cm margin around the lesion was taken into consideration in this study, which is reasonable since no ink on tumour defines a negative margin as per the 2014 SSO and ASRO guidelines. The formula for the prediction of these optimal resection volumes was based on the assumption that tumours are spherical, whereas in truth they may vary in shape. Similarly, the formula for the prediction of total resection volume was based on the assumption that the excision volume is ellipsoid. Actually, specimens might be cylindrical, spherical, cuboid or ovoid. These assumptions were made for simplicity as they allowed a simple calculation from the measurements of the histopathology reports.
Mean excision time was 19.5 min in ultrasound-guided surgery and 13.8 min in palpation-guided surgery, which is similar to the excision time taken in the COBALT Trial [18] (19 min and 15 min respectively). Additional operative time was needed in the ultrasound-guided surgery group to accommodate ultrasound probing during and after the procedure.
A few novel promising methods for an intraoperative assessment of margins include radiofrequency spectroscopy, diffusion-weighted MRI, optical coherence tomography, and near-infrared fluorescence optical imaging [30]. These techniques are not yet widely used in practice as the cost can be a barrier.
The results of this study show that with a few extra minutes, intraoperative use of ultrasound is a reliable tool in reducing resection volumes and attaining negative margins while performing a BCS.
Conclusion
Intraoperative ultrasound-guided surgery showed to be the most effective technique in obtaining negative margins and sparing healthy breast tissue in patients undergoing BCS. In a setup where intraoperative ultrasound is not available, cavity shaving technique can be considered as the second best alternative.
Compliance with ethical standards
Yes
Ethical approval
Obtained
Informed consent
Obtained
Conflict of interest
No
Funding
No funding