
Abstract
Background:
Tumour infiltrating lymphocytes (TILs) exhibit the local immune response directed against tumor growth and metastasis. TILs have emerged as a tool to assess immune-reactivity in various malignancies including colon, ovary, lung, bladder, breast etc as well as independent marker of favourable prognosis in many tumors. TILs in breast cancer (BC) play a role in tumor response to therapy in the adjuvant and neoadjuvant settings, especially in triple-negative cancers.
Material & Methods:
This cross sectional study comprised of 101cases of invasive breast carcinoma. For each case, a representative 5 μm H&E stained section was selected and the clinicopathological details were recorded. To establish the molecular subtype of breast cancer, immunohistochemistry for ER, PR and Her2neu was done. Both stromal (sTIL) and intratumoral (iTIL) TILs were assessed based on the recommendations of the International TIL Working Group (ITILWG).
Results:
A statistically significant difference was observed in the mean sTIL as well as iTIL scores and tumor grade, size, molecular type and lymph node metastasis. A signification correlation was observed between stromal TIL and tumor grade, lymph node metastasis, molecular subtype and mitosis. Intratumoral TIL showed a significant correlation with tumor size, mitosis, tumor grade, distant metastasis, stage and lymph node metastasis. Moreover, stromal and intratumoral TIL showed a highly significant correlation with each other.
Conclusion:
The ITILWG recommendations are reproducible and reliable for the evaluation of sTILs and iTILs. TILs, as evaluated on Hematoxylin and eosin (H&E) slides, has been shown in numerous studies now to be a reliable, reproducible, inexpensive and readily available marker of pre-existing antitumor immunity in breast cancer. We suggest that TILs should be evaluated for each case of breast carcinoma and should be part of histopathology report.
Introduction
Breast cancer is the most common cause of death among females world-wide [1]. Categorizing breast cancer into molecular subtypes has significant prognostic implications. There are five main molecular subtypes of breast cancer that are based on the genes a cancer expresses: (1)
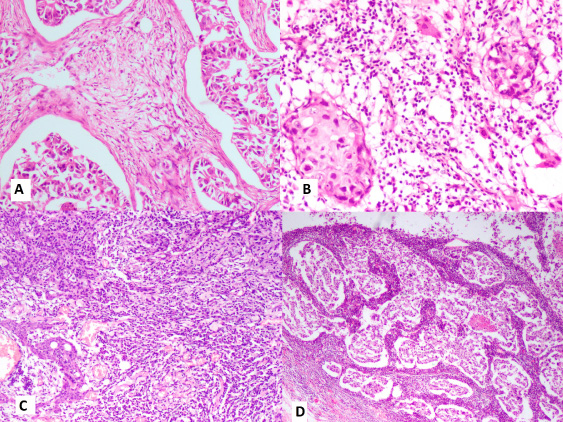
Photomicrograph showing sTIL scoring on H& E slides of breast carcinoma cases – (A) sTIL- 5–7%, (B) sTIL- 30–35%, (C) sTIL-70–80% and (D) sTIL- 95–100%.
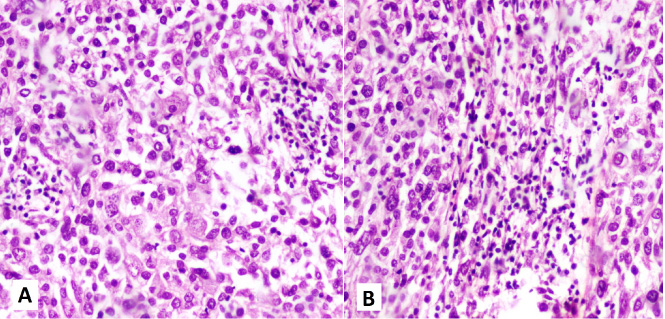
Photomicrograph showing iTIL scoring on H& E slides of breast carcinoma cases – (A) iTIL- score 1 and (B) iTIL- score 2.
The role of immune response in breast cancer is not fully established however, the interest in tumor infiltrating lymphocytes (TIL) as an immunological biomarker for breast cancer has been rapidly gaining momentum on account of various studies demonstrating that TILs predict better response to neoadjuvant chemotherapy especially in triple negative and HER 2 positive tumors. TILs, as evaluated on Hematoxylin and eosin(H&E) slides, has been shown in numerous studies now to be a reliable, reproducible, inexpensive and readily available marker of pre-existing antitumor immunity in breast cancer [3–8]. Salgado et al. [3] proposed that an immunological grade or score should be included in the histopathology reports.
To bring about uniformity, standardization and objectivity in the evaluation of TIL globally, the International TIL Working Group (ITILWG) published recommendations and guidelines in 2014 [3]. There are two types of TILs - stromal and intratumoral. Stromal TILs (sTILs) are dispersed in the stroma and have no direct contact with carcinoma cells while intratumoral TILs (iTILs) are defined as lymphocytes within the tumor nests and in direct contact with tumor cells.
The present study was conducted to evaluate the tumor infiltrating lymphocytes in primary breast carcinomas and determine the correlation between the tumor infiltrating lymphocytes and molecular subtypes, tumor grade, stage and other clinicopathological factors in breast cancer.
The study was carried out at the Department of Pathology, ESIC Medical College, Faridabad over a 3 months period from July 2019 to September 2019. Ethical clearance was obtained from the institutional ethics committee.
The study was a cross sectional study consisting of hematoxylin and eosin(H&E) stained slides comprising of 101 invasive breast carcinoma cases obtained from archives of the department of Pathology, ESIC Medical college and Hospital, Faridabad, Haryana.
Inclusion criteria: Core needle biopsies or Modified radical mastectomy specimens of all invasive breast cancer cases were included in the study
Exclusion criteria: carcinoma in situ cases were excluded
For each case, a representative 5 μm H&E stained section of each case was selected and the clinicopathological details like tumor size, grade, stage etc of the corresponding patients were recorded.
The TIL assessment was performed based on the recommendations of the International TIL Working Group (ITILWG) [3]. The percentage of sTIL was determined at ×200 magnification within the borders of the invasive tumor. The percentage of lymphoid cells to the stromal area was assessed in stromal area between tumor nests as shown in Fig. 1.
For iTIL evaluation, lymphocytes in direct contact with tumor cells were counted. A scoring system proposed by Khoury et al. [4] was followed to allocate an iTIL score to each case. iTu-Ly was scored using a semi-quantitative scoring system (H-score) encompassing the grade of lymphocytic infiltration (0 to 3) as well as the percentage of tumor harboring each grade. The grade of iTu-Ly ranged from 0 to 3, where 0 = virtually no lymphocytes, 1 = sparse intra-tumoral lymphocytes seen only under 40× magnification, 2 = frequent easily recognized lymphocytes seen under 20× magnification, and 3 = tumor is obscured by lymphocytes (Fig. 2). The final score was computed as the sum total of the products of multiplying the grade and the corresponding percentage, resulting a score ranging from 0 to 300 [4]. For example, for a tumor with 50% grade 0, 30% grade 1, 10% grade 2, and 10% grade 3, the final score would be 50 × 0 + 30 ×1 + 10 × 2 + 10 × 3 = 80.
To establish the molecular subtype of breast cancer, immunohistochemistry for ER, PR and Her2neu was done on tumor blocks and the intensity was compared with the controls. Each marker was considered as positive or negative for the purpose of allocating molecular subtype.
All immunohistochemical markers were assessed using light microscopy. A cut-off value of ≥1% positively stained nuclei was used to define estrogen receptor (ER) and progesterone receptor (PR) positivity [9]. HER2 staining was analyzed according to the American Society of Clinical Oncology/ College of American Pathologists guidelines using the following categories: 0 = no immunostaining; 1+ = weak incomplete membranous staining in <10% tumor cells; 2+ = complete membranous staining, either uniform or weak, in ≥10% of tumor cells; and 3+ = uniform intense membranous staining in ≥30% of tumor cells [10]. HER2 immunostaining was considered positive when strong (3+) membranous staining was observed.
Statistical analysis
Data was expressed as number, percentages and mean ± SD as applicable All data was be compiled and analysis was be done using ANOVA and student t tests. Correlation between different variables was calculated by calculating Pearson’s Correlation coefficient. p value of less than 0.05 shall be considered significant.
Observations and results
The present study comprised of 101 breast carcinoma cases including 68 Modified Radical Mastectomies (MRM) and 33 tru cut biopsies/excisional biopsies. Around 60% patients were in 4th & 5th decade followed by 27% cases in the 3rd decade. Infiltrating ductal carcinoma (IDC) was found to be the most common histologic type of breast carcinoma accounting for more than 90% cases followed by medullary carcinoma in around 5% cases.
Based on immunohistochemical staining of hormone receptors (ER, PR) and her 2 neu, breast carcinomas are divided into various molecular subtypes. Luminal A subtype was found to be the most common molecular subtype (in more than 40% cases) while 30% cases had Triple Negative molecular subtype. According to Modified Bloom Richardson grading of breast carcinoma (based on scoring for tubule formation, nuclear pleomorphism and mitotic count), grade 2 was the most frequently observed in more than 60% cases. Out of 68 MRM cases, tumor size of 2–5 cm was observed in around 60% cases.
On classifying the tumors as per TNM stage, more than 60% of the cases belonged to stage 2. Lymph node metastasis was observed in 29 out of 68 cases while lymphovascular invasion was present in 22 cases. Distant metastasis was present in only 8 out of 68 cases. The clinicopathological characteristics of the study population are depicted in Table 1.
Clinicopathological characteristics of the study population
Clinicopathological characteristics of the study population
Mean value of sTIL was calculated in terms of percentage and mean value of iTIL was calculated in terms of score out of 300. Out of 101 cases, sTIL% was found to be more than 50% in 46 cases while iTIL score was under 100 in around 60% cases and hardly 2% cases had score above 200. sTIL and iTIL both showed an increasing trend with increase in tumor grade and the difference was found to be statistically significant for both sTIL (p = 0.00) and iTIL (p = 0.00). In terms of tumor size (n = 68), sTIL and iTIL both did not show an increase between T1 and T2 but there was significant increase between T2 & T3, p value came out to be significant for both sTIL (p = 0.018) and iTIL (p = 0.001).
In the context of molecular subtypes, mean value of both sTIL and iTIL was found to be highest in triple negative subtype and lowest for luminal A subtype (Fig. 3) and the difference was also statistically significant for both sTIL (p = 0.00) and iTIL (p = 0.002).
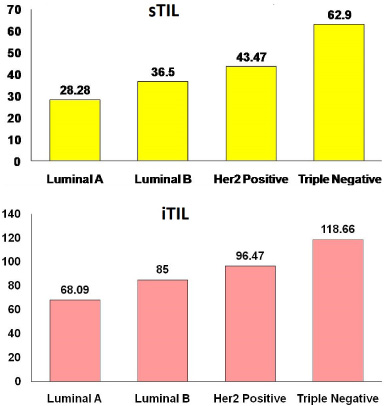
Bar graph showing comparison b/w mean percentage of sTIL’s and iTIL and molecular subtypes of breast cancer.
As mitotic count increased, mean values of both sTIL and iTIL showed an increase. When lymph node metastasis parameter was taken into consideration (n = 68), it was found that mean value of both sTIL and iTIL was more in cases with lymph node metastasis, p value here also came out to be significant for both sTIL (p = 0.0068) and iTIL (p = 0.0015). Mean values of both sTIL and iTIL showed a higher count in the cases with distant metastasis.
As the TNM stage increased from stage 1 to 3, the values of sTIL showed a gradual increase, however not much change was noted from stage 3 to 4. On the contrary, the values of iTIL showed a gradual increase from stage 1 to 4 and it was observed to be statistically significant. The mean values of sTIL and iTIL in the context of various clinicopathological parameters are shown in Table 2.
Mean values of sTIL and iTIL in the context of various clinicopathological parameters
Correlation coefficient was computed to determine the correlation between the tumor infiltrating lymphocytes and various clinico-pathological factors in breast cancer like molecular subtypes, tumor grade, stage etc. A signification correlation was observed between stromal TIL and tumor grade, lymph node metastasis, molecular subtype and mitosis. Intratumoral TIL showed a significant correlation with tumor size, mitosis, tumor grade, distant metastasis, stage and lymph node metastasis. The correlation coefficients of various parameters with each other and with sTIL and iTIL are depicted in Table 3. Moreover, stromal and intratumoral TIL showed a highly significant correlation with each other with a correlation coefficient of 0.818 as depicted in Fig. 4.
Correlation coefficients of various parameters with sTIL and iTIL and with each other
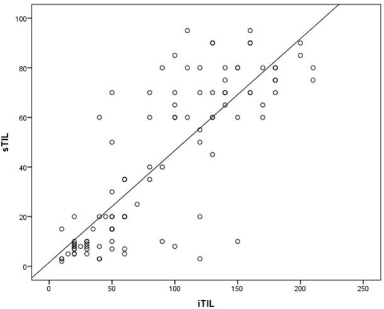
ROC curve showing a highly significant correlation between stromal and intratumoral TIL with a correlation coefficient of 0.818.
Globally, breast cancer is a leading cause of mortality among women while in India, after cervical cancer, it is second most important cancer among females. The pathogenesis of carcinoma breast is multifactorial. There are various conventionally used prognostic indicators for breast cancer comprising of tumour stage, grade, lymph node metastasis, distant metastasis and more recently molecular subtype based on estrogen (ER), progesterone (PR) and human epidermal growth factor receptor (HER2/neu or c-erb B2) status [11].
The tumors are infiltrated by lymphocytes called tumour infiltrating lymphocytes (TILs) exhibiting the local immune response directed against tumor growth and metastasis. Over the last decade, many researchers have emphasized upon the importance of evaluating TILs as a tool to assess immune-reactivity in various malignancies including colon, ovary, lung, bladder, breast etc [11,12] and degree of lymphocytic infiltration has emerged as independent marker of favourable prognosis in many tumors [11–14]. TILs in breast cancer (BC) has intrigued many researchers and is rapidly gaining impulse due to the aggregated studies implying that TILs play a role in tumor response to therapy in the adjuvant and neoadjuvant settings, especially in triple-negative and HER2+ types [15–17]. In some malignancies like triple negative breast cancer, TIL positive and TIL negative have been proposed to reflect tumour types with different response to immunotherapy. Some studies focused on TILs using immunohistochemistry, while others evaluated molecular markers using immunohistochemistry and gene expression analysis.
Most of the literature indicates that stromal TILs are better and more reproducible compared to intratumoral TIL as iTILs are present in less numbers, are detected in fewer cases and are difficult to observe on H&E stained slides. Hence, ITILWG’s latest recommendation is to assess stromal TIL as iTIL do not provide any additional information [3]. Nevertheless, recent evidence indicates that, in the neoadjuvant TNBC setting, and despite the methodological reasoning mentioned above, both stromal as well as intratumoral TILs are predictive of pathological response to neoadjuvant platinum-based chemotherapy. In the current study as well, sTIL and iTIL showed strong correlation with each other with a correlation coefficient of 0.818.
Tumor size and number of positive axillary lymph nodes are the two most important independent prognostic factors in breast carcinoma [18]. We found a statistically significant correlation between both sTIL and iTIL with tumor size as well as lymph node metastasis, similar to findings of Loi et al. [15], Macchetti et al. [19] and Bjelobrk et al. [20].
The current study observed a positive correlation between TIL scoring and Her 2 neu amplification which is in accordance with several other authors [6,20,21]. Moreover, the highest TIL scores were found in triple negative molecular subtype of breast carcinoma and the difference was found to be statistically significant between the various molecular subtypes similar to Loi et al. [6] and Bjelobrk et al. [20]. The literature on TIL in triple negative breast cancers and Her 2 positive tumors as well as our observations imply that triple negative breast cancers and Her 2 positive tumors are more immunogenic compared to luminal A carcinoma, probably the result of increased numbers of lymphocytes in the tumor microenvironment [20]. A statistically significant difference between TIL and tumor grade was observed in the index study similar to Bjelobrk et al. [20].
A positive correlation was observed between TIL scoring and tumor stage which is in accordance with several other authors [20,22]. This could be explained by the fact that lymphocytes’ ability to produce various growth factors like vascular endothelial growth factor, fibroblast growth factor which results in angiogenesis, thereby resulting in spread of malignancy and increase in stage [20,23].
Although extensive literature is available on TIL in breast carcinoma, but still the clinical significance is still poorly defined on account of the variability of techniques employed to assess TIL, that is, histopathology vs immunohistochemistry vs flow cytometry; variabilility of sections full section vs tissue microarray and last but not the least is the inter observer variability.
Our study had several limitations. Firstly, the sample size was relatively small and there was an unequal distribution of patients in each molecular subtype, which could lead to dubious statistical results and alter the characteristic features in the HER2 and/or TNBC types. Second, we did not assess the T cell subpopulations of TILs, however, the recommended method to assess TILs is H&E-stained slides only [3].
Conclusion
To conclude, the ITILWG recommendations are reproducible and reliable for the evaluation of sTILs and iTILs. TILs, as evaluated on Hematoxylin and eosin (H&E) slides, has been shown in numerous studies now to be a reliable, reproducible, inexpensive and readily available marker of pre-existing antitumor immunity in breast cancer. We suggest that TILs should be evaluated for each case of breast carcinoma and should be part of histopathology report. An understanding of the role of tumor infiltrating lymphocytes regarding immune response in tumors is of a critical importance for devising novel immunotherapeutic strategy in breast cancer treatment.
Footnotes
Acknowledgements
The Authors would like to thank Indian Council of Medical Research (ICMR), New Delhi for awarding the Short Term Studentship (STS) to student Harsh Jain.
Authors contributions
Idea & design: Dr Mukta Pujani, Mr Harsh Jain, Dr Charu Agarwal
Data acquisition: Dr Varsha Chauhan, Mr Harsh Jain, Dr Charu Agarwal,
Analysis: Dr Charu Agarwal, Dr Mitasha Singh, Dr Kanika Singh
Interpretation of findings: Dr Mitasha Singh, Dr Mukta Pujani, Dr Kanika Singh
Preparation of manuscript: Dr Mukta Pujani, Mr Harsh Jain
Critical revision: Dr Varsha Chauhan, Dr Kanika Singh
Conflicts of interest
There is no conflicts of interest to declare.