
Abstract
BACKGROUND:
With an aging society, Korean women ≥70 years of age are increasingly being diagnosed with breast cancer.
OBJECTIVE:
To investigate the clinicopathological and biological characteristics of breast cancer in elderly Korean women and compare them with breast cancer in elderly (≥70 years) women globally and in Korean women of all ages.
METHODS:
We retrospectively reviewed the clinicopathological and biological features of breast cancer in elderly Korean women (≥70 years; n = 87) who sought treatment during 2004–2014 from a single institution. These data were indirectly compared with data of Korean women of all ages (nationwide Korean Breast Cancer Registry) or elderly women globally (meta-analysis).
RESULTS:
Compared to elderly women with breast cancer globally, Korean elderly women had a more symptomatic presentation, lower ER expression, and overexpression or amplification of human epidermal growth factor receptor 2. Compared to Korean women of all ages with breast cancer, elderly Korean women presented with advanced tumor stages, larger tumor size, more lymph node involvement, and more luminal B and basal-like subtypes.
CONCLUSIONS:
Breast cancer had a more aggressive clinicopathological and biological characteristics in elderly Korean women than in Korean women of all ages or elderly women globally.
Introduction
Breast cancer is now ranked as the most common type of cancer among women in the vast majority of countries worldwide [1,2]. Although the incidence of breast cancer decreased in the early 2000s in several developed countries, including the United States (US), Canada, the United Kingdom, France, and Australia, its incidence has continuously increased in most developing countries and has increased most rapidly in Asia [1,3–5]. In 2018, of the 2,088,840 new breast cancer cases worldwide, Asian patients accounted for 43.6% (911,014) of the cases [6]. If this steep increase in the incidence rate continues in Asian populations, Asian patients will soon account for the majority of breast cancer cases worldwide [7]. The current knowledge of breast cancer is mostly based on studies performed in Western populations, and there is a relative paucity of data on Asian populations in all aspects of breast cancer research [7].
The same phenomenon is also true for breast cancer in the elderly. Given the aging of the global population, breast cancer in the elderly has increasingly gained attention, and its epidemiology, clinical and biological characteristics, and clinical outcomes have been systematically compared with breast cancer cases in younger patients [8]. However, most global research on breast cancer in the elderly has been conducted in Western populations [8].
Although in Korea the incidence rate of breast cancer was lower in the older than in the younger age group, it is noteworthy that the degree of increase in the incidence was more pronounced in the older than in the younger group [9]. Between 1998 and 2010, the incidence rate of breast cancer among Korean women increased by 2.3, 2.5, 2.6, 3.4, and 3.8 times for women in their 30s, 40s, 50s, 60, and 70s, respectively [9]. Consequently, the median age at diagnosis has gradually increased (from 46 years in 1996 to 50 years in 2015) [9,10]. By 2020, the age of onset of breast cancer is predicted to be similar to that in Western countries [11]. In addition, the Korean population is rapidly aging, and by 2050, individuals aged 70 years or older are expected to comprise 30.4% of the total population, as compared to 9.7% of the total population in 2018 [12].
Nevertheless, knowledge about the biological and clinical behavior of breast cancer in elderly breast cancer patients in Korea is scarce, although it will become crucial to understand the characteristics of breast cancer in elderly Korean women in this era of personalized medicine. Thus, more information about the clinicopathological and biological features of breast cancer is required to provide optimal therapy and management for elderly Korean breast cancer patients.
This study sought to describe the clinicopathological and biological features of primary breast cancer in elderly Korean women. Additionally, as no previous study has described the clinicopathological and biological features of breast cancer in native Korean elderly women aged ≥70 years, we aimed to identify differences in the characteristics of breast cancer in Korean women of different ages, using data from a nationwide Korean breast cancer registry [10,13] and elderly (≥70 years) women globally, using data from a meta-analysis [8].
Materials and methods
Patient selection
The relevant institutional review board approved this retrospective study and the requirement for obtaining informed consent from patients was waived. We searched our institutional database for patients 70 years of age or older with a histopathological diagnosis of primary invasive and in situ breast cancer from January 2004 to May 2014. During this period, the total number of women of all ages with a diagnosis of primary breast cancer was 973. Among these, 87 (8.9%) patients were aged 70 years or older and they were included in this study. This was a cohort study and complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Figure 1 shows the flow diagram for patient inclusion and analysis.
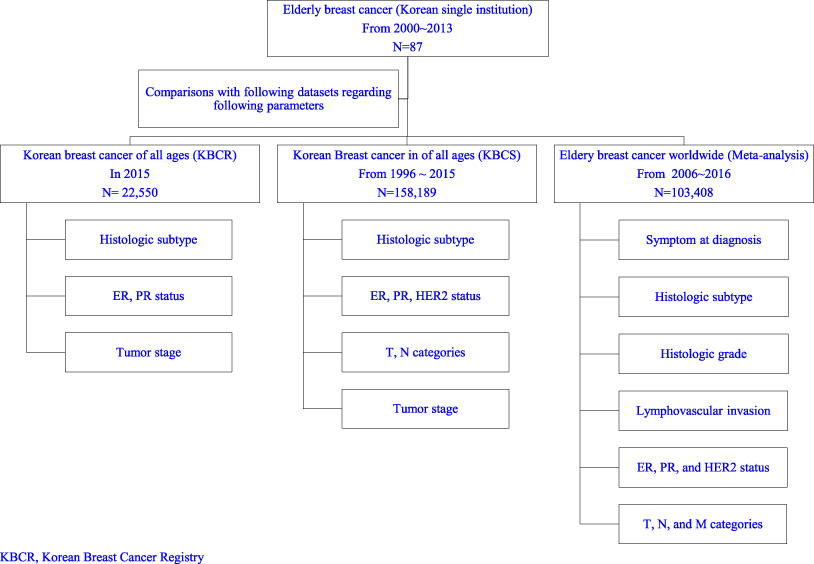
Flow diagram for patient inclusion and analysis.
Clinical data were retrieved through a review of medical charts, and the following information was recorded: age at diagnosis, types of symptoms at presentation, type of surgery, and locoregional recurrence or distant metastasis occurring after surgery.
Pathological and biological data were retrieved through a review of pathology reports, and the following information was recorded: histological subtypes, histological grades for invasive carcinomas, nuclear grades for in situ carcinomas, presence of lymphovascular invasion, and immunohistochemistry (IHC) results of the biological markers such as hormone receptor (estrogen receptor [ER], progesterone receptor [PR]), human epidermal growth factor receptor 2 [HER2], and Ki-67. Histological grades for invasive carcinomas were assigned as grade 1 (low combined histological grade), 2 (intermediate combined histological grade), and 3 (high combined histological grade), according to the Nottingham modification of the Scarff–Bloom–Richardson grading system. For in situ carcinomas, nuclear grades were assigned as grade 1 (low nuclear grade), 2 (intermediate nuclear grade), and 3 (high nuclear grade). ER and PR status were regarded as positive when 1% or more of tumor cells were positively stained in IHC assays [14]. HER2 status was determined primarily by IHC assay, or progressively by in situ hybridization (ISH) if IHC was equivocal [15]. A qualitative scale based on stain intensity was applied to obtain IHC scores: 0 and 1+ were negative, 2+ was equivocal, and 3+ was positive. In cases of equivocal IHC assay results, ISH was used to confirm HER2 status [15]. For Ki-67, a percentage score was determined by IHC assays and a cutoff of 14% was used [16]. Breast cancer biological subtypes were defined based on the IHC results which was a surrogate for molecular testing, followed by implementing the Saint Gallen criteria: luminal A (ER- and/or PR-positive, HER2-negative, and Ki-67 < 14%), luminal B (HER 2-negative; ER- and/or PR-positive, HER2-negative, and Ki-67 ≥14% or HER2-positive; ER- and/or PR-positive, HER2-positive, and any Ki-67), Erb-B2 overexpression (HER2 over-expressed or amplified, ER- and PR-absent), triple-negative (ER- and PR-absent, HER2-negative) [16]. Tumor (T), regional lymph nodes (N), distant metastases (M), and their combinations (anatomic tumor stages) were assigned considering both clinical information and pathological measurement, according to the American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 8th edition [17].
Comparison of breast cancer in elderly women (≥70 years) globally and Korean women of all ages
Clinicopathological and biological data of elderly Korean women in our study were indirectly compared with available data from a recent meta-analysis, which integrated 63 original articles, published between 2006 and 2016, and reflected the status of breast cancer in elderly (≥70 years) women worldwide [8].
Clinicopathological and biological data from elderly Korean women in our study were also indirectly compared with available data from the Korean Breast Cancer Society (nationwide, hospital-based breast cancer registry), reflecting the status of breast cancer in Korean women of all ages in 2015 [10] or between 1996 and 2015 [13].
Statistical analysis
The data are presented as frequency with a percentage for categorical variables. Differences in the study’s participants’ characteristics were compared across the subgroups using the chi-square or Fisher’s exact test for categorical variables. All statistical analyses were carried out using SPSS 24.0 and p values less than 0.05 were considered statistically significant.
Results
Korean elderly breast cancer: Incidence and clinicopathological and biological characteristics (Table 1)
The 87 elderly Korean women (mean age, 74 years; range, 70–88 years) identified in this study constituted 8.9% of women of all ages diagnosed with primary breast cancer at our institution from January 2004 to May 2014. Among the 87 cases, 77 cases were of invasive breast carcinoma and 10 were of in situ breast carcinoma. Details of the clinicopathological and biological characteristics of breast cancer are presented in Table 1.
Pathological, biological, and clinical characteristics of 87 elderly Korean women with breast cancer
Pathological, biological, and clinical characteristics of 87 elderly Korean women with breast cancer
CT, computed tomography; PET, positron emission tomography; BCS, breast conservation surgery; MRM, modified radical mastectomy.
Comparison of breast cancer other than in situ carcinoma between elderly Korean women and elderly women worldwide
Comparison of breast cancer other than in situ carcinoma between elderly Korean women and elderly women worldwide
1 P values were derived from chi-square test. 2 P values were derived from Fisher’s exact test.
In our study, 81.6% of elderly women with breast cancer initially presented with a palpable mass (75.9%) or other significant symptoms (5.7%), such as nipple discharge and skin changes. These values were significantly greater than those (71.8%) observed in a meta-analysis of breast cancer in elderly women globally (p = 0.017, Table 2) [8]. In the meta-analysis, of 7,597 cases of breast cancer in elderly women (age ≥ 70 years), included from 15 articles, symptomatic presentations were noted in 71.8% [8].
Histological subtypes
In our study, among the 77 invasive carcinomas, 88.3% were ductal, 2.6% were lobular, 5.2% were mucinous, and 3.9% were of other histological subtypes. In the meta-analysis of breast cancer in elderly women globally, of the 103,408 elderly cases (patient age ≥ 70 years), included from 28 articles, histological subtypes were ductal in 66.1%, lobular in 8.9%, mucinous in 3.6%, and other in 21.4% of cases [8]. Therefore, compared with the global data [8], the histologic subtypes in Korean elderly women differed significantly (p < 0.001, Table 2): ductal and mucinous subtypes were more prevalent in elderly Korean women than in elderly women globally (88.3% and 5.2% vs. 66.1% and 3.6%, respectively), and the lobular subtype was less prevalent in elderly Korean women than in elderly women globally (2.6% vs. 8.9%, respectively).
Tumor size
In our study, T categories of the 77 invasive carcinomas were as follows: T1 in 44.2%, T2 in 40.3%, T3 in 7.8%, and T4 in 7.8% of cases. In the meta-analysis of breast cancer in elderly women involving 13,981 elderly women (age ≥ 70 years), included from 26 articles, T categories, after excluding tumors of an unknown size (0.6%), were as follows: T1 in 47.5%, T2 in 43.2%, T3 in 5.1%, and T4 in 4.2% of cases [8]. Therefore, compared to the T categories from the meta-analysis [20], larger tumor size (T3 and T4) was more common in elderly Korean women (15.6% in our study vs. 9.3% in the meta-analysis), although the difference was not statistically significant (p = 0.058, Table 2).
Lymph node involvement
In our study, regional lymph node involvement at diagnosis was present in 40.3% of elderly women with breast cancer, which was not significantly different from the frequency (39.2%) reported in the meta-analysis of breast cancer in the elderly [8] (p = 0849, Table 2). In that meta-analysis [8], among the 21,614 cases of breast cancer in elderly women (age ≥ 70 years) recruited from 29 articles, after excluding cases with unknown status for lymph node involvement (7.8%), a metastatic extension to the lymph nodes was present in 39.2% and absent in 60.8% of the cases. However, the high prevalence of an unknown lymph node status (7.8%) in the meta-analysis made it difficult to compare lymph node status between the studies.
Distant metastasis
In our study, distant metastasis was found in 8.0% of patients at the time of diagnosis. This value (8.0%) slightly exceeded that (6.3%) in the meta-analysis of breast cancer in the elderly [8]; however, it did not reach statistical significance (p = 0.214, Table 2). In the meta-analysis, of 87,601 elderly women (age ≥ 70 years) recruited from 22 articles, distant metastasis was present at the time of diagnosis in 6.3% and absent in 93.7% of cases [8].
Histological grade
In our study, of the 77 invasive carcinomas, tumors were a non-high grade (low or intermediate) in 68.8% and high grade in 31.2%. The proportion (31.2%) of high-grade tumors in our study seemed to be slightly higher than that (27.7%) in the recent meta-analysis of breast cancer in the elderly [8]; however, the difference was not statistically significant (p = 0.497, Table 2). In the meta-analysis, of the 20,014 cases of elderly women (age ≥ 70 years) included from 32 articles, histological grade, after excluding tumors of an unknown grade (5.0%), was low or intermediate in 72.3% and high in 27.7% of the cases [8]. The high prevalence of unknown histological grade (5.0%) in the meta-analysis also hampered a comparison between studies.
Lymphovascular invasion
In our study, lymphovascular invasion was present in 30.3% of elderly patients. This finding slightly exceeded the observations (24.4%) of the recent meta-analysis of breast cancer in the elderly [8]; however, the difference was not statistically significant (p < 0.267, Table 2). In the meta-analysis, of the 9,924 global cases of elderly women with breast cancer (age ≥ 70 years), included from 13 articles, lymphovascular invasion was present in 24.4% and absent in 75.6% of the cases [8].
Biological markers
In our study, ER and PR expression and HER2 overexpression or amplification were demonstrated in 66.2%, 49.4%, and 22.1% of the invasive breast cancer in the elderly, respectively. After excluding cases with unknown ER, PR, and HER2 status, the proportions of ER and PR expression and HER overexpression or amplification changed to 67.1%, 50.0%, and 22.4%. In terms of expression of ER, our results (regardless of the inclusion of cases with unknown ER and PR status) were well below the values reported in the recent meta-analysis of breast cancer in the global elderly female population [8] (p = 0.002, Table 2). Based on the meta-analysis, of the 19,627 cases of elderly women with breast cancer (age ≥ 70 years), included from 36 articles, 81.1% were ER-positive [8]. However, in terms of HER2 overexpression (+ ++) or amplification, our results (regardless of the inclusion of cases with unknown HER2 status) significantly exceeded the values of the meta-analysis of breast cancer in the global elderly female population [20] (p = 0.023, Table 2). Of the 8,392 cases, included from 26 articles, HER2 overexpression (+ ++) or amplification was found in 13.4% [8].
Outcomes
In our study, definitive surgery was performed in 74 (85.1%) of patients. Of the 74 patients who underwent surgical treatment, during the follow-up period of a mean of 54 months (range 0–142 months), loco-regional recurrence occurred in 6.8% and distant metastasis occurred in 14.9%. The site of distant metastasis included lung, bone, and axillary lymph nodes. Overall, 75.7% of patients survived without local recurrence or distant metastases.
However, in our study, survival information (overall, loco-regional relapse-free, or metastatic-free survival) was incomplete, because it was unable to conduct a follow-up as the patient had passed away or failed to show up, due to other comorbid conditions or the patients’ individual situations.
In the meta-analysis of breast cancer in the global elderly population, recruited from 25 articles, loco-regional recurrence at 5 years was 9.7%, overall mortality was 34.5% at 5 years and 59.4% at 10 years after diagnosis, and breast cancer-specific mortality was 17.0% at 5 years and 28.9% after diagnosis [8].
Comparison of breast cancer in Korean women of all ages
Tumor stage distribution
In our study, tumor stage distribution was as follows: stage 0 in 11.5%, stage I in 29.9%, stage II in 35.6%, stage III in 14.9%, and stage IV in 8.0%. According to the Korean Breast Cancer Society data, reflecting patients of all ages, the stage distribution of newly diagnosed breast cancer in 2015, after excluding cancers of an unknown stage, was stage 0 in 15.4%, stage I in 44.8%, stage II in 30.4%, stage III in 8.3, and stage IV in 1.1% of cases [10]. Furthermore, the stage distribution of newly diagnosed breast cancer, between 1996 and 2015, when excluding cancers of an unknown stage, was stage 0 in 11.6%, stage I in 38.8%, stage II in 36.8%, stage III in 11.4, and stage IV in 1.3% of cases [13]. Therefore, compared with Korean women of all ages, later stages (II, III, and IV) were significantly more common in the elderly (58.6% in our study group vs. 39.8% in the all-ages group in 2015, p < 0.001, Table 3); later stages (III and IV) were also significantly more common in the elderly (23.0% in our study group vs. 12.7% in the all-ages group between 1996 and 2015, p = 0.004, Table 4).
Comparison of all breast cancer between elderly Korean women and Korean women of all age (2015)
Comparison of all breast cancer between elderly Korean women and Korean women of all age (2015)
1 P values were derived from chi-square test. 2 P values were derived from Fisher’s exact test.
Comparison of all breast cancer between elderly Korean women and Korean women of all ages (1996–2015)
1 P values were derived from chi-square test. 2 P values were derived from Fisher’s exact test.
In our study, T categories of 77 invasive carcinomas were Tis in 11.5%, T1 in 39.1%, T2 in 35.6%, T3 in 6.9%, and T4 in 6.9%. According to the Korean Breast Cancer Society data reflecting patients of all ages between 1996 and 2015, T categories, after excluding tumors of an unknown size (1.3%), were Tis in 12.5%, T1 in 50.2%, T2 in 32.5%, T3 in 3.6%, T4 in 1.1% [13]. Therefore, larger tumor sizes (T2 or higher) were significantly more common in the elderly (49.4% in our study vs. 37.2% in the all-ages group) (p = 0.019, Table 4).
Lymph node involvement
In our study, regional lymph node involvement at diagnosis was present in 35.6% of elderly women. According to the Korean Breast Cancer Society data reflecting patients of all ages, a metastatic extension to the lymph node, after excluding cases with unknown status (1.4%), was present in 33.0% and absent in 67.0% [13]. Therefore, regional lymph node involvement (N2 or higher) significantly more common in the elderly (18.4% in our study group vs. 9.4% in the all-ages group) (p = 0.004, Table 4).
Histological subtypes
In our study, the most frequent histological subtypes was invasive ductal carcinoma (IDC), (78.2%), followed by ductal carcinoma in situ (DCIS) (9.2%), mucinous carcinoma (4.6%), invasive lobular carcinoma (2.3%), papillary carcinoma (2.3%), Paget’s disease (2.3%), and invasive carcinoma of no specific type (1.1%) [8]. According to the Korean Breast Cancer Society data reflecting all ages, the histological types of Korean breast cancer in 2015, after excluding cancers with unknown histology (11.1%), were IDC in 77.5%, DCIS in 14.8%, invasive lobular carcinoma in 4.2%, and other in 3.4% of cases [37]. Furthermore, according to this Society’s data, histological types of Korean breast cancer between 1996 and 2015, after excluding cancers of unknown histology (6.1%), were IDC in 85.0%, DCIS in 11.7%, invasive lobular carcinoma in 3.1%, and other in 0.2% of cases [13].
Therefore, compared with Korean women of all ages [11,13], the distribution of histologic subtypes in our study differed significantly (p < 0.019 in Table 3, p < 0.001 in Table 4): the proportions of IDC, invasive lobular carcinoma, and DCIS were all lower in our study than in the all-ages groups (78.2%, 2.3%, and 10.3% respectively, in our study group vs. 77.5%, 4.2%, and 14.8% respectively, in the all-ages group in 2015; 85.0%, 3.1%, and 11.7%, respectively in the all-ages group between 1996 and 2015); however, the proportion of other subtypes were higher in our study than in the all-ages groups (8.0% in our study group vs. 3.3% in the all-ages group in 2015, 9.2% in our study group vs. 0.2% in the all-ages group between 1996 and 2015)
Biological markers
In our study, ER and PR expression and HER2 overexpression or amplification were demonstrated in 63.2%, 48.3%, and 21.8% of the elderly, respectively. After excluding cases of unknown ER, PR, and HER2 status (6.9% for each status), the proportions of tumors with ER and PR expression and HER overexpression or amplification in the elderly changed to 67.9%, 51.9%, and 23.5%, respectively. According to Korean Breast Cancer Society data reflecting breast cancer patients of all ages in 2015, ER was expressed in 73.7% and PR was expressed in 62.7% of Korean women of all ages with breast cancer [10]. Based on the Society’s data reflecting breast cancer patients of all ages between 1996 and 2015, after excluding cases with unknown ER, PR, and HER2 status (6.5%, 7.8%, and 21.8%, respectively), ER was expressed in 67.9%, PR was expressed in 59.0%, and HER2 was overexpressed or amplified in 25.8% of Korean women of all ages with breast cancer [13]. Therefore, compared with Korean women of all ages [10,13], both ER and PR were less expressed in the elderly (67.9% and 51.9% in our study group vs. 73.7% and 62.7% in 2015 or 67.9% and 59.0% between 1996 and 2015 in the all-ages group), of which statistical significance was met only for PR status (p = 0.045, Table 3). HER2 overexpression or amplification was slightly lower in the elderly group in our study than in the all-ages group of the Korean breast cancer registry (23.5% vs. 25.8%) [13], which did not reach statistical significance (p = 0.775, Table 4).
In our study, molecular phenotypes were as follows: luminal A in 23.5%, luminal B in 44.4%, Erb-B2 overexpression in 12.3%, and basal-like in 19.8% of cases. In the Korean Breast Cancer Society data reflecting breast cancer patients of all age between 1996 and 2015, molecular phenotypes (after excluding tumors of an unknown type) were luminal A in 47.5%, luminal B in 23.5%, Erb-B2 overexpression in 12.2%, and basal-like in 16.9% [13]. Therefore, compared with Korean women of all ages [13], distribution of molecular phenotypes in our study differed significantly (p < 0.001 in Table 4): luminal A was a much less common subtype in the elderly (23.5% vs. 47.5%, Table 4), whereas luminal B and basal-like subtypes were more common subtype in the elderly (44.4% and 19.5% vs. 23.5% and 16.9%, respectively, Table 4). With regard to the luminal B subtype, the prevalence of the luminal B subtype in our study was attributable to a high proliferation index (Ki-67); HER2+ luminal B subtype accounted for 11.1% and HER2–luminal B subtype accounted for 33.3% of cases in our study, whereas the HER 2+ luminal B subtype accounted for 12.7% and the HER2–luminal B subtype for 10.8% in the Korean Breast Cancer Society data [13].
Discussion
This study focused on the pattern of primary breast cancer in elderly (≥70 years) Korean women from a single tertiary referral institution over a 10-year period. In comparison with non-Korean elderly women of the same age with primary breast cancer, Korean elderly women had significantly more symptomatic presentation, more ductal and mucinous histological subtypes, and more HER2 overexpression and amplification, but less frequent ER expression. Moreover, to date, no direct comparison has been made of the tumor characteristics (tumor stage, tumor size, lymph node involvement, distant metastasis, histological subtype, histological grade, molecular phenotypes, and outcomes) between the elderly and younger breast cancer patients in Korea. We show that, in comparison with Korean women of all ages with primary breast cancer, Korean elderly (≥70 years) women had more advanced tumor stages, and more luminal B (high Ki-67) and basal-like subtypes.
Breast cancer incidence and mortality increases with age in developed countries [8]. Women aged ≥70 years represented 30.1% of newly diagnosed breast cancer cases, and 51.2% of breast cancer deaths in developed countries in 2012 [8]. However, the characteristics of breast cancer in Korean women were distinct from those in Western women. Although breast cancer is generally described as a disease of older women, this is not true for Asian women: the incidence of breast cancer in Korea increased with age until peaking at the age of 45–49 years, and thereafter declined with age [10]. According to data from the Korean Central Cancer Registry from 2015, the proportion of patients with breast cancer who were aged 70 years or older constituted only 8.8% of the total breast cancer population across all ages [10]. This pattern is distinctively different from Western countries, where the incidence continuously increased with increasing age [5]. The current Korean guidelines for breast cancer screening essentially involve biennial mammography screening in asymptomatic women aged 40–69 years [18]. Because of the relative rarity of breast cancer in the elderly, to date, the characteristics of elderly Korean patients with breast cancer have not been reported in detail.
The literature to date reports discrepancies regarding tumor stage, tumor size, tumor grade, lymph node involvement at presentation, and outcomes in elderly patients compared with younger patients with breast cancer [8,19,20]. Depending on the different study populations, these parameters are different in the elderly or are not affected by age [8]. Data on the nodal, primary, and metastatic status of these tumors are frequently omitted for elderly patients, and therefore, the percentage of tumors of unknown stage increases with patients’ age [8,21–24]. Insufficient data for elderly patients may partially explain the controversies across studies on whether elderly women present with higher stage tumors, which manifest less aggressively, than young women [24]. In other aspects, the elderly patients could be diagnosed at an advanced stage because the diagnosis may be delayed among the elderly due to a lack of mammographic screening or reduced breast awareness and self-examination [24,25].
In a recent systematic review of 63 international original articles published between 2006 and 2016 of studies of women over 70 years of age with breast cancer, breast cancer in the elderly had distinct clinicopathological features from that in younger patients: breast cancer in the elderly frequently demonstrated favorable biology (low grade, low lymphovascular invasion, hormone sensitivity [? ], histological types with a good prognosis, lack of HER2 overexpression or amplification, lower Ki67, p53, and EGFR expression), but paradoxically, a larger tumor size, more lymph node involvement, and more stage IV metastatic disease [8,19,26–32]. Among the 63 articles included in the meta-analysis, 7 Chinese studies, and 1 Singaporean and 1 Malaysian study reflected the characteristics of the East and South-East Asian populations [8]. Furthermore, among these 9 Asian studies, 3 Chinese studies were reported only in Chinese [8].
It has been reported that breast cancer biological subtypes, defined by ER, PR, and HER2 status, are differently distributed depending on age [32]. ER-positivity sharply inclines with age, while PR-positivity increases more modestly with age, whereas HER2-positivity declines with age [32]. Breast cancer subtypes were also differently distributed across races/ethnicities [33–36]. California-based studies have found that Asian Americans were more likely to be diagnosed with HER2+ breast cancer [33,34,36]. Specifically, Asian American women were more likely to have ER-/PR-/HER2+ or ER+/PR+/HER2+ subtypes, and were less likely to have ER-/PR-/HER2- (triple-negative) or ER+/PR+/HER2- subtypes, than any other subtypes, as compared with white women [33]. Even within the same Asian race, the distributions of breast cancer subtypes varied with ethnicity [higher ER and PR expression]. Among Asian ethnicities in California, Korean women demonstrated widely dissimilar subtype distributions: the lowest percentage was found for the HR+/HER2- subtype and the highest for the HER2+ subtype [35]. Notably, among entire races/ethnicities, including diverse Asian ethnicities in California, Korean women had the highest proportion (36%) of the HER2+ subtype, regardless of ER and PR status [35], and also had the highest percent of ER+/PR+/HER2+ (14.5%), ER-/PR-/HER2+ (11.5%), and ER+/PR-/HER2+ (4.9%) subtypes [34]. Compared with white women, Korean American women were 80% more likely to have HER2+ subtype, regardless of ER and PR status, as compared to HER2- with ER+ and/or PR+ [35].
Breast cancer is indeed a heterogeneous disease, and even the variation of breast cancer subtypes with age manifests differently within each race [32]. Parise et al. studied the variation of eight breast cancer subtypes with age within races, by comparing younger (aged 46–69 years) and older women (aged ≥ 70 years) within the same race [32]. They found that the risk of ER+/PR+/HER2- subtypes were higher in women aged ≥ 70 years than in women aged 46–69 years, for all but white races, in whom the risk of the ER+/PR+/HER2- subtype did not vary with age [32]. Asian/Pacific Islander women showed no variation of the risks of all other subtypes between age ≥ 70 years and age 46–69 years [32]. However, these women showed a significantly reduced risk for the ER-/PR-/HER2+ subtype in the age group under 46 years, but the risk remained the same after age 70 years [32]. For Asian/Pacific Islander women, the risk for the triple-negative subtype did not vary with age [32]. Distribution of breast cancer subtypes has rarely been evaluated for native Korean women [37]. ER, PR, and HER-2 status were evaluated in early-onset breast carcinomas in native Korean women, as compared with age-matched Caucasian women; HER2 overexpression was more frequent in the native Korean women (47.5%) than in the Caucasian women (15.8%) [37].
Breast cancer in the elderly had been preconceived to be relatively indolent and to behave less aggressively, and therefore to spread more slowly than in younger individuals [8]. Accordingly, the relative survival of elderly women with early-stage breast cancer is similar or better than survival in the general population [19], and better than survival in age-matched women without breast cancer [38]. This may be due to the healthy user effect or the additional medical attention, which reduced the number of deaths related to other diseases and improved overall survival, and a higher level of or higher sensitivity to endogenous estrogen, or more hormone replacement therapy, which might have lowered the cardiovascular (coronary artery disease and stroke) risk [19,38]. Barchielli et al. reported that, in an analysis of 1,182 invasive breast cancers, after adjusting for disease extent, age at diagnosis did not significantly impact the 10-year relative survival [39]. They explained that the worse prognosis in the elderly was largely due to death from other causes and that the worse distribution of the extent of disease in the elderly might be associated with delayed diagnosis [39].
This study had several limitations. First, this study inherently had a selection bias resulting from its retrospective design. Second, clinicopathological and biological data of elderly breast cancer patients, both in our study and in previous literature, were missing, which could impede accurate comparison of cohorts across studies Third, the study population was too small and was derived from only a single tertiary referral center, which does not allow generalization to the entire elderly Korean population. A population-based study is further warranted to establish the characteristics of breast cancer in the general Korean elderly population.
To summarize, we showed that breast cancer in the elderly (≥70 years) patients in Korea seemed to have aggressive clinical, pathological, biological characteristics. Breast cancer presentations in the elderly might reflect the intertwined impact of age, race, ethnicity, and individual biological and genetic backgrounds. Therefore, it is difficult to apply uniform standards of management to breast cancer in the elderly, for each race/ethnicity. This study may provide some insights into breast cancer in the elderly in Korea and facilitate the development of optimized management of these patients. In the future, a population-based study should be performed to improve the management of breast cancer in older Korean women.
Footnotes
Acknowledgements
This work was supported by a grant from the Research year of Inje University in 2017 (20170045).
This work was supported by “Inje University Haeundae Paik Hospital”.