
Abstract
Background
Impairment of the activities of daily living (ADL) due to dementia can reduce the quality of life of patients and increase the burden on caregivers, necessitating appropriate interventions. Recently, the effectiveness of telerehabilitation for patients with dementia has been demonstrated, but its effect on ADL is uncertain.
Objective
We report on a 76-year-old female patient with Alzheimer's disease who underwent photo assessment for activities of daily living (PA-ADL) in the home environment and online management (O-MGT) at home.
Methods
The PA-ADL and O-MGT were implemented because of the progressive impairment of instrumental ADL and increased caregiver burden. In the PA-ADL, occupational therapists used photos of her home environment taken by her caregivers to check off environments that might pose a risk for life disability and set rehabilitation goals. Using a videoconferencing system, O-MGT had a therapist provide goal-directed ADL interventions remotely while she and her caregivers were at home.
Results
She improved in behavioral psychological symptoms and instrumental ADL after our PA-ADL and O-MGT intervention package, despite no improvement in cognitive function. In addition, caregiver burden was also found to be reduced after these interventions.
Conclusions
The PA-ADL and O-MGT intervention packages improved some of her behavioral and psychological symptoms, ADL abilities, and caregiver burden. Physical environment assessment using home photos and remote ADL rehabilitation may be considered options for Alzheimer's disease patients with ADL impairment.
Introduction
Dementia influences activities of daily living (ADL), interaction, and participation, and impairs the ability to engage in certain behaviors. 1 Dementia rehabilitation focuses on activities and participation, 2 and ADL interventions and role building are important. For patients with dementia to continue living at home, it is important for rehabilitation professionals, such as occupational therapists, to assess ADL and target specific interventions for impaired ADL in each patient's home environment. One of the challenges associated with the spread of COVID-19 was the increased risk of viral transmission owing to contact between patients and medical staff. However, remote dementia rehabilitation has been reported to be as effective as traditional face-to-face interventions. 3 This suggests that face-to-face care is not always necessary in dementia rehabilitation and that it is important to consider telemedicine to help people with dementia live sustainably in familiar communities. We modified the previously reported Photographic Assessment of Living Environment 4 for ADL and investigated the usefulness of a photo assessment for ADL (PA-ADL). Furthermore, we investigated the usefulness of the online management (O-MGT) of ADL in older women with moderate-severity dementia due to Alzheimer's disease (AD). These tools are designed for community-dwelling patients with mild to moderate AD. Our aim was to determine whether a series of intervention packages, PA-ADL and O-MGT, are effective in improving ADL in community-dwelling patients with AD. This report was prepared in accordance with the CARE guideline. 5
Methods
Case presentation
A 76-year-old married Japanese woman lived with her husband, spent her time walking a dog, and helped her husband during the day. Meals were prepared by the delivery service and her husband, and her main responsibility was laundry. Several years before diagnosis, her family said that she was forgetful, but she compensated by claiming that her forgetfulness was appropriate for her age. Four months before the first visit, she had lost track of where she had left her car on the way home from a drive and had to ask a passing car for a ride. Immediately prior to her hospitalization, her ability to perform ADL was severely impaired, as she had lost the ability to use her cell phone and had been observed to have sudden bouts of crying and other signs of emotional instability. Concerned family members admitted the patient to the hospital for a two-week stay to thoroughly evaluate her cognitive impairment. She exhibited a slow, progressive impairment of recent memory and a severe impairment of visuospatial cognitive function. She stopped participating in golf with friends and no longer attended the women's association for which she had been president, indicating a decline in her social functioning. Single-photon emission computed tomography (SPECT) revealed hypoperfusion in the parietal, temporal, and occipital regions of the brain. Brain magnetic resonance imaging (MRI) demonstrated severe atrophy in the parietal and hippocampal regions. Minor white matter lesions were also observed but were not considered significant for diagnosis (Figure 1). The amyloid-β 1-42/1-40 ratio in the cerebrospinal fluid (CSF) was 0.057, which was significantly lower than the reference value of 0.067. The concentration of total tau in the CSF was 579 pg/mL, whereas that of phosphorylated tau was 79.0 pg/mL, respectively, exceeding the respective reference values of 400 pg/mL and 59 pg/mL. The observed beta-amyloid ratio and elevated phosphorylated tau levels suggest the presence of AD, whereas increased total tau levels indicate neuronal damage. Based on clinical findings, imaging findings, and CSF biomarker results, she was diagnosed with late-onset AD. Significant parietal atrophy was present, raising concerns about the progression of visuospatial cognitive impairment in the future. Frontotemporal dementia, dementia with Lewy bodies, and vascular dementia were also considered in the differential diagnosis; however, these were ruled out because of the absence of typical clinical symptoms and imaging findings, including normal dopamine transporter SPECT and metaiodobenzylguanidine myocardial scintigraphy results (data not shown). During the diagnostic process, we examined economic, cultural, and linguistic factors, but did not find any that directly influenced the diagnosis in this case. However, some of these factors contributed to the delayed diagnosis of AD as follows: The loss of caregiver productivity due to her care was identified as an economic factor that challenged the diagnosis. In addition, the patient lived in an area with limited access to medical care and lived with her husband. She needed to maintain a domestic role for as long as possible, and this cultural factor may have delayed professional evaluation and diagnosis of AD. Linguistic factors related to the diagnosis, such as the tendency to mend her forgetfulness and the dialect in her area of residence, may also have contributed to the delay in recognizing that she had the clinical symptoms characteristic of AD. Baseline neuropsychological and ADL assessments were as follows: Mini-Mental State Examination (MMSE), 15/30; Clinical Dementia Rating (CDR), 2; Neuropsychiatric Inventory (NPI), severity 32/120 and caregiver distress 15/50; Geriatric Depression Scale (GDS), 4/15; Physical Self-Maintenance Scale (PSMS), 3/6; and Lawton IADL, 3/8. The patient scored 123/210 points on the Process Analysis of Daily Activities for Dementia (PADA-D),6 consisting of 86/90 points for basic ADL and 37/120 points for instrumental ADL. The short version of the Zarit Care Burden Scale (J-ZBI8) score was 8/32. As a drug therapy, Yokukansan 7.5 g/day was prescribed from the second day of hospitalization, and the same drug therapy was continued after discharge. She was not taking any medications prior to admission. Yokukansan is a traditional Japanese Kampo medicine approved by the Ministry of Health, Labour and Welfare for the treatment of night crying and irritability in children, neurosis, insomnia, and behavioral and psychological symptoms of dementia (BPSD). 7 The Japanese Society of Neurology also recommends the use of Yokukansan for BPSD. 8
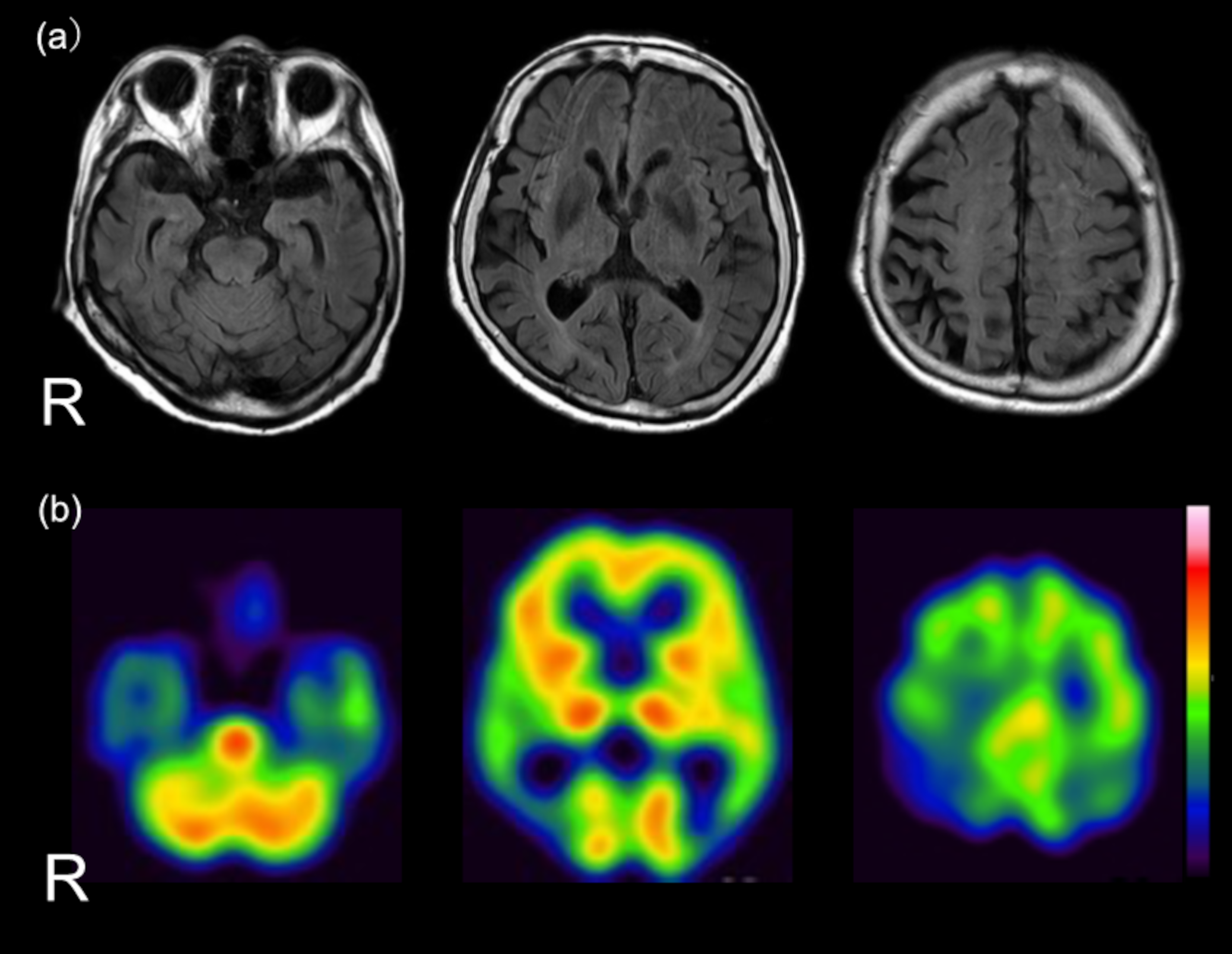
Brain MRI results of the patient.
We have obtained written informed consent from the patient's family and the patient's own informed assent to participate in this study and publish this case report.
Intervention procedure
On the day of discharge, written informed consent was obtained from her family, and informed assent was obtained from her. Her family was given the device and instructions for performing PA-ADL (Figure 2(a)) and asked to take photographs of their home environment in the presence of the patient and family members. The key points of photography were to consider the patient's usual point of view and avoid moving or cleaning objects for photography purposes. The patient's outpatient visit took approximately 90 min from her home, with her fourth son serving as the primary caregiver. On the next outpatient day, a 60-min interview about the patient's living situation was conducted based on photographs taken at home. During the interview, the patient and family were asked questions about the usual living situation, ADL she could perform, and those she needed help with, all in the presence of the patient and family. Based on the information obtained from the interviews, we completed a PA-ADL checklist (Figure 2(b)) and shared with the patient and family three life issues that we considered to be the most important needs for caregivers and patients: 1) the home is cluttered with many objects, 2) clothes are scattered and of different seasonal types, and 3) it is unclear whether medications are being administered correctly. The O-MGT was then administered in parallel with the usual 1/three-weeks outpatient clinic. A tablet PC (iPad) and a data communication device were lent to family members, and the O-MGT was administered approximately once every two weeks for 60 min per session using a video conferencing system.
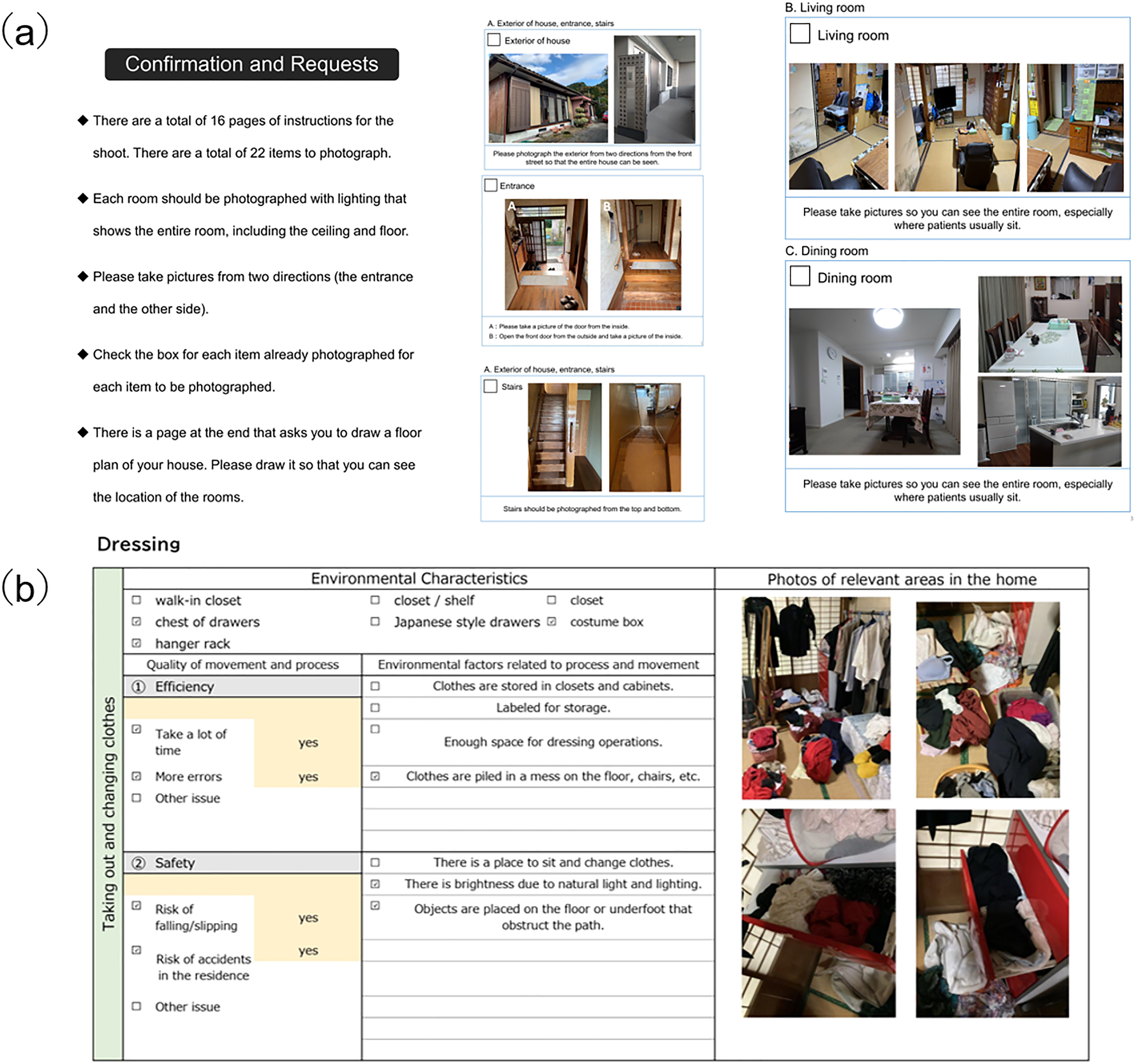
Photography instructions and checklist of PA-ADL.
Results
The contents of the five O-MGT sessions and the personnel and time costs for each session are presented in Table 1. Figure 3 shows the changes in the home environment regarding medication and dressing/laundry, which were the focus of the O-MGT intervention. No unexpected or adverse events occurred during the intervention period. Family members of patients who received O-MGT said, “I can put the instructions into practice immediately without forgetting,” and “I don't have to go all the way to the hospital, so it's less inconvenient.” After 3 months of intervention, the patient was re-assessed as follows: MMSE, 15/30; CDR, 2; NPI, severity 6/120 and caregiver distress 8/50; GDS, 3/15; PSMS, 4/6; Lawton IADL, 3/8; PADA-D, basic ADL 65/90 and instrumental ADL 40/120, for a total of 105/210; and J-ZBI8, 7/32.
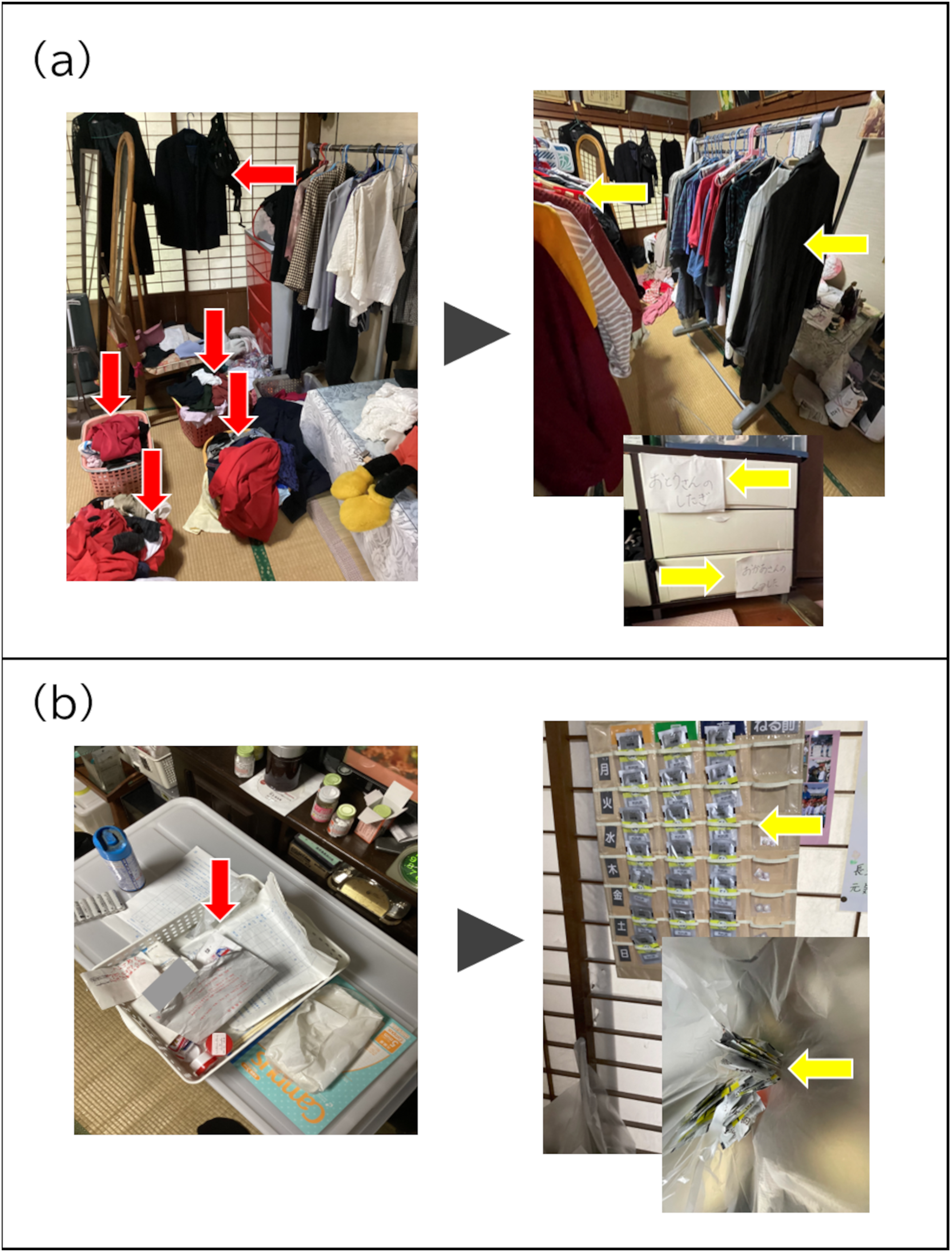
Examples of environmental changes in the home before and after O-MGT.
Description of the o-MGT implementation.
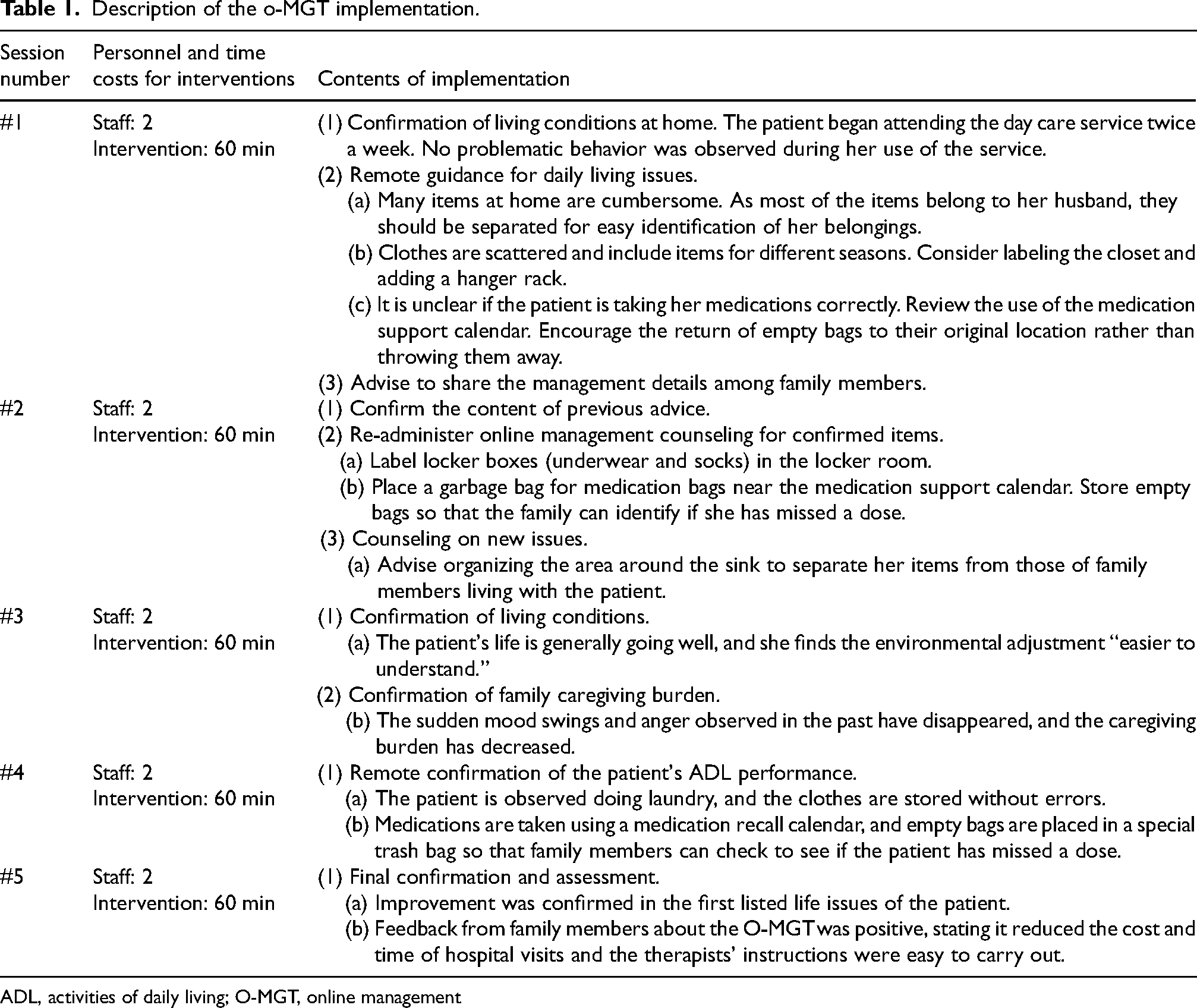
ADL, activities of daily living; O-MGT, online management
Discussion
In the field of psychiatry, much medical care can be provided through face-to-face interactions between patients and physicians, and this is considered one of the most widely used fields of telemedicine in the world. 9 Although a relatively large body of evidence 10 showing that telemedicine in psychiatry does not differ from face-to-face care in terms of diagnostic accuracy or treatment effectiveness, there are few reports on its effectiveness in dementia rehabilitation for ADL impairment. 11
In this case study, PA-ADL was used to assess the factors of ADL impairment and BPSD in the physical environment of the patient's home using photographs. Based on the PA-ADL, guidance such as environmental improvement and ADL guidance was provided remotely via the O-MGT. Therefore, it is recommended to use PA-ADL and O-MGT together as a package. The only intervention during her hospitalization was medication, which was intended to diagnose the patient through close assessment of cognitive function and biomarkers. Therefore, the patient's ADL was not approached during the hospitalization. However, it is undeniable that the hospitalization may have altered her ADL ability.
It is important to note that not all rehabilitation protocols implemented in this study were conducted remotely. Instead, they included face-to-face home situation interviews conducted by occupational therapists (SS and TT). This interview was important to establish trust between the patient, family, and therapist, and to build a foundation for the continuation of the telehealth relationship. It should be reiterated that, particularly in an aging society such as Japan, it is increasingly more common for older adults to care for other older adults, and some patients and families may be resistant to new technologies, such as teleintervention.
A series of interventions using PA-ADL and O-MGT were designed to primarily target mild to moderate community-dwelling AD patients. With the accumulation of future data, we believe that indications for patients with AD of different severity and for other types of dementia (dementia with Lewy bodies, frontotemporal dementia, etc.) should also be considered. For example, in dementia with Lewy bodies, hiding the pattern of carpets and curtains in the home has been shown to reduce visual hallucinations, 4 and this can be achieved by remote intervention. There are alternatives to remote intervention, such as leaving the family to organize without support or sending people with AD to a residential facility, but family members may not have enough knowledge about how to improve the environment to make it easier for the person with dementia to live there, while moving the person to a residential facility may increase the cost of care. Of further concern is the development of symptoms such as anxiety, confusion, hopelessness and loneliness, known as relocation stress syndrome, which occurs immediately after an older adult moves from a private home to a nursing home or assisted-living facility. 12 In addition, efforts to make it easier for people with dementia to live at home are becoming increasingly important, as Japan has introduced a plan to encourage people with dementia to continue living in the community from 2013. 13 We believe that remote intervention is an innovative and cost-effective way to improve ADL and BPSD in community-dwelling AD patients. One factor that increases the effectiveness of this remote intervention is the cooperation of the family. Family members may change their attitudes toward the person with AD as they understand his or her unique lifestyle and psychological state through a series of remote intervention sessions. We believe that this kind of mutual involvement can increase the effectiveness of the remote intervention. As home visit education for family members of AD patients has been shown to be effective for both patients and family members, 14 it is expected that the remote intervention will similarly improve family members’ understanding of AD and their ability to support ADL of AD patients. In addition, differences in the patient's home environment may be a confounding factor in the success of O-MGT. Therefore, it is preferable that the health care professionals performing the O-MGT be occupational therapists or other staff with experience in helping patients with different home environments in a variety of settings. In the future, we would like to develop our practice into a manual and intervention package that would be accessible to more health professionals.
The advantages of O-MGT are that patients and caregivers can receive instructions from rehabilitation professionals in the comfort of their own homes and that rehabilitation professionals can check the actual movement performance status of the patient at home. In the present case, medication was started after hospitalization and continued after discharge, so the possibility that this improvement was due to medication cannot be ruled out. However, despite the fact that the patient started medication in the hospital, ADL and BPSD improved at the final assessment after O-MGT compared with the initial assessment immediately after discharge, suggesting that the combination of pharmacotherapy and O-MGT may also be effective. An additional advantage is the cost. The O-MGT sessions can reduce the cost of mobility, fuel, and travel time for the caregiver and the individual to come to the hospital, or for the medical staff to visit the patient's home, compared to traditional outpatient or home rehabilitation. These costs would be significant compared to the cost of purchasing a mobile device for remote intervention. Upon completion of the PA-ADL and O-MGT interventions, we received positive feedback from her families regarding the effectiveness of the interventions and the reduction in hospital visit costs. Therefore, the PA-ADL and O-MGT protocols developed in this study may be useful not only for infection control but also for remote islands and remote medical care.
The PA-ADL and O-MGT were useful in improving ADL impairment, BPSD, and caregiver burden. This is because, unlike ADL practice in hospitals and institutions, ADL practice and environmental adjustment can be performed at home. Environmental changes in people with dementia have been identified as factors that lead to increased stress. 15 In other words, the ability to receive ADL instruction from family members in a safe home environment may have been effective in reducing BPSD. It is also suggested that caregivers may have experienced an immediate improvement in the patients’ condition as a result of the environmental adjustment provided by the O-MGT and the advice provided by professionals, thereby reducing the burden of caregiving. However, it cannot be denied that the use of day care and medication adjustments may have contributed to the formation of a rest-activity rhythm and played a role in her improvement. In addition, the current case was a patient with moderate AD, but it is necessary to verify whether this intervention is also effective even in patients with mild or severe AD. As this is a case report, future studies with a comparison group or a larger cohort is crucial to minimize the effects of random errors and to generalize the findings. This would help in developing robust conclusions that can be effectively integrated into clinical practice.
Conclusions
Interventions using PA-ADL and O-MGT as packages for community-dwelling older adults with dementia have the potential to improve ADL impairment, BPSD, and caregiver burden. O-MGT for people with dementia is expected to reduce not only the risk of infection but also the cost of hospital visits and caregiver burden. This study is limited to a single case. In future, it will be necessary to accumulate a larger number of cases and investigate the effectiveness of PA-ADL and O-MGT in people with dementia using high-level evidence methods.
Footnotes
Acknowledgments
We would like to thank the patient and her family for their contribution and willingness to participate in this case report.
ORCID iDs
Author contributions
Suguru Shimokihara (Conceptualization; Data curation; Writing – original draft; Writing – review & editing); Takayuki Tabira (Conceptualization; Data curation; Project administration; Writing – review & editing); Ryuji Fukuhara (Data curation; Investigation; Writing – review & editing); Takanori Ishizuka (Data curation; Investigation; Writing – review & editing); Hitoshi Sakimoto (Data curation; Investigation; Writing – review & editing); Kazuki Matsumoto (Data curation; Investigation; Writing – review & editing); Tetsuya Kondo (Data curation; Investigation); Kaoru Arai (Data curation; Investigation); Kunihiko Katsuki (Investigation; Writing – review & editing); Daiki Ishimaru (Data curation; Investigation; Writing – review & editing); Yuma Nagata (Data curation; Investigation; Writing – review & editing); Maki Hotta (Conceptualization; Data curation; Investigation; Writing – review & editing); Manabu Ikeda (Conceptualization; Project administration; Writing – review & editing); Masayuki Nakamura (Conceptualization; Investigation; Project administration; Writing – review & editing).
Funding
This work was supported by Health, Labour and Welfare Sciences Research Grants (grant number: 22GB1001) and Grants-in-Aid for Scientific Research (KAKENHI, grant number: 24KJ1846).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.