
Abstract
Several data suggest that physical activity and cognitive stimulation have a positive effect on the quality of life (QoL) of people with Alzheimer’s disease (AD), slowing the decline due to the disease. A pilot project was undertaken to assess the effect of cognitive stimulation, physical activity, and socialization on patients with AD and their informal caregiver’s QoL and mood. Fourteen patients with AD were randomly divided into active treatment group and control group. At the end of treatment, a significant improvement in apathy, anxiety, depression, and QoL in the active treatment group was found. Considering caregivers, those of the active treatment group exhibited a significant improvement in their mood and in their perception of patients’ QoL. This study provides evidence that a combined approach based on cognitive stimulation, physical activity, and socialization is a feasible tool to improve mood and QoL in patients with AD and their caregivers.
Introduction
Alzheimer’s disease (AD) is the most common form of dementia. 1 It is a slowly progressive neurodegenerative disease characterized by the presence of multiple cognitive deficits in the absence of delirium, which cause a significant impairment in common activities of daily living (ADL) and are of such a magnitude to represent a decline from the previous level of functioning in the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision [DSM-IV-TR]). 2 Noncognitive symptoms, concerning the sphere of personality, affectivity, and behavior, are also of central importance in the clinical profile of the disease.
Previous studies suggest that the course of AD could be positively influenced by 2 different variables: physical activity 3 and mental activity. 4 Regarding physical activity, defined as any bodily movement produced by skeletal muscles that requires energy expenditure, some studies 5 –9 reported benefits due to such activity on learning and memory in patients with AD. Furthermore, as discussed by Dvorak and Poehlman, 10 physical activity interventions in patients with AD may represent a practical and inexpensive strategy to slow down the progressive loss of muscle mass which is often present in patients with AD and which is associated with a reduction in the level of autonomy and independence. Thus, the maintenance of good physical conditions in patients with AD (ie, health conditions that, aside from the cognitive impairment, is not significantly different from healthy individuals of the same age) may not only improve their lifestyle, but also prolong their independence and could slow the disease progression. It is well known that physical activity is characterized by 2 main aspects: intensity and duration. Therefore, in choosing the type of activity to be used, these 2 variables had to be taken into account. The existing literature supports the view that aerobic exercise at low intensity, such as walking, could be relevant. In fact, Weuve et al 11 found a significant reduction in cognitive decline in older women who practiced a long-term regular physical activity, including walking, compared to the ones who had lower levels of energy expenditure. Recently, Erickson et al, 12 in a randomized-controlled trial with 120 older people, observed that aerobic exercise training increases the size of the anterior hippocampus, leading to improvements in spatial memory. Arkin 13 studied the effect of regular aerobic and weight training workouts on noninstitutionalized patients affected by dementia and found not only fitness and mood improvements but also socialization benefits in all the participants. Teri et al, 14 carried out a randomized-controlled trial comparing a group of patients randomly assigned to routine medical care and another group assigned to a home-based physical activity program combined with caregiver training in behavioral management techniques. After 3 months, the program significantly improved the physical health and depression in patients with AD, reducing functional dependence and allowing less institutionalization of patients due to behavioral disturbances. A meta-analysis 15 to evaluate whether physical activity could be beneficial for people with dementia and related cognitive impairments concluded that exercise training increases fitness, physical function, cognitive function, and positive behavior in people with dementia and related cognitive impairments.
Concerning cognitive stimulation, Olazarán et al 16 evaluated the efficacy of a cognitive-motor program in patients with early AD; they observed that patients receiving psychosocial support plus cognitive-motor intervention maintained cognitive status at month 6, whereas patients receiving psychosocial support alone had significantly declined at that time. Moreover, Quayhagen et al 17 analyzed the effects of cognitive stimulation not only in patients with dementia but also in their caregivers and observed that patients who underwent cognitive stimulation had more improvement over time in cognitive outcomes, and their caregivers decreased in depressive symptoms. Very recent publications confirm these observations. 18,19
Finally, it has been recently observed that socialization, together with language-enriched exercises, is capable of slowing cognitive decline in patients with AD. 20
From these observations, we carried out a pilot study called GAIA (Gruppo Alzheimer In Attività, ie, Alzheimer Group In Activity) to assess the effect of simultaneous application of cognitive stimulation, physical activity, and socialization on cognitive and behavioral symptoms as well as quality of life (QoL) of patients with AD. Moreover, we investigated the effect of such activities on caregiver’s burden of care including mood and their perception of patients’ QoL.
Materials and Methods
Study Population
Patients with AD were enrolled from the Alzheimer and Dementia Centre of Neurologic Clinic of the University of Catania. Only patients with AD who were resident in the province of Catania were enrolled. The study was approved by the local ethical committee, and patients were enrolled only after signing the informed consent by themselves and by the respective caregiver.
Diagnosis of AD was made according to the diagnostic criteria proposed by National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA) 21 for probable or possible AD. Inclusion criteria were a Mini-Mental State Examination (MMSE) 22 score of 16 to 24 (mild-to-moderate AD); adequate visual and auditory abilities to perform all aspects of the cognitive and functional assessments; enough mobility to allow their transportation and their participation in all exercises planned for the program; the presence of reliable caregivers willing to participate; a stable dose regimen of memantine and/or cholinesterase inhibitors and/or antidepressants for at least 6 months prior to the beginning of the study. Exclusion criteria were significant neurological diseases, other than AD, that may affect cognition; current presence of a clinically important major psychiatric disorder; current use of medication for cognitive enhancement (eg, ginkgo biloba) other than cholinesterase inhibitors or memantine as previously described; current clinically important systemic illness that is likely to result in deterioration of the participant’s condition or affect the participant’s safety during the study.
Fourteen consecutively admitted patients (aged 72.6 ± 9.5 years; mean ± SD) were enrolled in the study and were randomly assigned to the active treatment group or to the usual care as control group according to a list of randomly generated sequence of numbers.
Both patients and their informal caregivers underwent a battery of tests before the experimental phase and at the end of the experiment. In order to assess patients’ cognitive–behavioral symptoms and QoL, the following tests were administered to all the patients: MMSE; Frontal Assessment Battery 23 assessing executive functions; ADL 24 ; Instrumental Activities of Daily Living 25 ; Clinical Dementia Rating scale 26 assessing severity of dementia; Cornell Scale for Depression in Dementia 27 ; Cornell-Brown Scale for Quality of life in Dementia 28 ; Apathy Evaluation Scale 29 ; Quality of Life–Alzheimer’s Disease (QoL-AD; version for the patient and total value) 30 ; and Hamilton anxiety rating scale. 31 We also evaluated caregivers’ depression and burden, as well as their perception of the QoL of the patient by using the following tools: Caregiver Burden Inventory 32 ; Beck Depression Inventory 33 ; and QoL-AD (version for the caregiver). 30 Examiners were blinded to patients’ treatment.
Protocol
The enrolled patients were divided in 2 groups: the treatment group and the control group. During the study period, the patients of the control group carried out their usual activities at home. The treatment group underwent a program lasting 3 months and consisting of cognitive stimulation, physical activity, and socialization. In particular, every morning, 5 days a week from Monday to Friday, patients were driven from their homes to a gymnasium, where they stayed from 9:30
Regarding the distribution of activity of a single morning, the 4 hours were distributed in this way: 30 minutes for transportation to gymnasium, 1 hour for physical activities (3 blocks of 15 minutes with a 5-minute break between blocks), 15 minutes of interval, 1 hour for cognitive stimulation (3 blocks of 15 minutes with a 5-minute break between blocks), 15 minutes of interval, 30 minutes for group discussion, and 30 minutes for transportation to home. Each patient was assisted by 2 trained psychology and physical education (PE) students, constantly supervised by a trained neurologist, expert in neuropsychology and rehabilitation (T.M.), who was physically present during all the sessions all the time. Students were trained for about 3 months at the neurological clinic and received general information about AD.
Concerning the transportation, all patients were taken from their homes, picked up in a minivan that brought them to the gymnasium; and at the end of the morning, the patients returned to their home. The distance was about 15 km. On the way, music was played (old Italian songs that all patients knew), and one of us (T.M.) stimulated patients to interact with each other, singing all together or talking about everyday life. We decided to drive patients directly from their homes in order to support the caregivers who were already overburdened. For the same reason, we did not require caregivers to supervise or administer any activities.
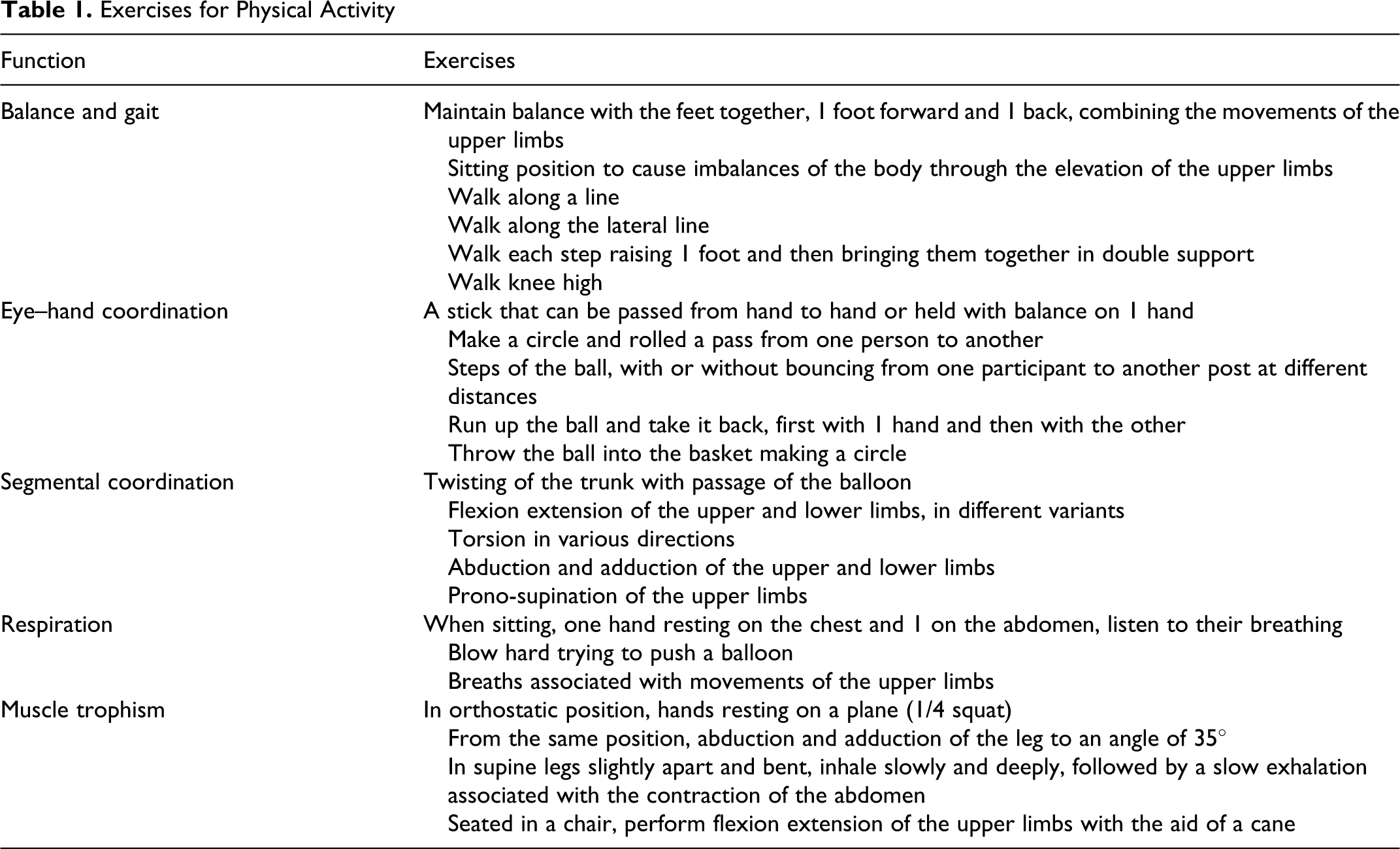
Concerning physical activity, all the patients of the treatment group performed a program of regular physical activity 1 hour a day and the participants performed an aerobic exercise of mild intensity (about 55% maximal oxygen uptake [VO2max ]). This was estimated for each patient at the beginning of the program by measuring the patient’s heart frequency, with a digital heart rate monitor and by using the Karvonen formula. 34 The performed activity was equal to an energy consumption of 3 to 5 metabolic equivalent (MET) of task per hour (1 MET = 3.5 mL O2 /kg per min = 0.0175 kcal/kg per min = 0.0732 kJ/kg per min). The physical activity consisted of exercises for balance and gait, eye–hand coordination, segmental coordination, respiration, and muscle trophism. All the exercises were performed every day (Table 1).
Exercises for Physical Activity
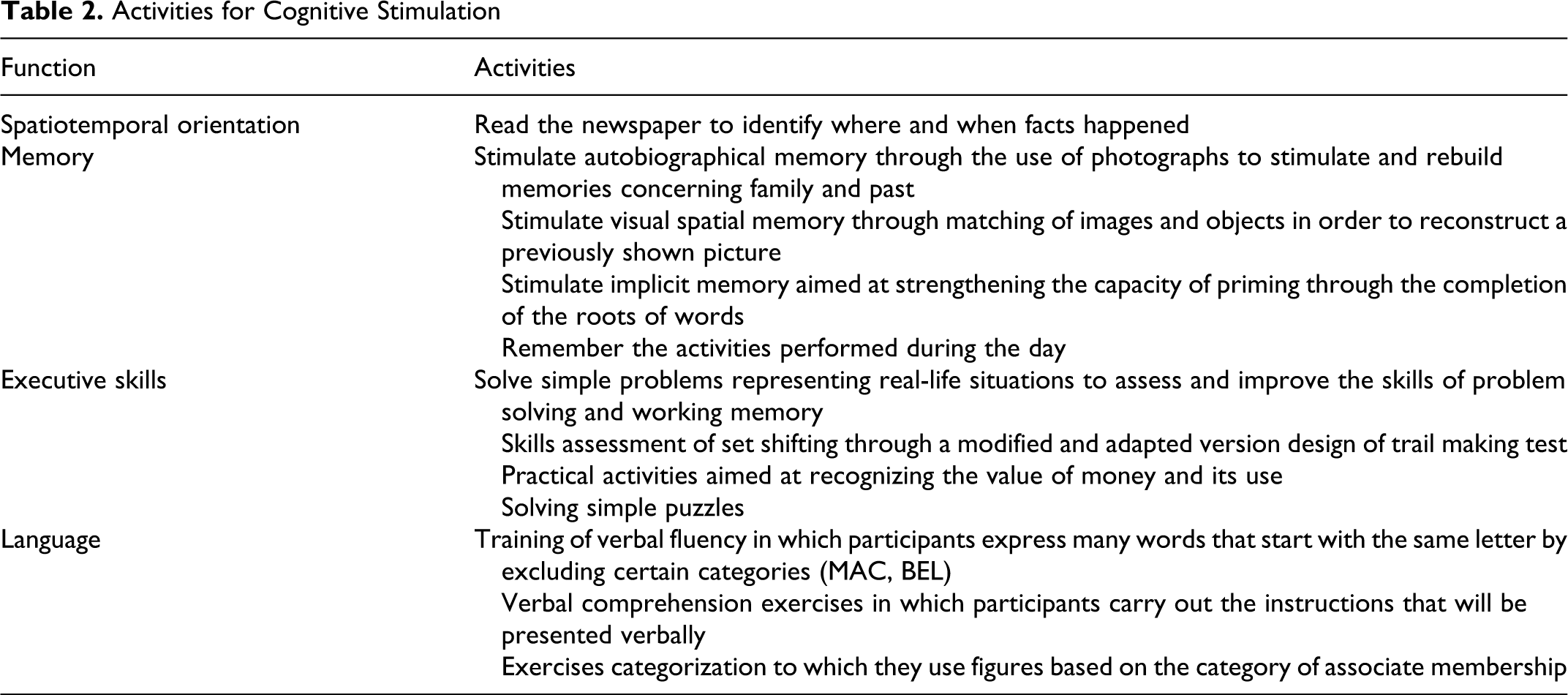
Concerning cognitive stimulation, activities related to enhancement of spatiotemporal orientation, memory, executive skills, and language were performed every day (Table 2). All the exercise indicated in the table were carried out by each patient and then discussed with the psychology and PE students.
Activities for Cognitive Stimulation
Concerning socialization, participants were encouraged to integrate with other participants during transportation from home to gymnasium and vice versa, during the intervals between activities and at the end of the morning during the final group discussion.
Statistical Analysis
Data were analyzed using GraphPad 4.1 software package (GraphPad Software Inc, La Jolla, CA, USA). Data were double entered into the database. Data cleaning was also performed before the data analysis, considering both range and consistence checks. Quantitative variables were described using mean and standard deviation. Due to the small sample size, the appropriate nonparametric tests were performed. In the comparison between treatment and control group, Mann-Whitney test was used, whereas when comparing in each group values at the beginning and at the end of the study, Wilcoxon matched pair test was used. Significance was set at P < .05.
Results
Table 3 shows the main characteristics of patients and their caregivers for both treatment group and control group. The patients and informal caregiver groups were similar and not significantly different for gender, age, education, and severity of dementia (for the patient groups). The caregivers were relatives of the patients (treatment group: 3 wives, 3 daughters, and 1 son; control group: 3 wives, 2 husbands, and 2 daughters). During treatment, all the patients attended the gymnasium every day without missing any session.
Main Characteristics of Patients and Caregivers a
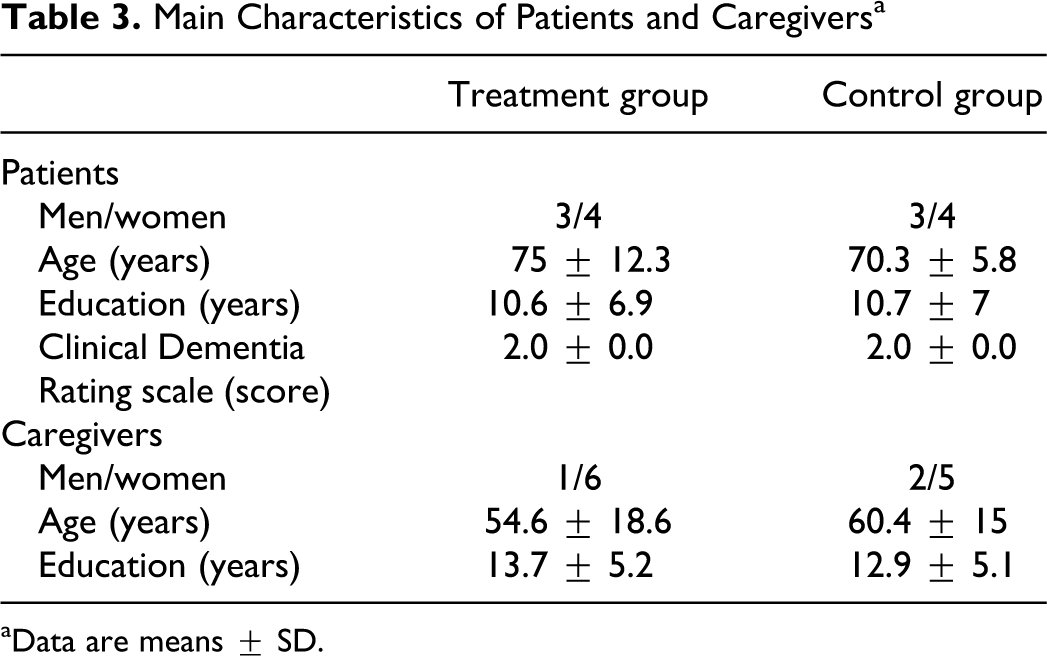
aData are means ± SD.
Scores obtained from neuropsychological evaluation of patients with AD at baseline and at the end of the study are summarized in Table 4. As shown, considering the group of patients assigned to our cognitive and physical activity program, no significant changes in cognitive performances were observed, while we found a significant improvement in apathy, anxiety, depression, and QoL after the treatment. On the other hand, we observed a significant worsening of mood and QoL in the whole group of patients with AD assigned as controls to routine medical practice.
Tests Performances for Patients and Caregivers in Both Treatment Group and Control Group a
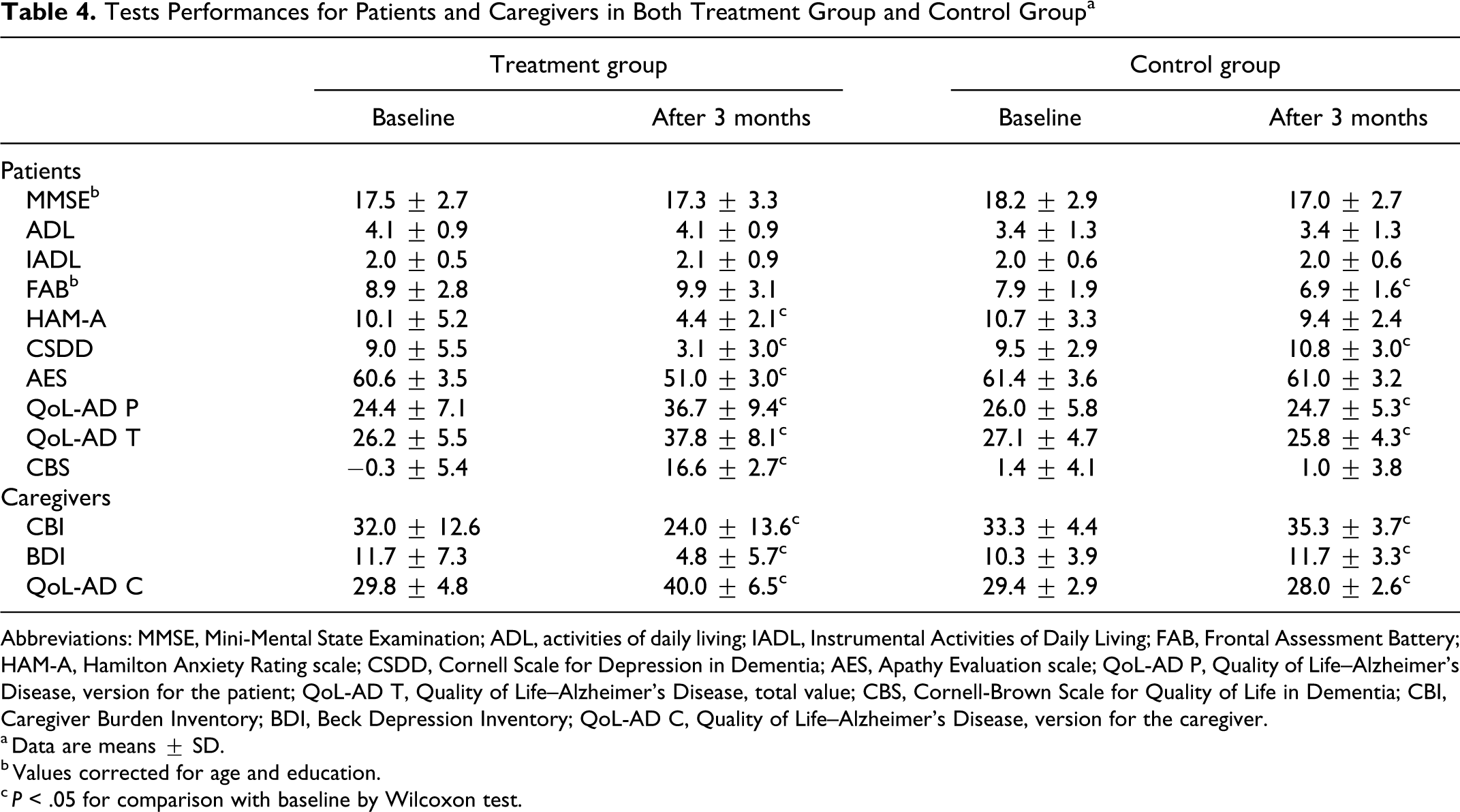
Abbreviations: MMSE, Mini-Mental State Examination; ADL, activities of daily living; IADL, Instrumental Activities of Daily Living; FAB, Frontal Assessment Battery; HAM-A, Hamilton Anxiety Rating scale; CSDD, Cornell Scale for Depression in Dementia; AES, Apathy Evaluation scale; QoL-AD P, Quality of Life–Alzheimer’s Disease, version for the patient; QoL-AD T, Quality of Life–Alzheimer’s Disease, total value; CBS, Cornell-Brown Scale for Quality of Life in Dementia; CBI, Caregiver Burden Inventory; BDI, Beck Depression Inventory; QoL-AD C, Quality of Life–Alzheimer’s Disease, version for the caregiver.
aData are means ± SD.
bValues corrected for age and education.
cP < .05 for comparison with baseline by Wilcoxon test.
Concerning the caregivers, the observed results are also summarized in Table 4. The caregivers of the patients belonging to the treatment group exhibited a significant improvement in their mood and in their perception on patients’ QoL, whereas the caregivers of patients included in the control group showed a worsening of both depression and QoL items.
Discussion
Several studies seem to indicate that physical activity and cognitive stimulation have a positive effect on QoL-AD. 3 –9 Less studied is the caregivers’ burden of care and QoL. 14,17 Starting from these data, our program was undertaken not only with the intent to determine whether physical activity, cognitive stimulation, and socialization were able to act on cognitive parameters but also on mood and on QoL of both patients and their caregivers. Even if other studies had similar approach, the peculiarity of this study is to analyze, with a combined approach, the effect of 3 different stimuli (physical activity, mental activity, and socialization) on the QoL of patients and caregivers. No other studies, to the best of our knowledge, explored simultaneously all the components investigated in our study.
Concerning the results obtained in our patients, we observed that participants submitted for 3 months to our stimulation protocol exhibited a good stability of their cognitive condition, whereas patients of control group displayed a worsening of their cognitive capabilities. Furthermore, the participants of the study group showed a marked improvement in apathy, mood, and QoL when compared with the control group. Our results are in agreement with other reports on multicomponent interventions. 4,14,16 The beneficial effects of our protocol on apathy is confirmed by a recent study 35 that observed positive effects after 4 weeks of cognitive stimulation in probable early stage of AD. Besides physical activity and cognitive stimulation, we underline the importance of socialization as the determinant of our positive results. This aspect has been investigated in a previous report where language exercise plus socialization were able to slow cognitive decline in AD. 20
The caregivers of patients assigned to the treatment group showed an improvement in mood and perception of patients’ QoL. On the contrary, the caregivers of patients forming the control group, who did not undergo the stimulation protocol, exhibited a deterioration of both the affective status 17,14 and perception of patients’ QoL. The differences seen in the caregivers were not surprising, since the treatment group received 20 hours of respite a week, while the participant was in the program and the control group did not receive comparable “time off.”
It is well known that patients with AD, in a high percentage of cases, tend to remain confined at home, gradually losing social contacts and physical autonomy. For patients with AD who have a moderate cognitive impairment, this behavior inevitably leads to a worsening of mood and to a negative perception of their QoL. 36 Moreover, this accentuates the caregiver’s workload, also resulting in them a deterioration of mood and QoL. 37 This study provides experimental evidence that an integrated approach based on cognitive stimulation, physical activity, and socialization experiences is a simple and feasible tool to slow down affective decline in patients with AD and to alleviate the caregivers’ burden of care. Anyway it is not clear whether the observed improvement was due to the physical activity itself or due to the stimulation provided by regular interaction with our staff and other patients. Therefore, it could be interesting to plan interventions evaluating the impact of each component of our program on AD and caregiver’s patients.
We are aware that our study was expensive in terms of both human resources and facilities, even if we were not able to estimate the cost of the GAIA project since the facilities were provided free from our university and people who participated did so for free. On the other hand, our pilot study was developed for assessing the feasibility and the efficacy of the GAIA project, and thus, the costs of the study were not considered in this phase. Nevertheless, because our results showed a clear efficacy deriving from the GAIA project, we believe that the same program could also be replicated in other settings. For instance, by attempting to optimize the resources necessary to carry out a similar protocol, a 3-month period of treatment for up to 15 patients needs no more than 3 psychologists (or other personal trained for cognitive stimulation) and 3 PE experts, under the supervision of 1 neurologist and, possibly, with nurse’s assistance.
In conclusion, our data suggest the efficacy of an integrated approach based on physical activity, cognitive stimulation, and socialization on QoL-AD and their caregivers. Starting from the positive results of this pilot study, we suggest that this protocol applied for a longer period and in larger samples could represent an useful and noninvasive tool for inducing not only an improving of mood and QoL of patients but, possibly, also a slowing of cognitive decline.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.