
Abstract
Background:
Non-pharmacological therapies have been shown to be effective in managing challenging behavior in people with dementia. However, the efficacy of art therapy has yet to be determined.
Objective:
In the present systematic review, we evaluate the efficacy of art therapy as a non-pharmacological intervention for dementia and examine whether art therapy improves wellbeing and quality of life while decreasing biological and psychological symptoms of dementia (BPSD).
Methods:
Research undertaken between 2015 and 2020 was examined and a total of seventeen studies met the specified search criteria, with 853 participants (657 people with dementia, 180 formal and informal carers, and 16 volunteers) involved.
Results:
We identified four outcome domains: wellbeing, quality of life, BPSD, and cognitive function. One or more significant outcomes as having an impact on the efficacy of the intervention were reported in 88% (15/17) of the studies, whereas 17% (3/17) demonstrated significant outcomes across quality of life, wellbeing, and BPSD.
Conclusion:
People with dementia benefit from art therapy. These interventions when incorporating elements of being ‘in the moment’ increase opportunities for communication between people with dementia and their caregiver(s) and facilitate person-centered therapeutic activities.
Keywords
INTRODUCTION
Globally, 47.5 million people are currently living with dementia, and a further 7.7 million will be diagnosed every year, reaching overall to 152 million individuals diagnosed by 2050 [1]. Dementia pharmacological interventions pose clinical challenges which are becoming increasingly harder to ignore. As patients experience various discouraging side effects, a cycle commences of them being non-compliant with taking their medications, and this in turn will affect their clinical symptoms and the response the drug has overall. Consequently, there has been a rise in non-pharmacological and psychosocial interventions available to enhance quality of life, wellbeing and reducing behavioral and psychological symptoms of dementia (BPSD) [2, 3].
Social interactions and activities positively correlate with older people’s wellbeing and physical health [2, 4] which are essential for the retention of personhood. Personhood is also used as an indicator of wellbeing and quality of life for an individual diagnosed with dementia. Kitwood (1997) defines personhood as ‘a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being; it implies recognition, respect, and trust’ (p.8; [5]). The concept of personhood is the core of the Person-centered care model—it states that there is a need for creativity, self-expression, and social interactions in relation to the needs of the individual [2]. It is now a widely adopted model for both dementia care and other clinical care settings instead of the traditional medical model. It builds upon the notion that every individual should have a fulfilled life independently of the health status [5, 6].
Art therapy for dementia
According to The United Nations Declaration of Human Rights Act (1948) Article 27 “Everyone has the right freely to participate in the cultural life of the community, to enjoy the arts and to share in scientific advancement and its benefits” [7]. Creative expression (as stated in [5]) is part of the ten forms of positive interactions that support positive wellbeing in people with dementia. As such, there has been an increase within dementia care services to engage service users with dementia in therapeutic meaningful activities such as art, music, and storytelling amongst others. These activities allow people with dementia to regain a sense of identity and explore new skills safely, that would otherwise not be possible for them.
Art therapy, as defined by The British Association of Art Therapists (BAAT), is a form of psychotherapy that uses art media as its primary mode of expression and communication [8]. Art therapy presents itself in one of two forms, structured or unstructured, and the sessions are subsequently based on these principles. Structural forms of art therapy are those when facilitators pre-determine a theme, materials and how the session will proceed. Structural sessions are considered better for patients with severe dementia, mobility issues or other concerns. In contrast, unstructured sessions are patient led, and people with dementia are encouraged to choose materials, themes and tools without a facilitator.
Art therapy is considered effective because it can be tailored to meet a range of needs for each individual person. For example, it can be used as a tool for communication [9], helps meet the emotional and psychological needs of patients [10], retains skills [11, 12], and encourages the process of reminiscence. Seifert et al. [13] reported that for patients with dementia, art-based interventions lead to improvements in self-esteem, concentration, and memory.
In 2007, the Museum of Modern Art (MoMA) in New York City launched the innovative “Meet Me at MoMA” program. It was the first gallery to make art accessible to individuals with dementia and their caregivers [14]. The aim of the program was to promote public engagement and enhance quality of life through intellectual stimulation, shared experiences and opportunities for social interactions. Subsequently, it inspired a framework for interventions on delivering and creating art programs for people with dementia and their care partners.
Despite the growing interest in non-pharmacological interventions for dementia, there is still a perceived failure to accurately report the efficacy of these interventions. The studies fail especially in the manner in which they report valid and reliable clinical measures which demonstrate how the intervention affects patients, and how patient’s outcome measures are scored and change over time. In the present study, we provide a review of current research in this area, concentrating on both the efficacy of art therapy as a non-pharmacological intervention for dementia and in improving the wellbeing and quality of life for people with dementia.
METHODS
Literature search
We identified peer-reviewed articles published or translated in the English language, between January 1, 2015 and June 1, 2020. We limited the timeframe to capture the most recent and up to date studies. Using a systematic approach set out by the PRISMA guidelines for reporting systematic reviews (PRISMA [15]), a comprehensive search of following electronic databases was conducted: PubMed, EBSCOhost (searching PsycARTICLES, PsycINFO, AMED and CINAHL), and Google Scholar. Initially the terms Art therapy, Art intervention, Music Therapy, and Music Intervention were paired individually with Dementia or Alzheimer’s. Subsequently, the terms non-pharmacological intervention and psychosocial were added to the searches to generate every possible combination.
Selection criteria
The identified articles were individually assessed for inclusion in the present review according to a set criterion. The initial inclusion criteria were as follows: 1) involved individuals diagnosed with any form of dementia, 2) published in a peer-reviewed journal and meeting study design inclusion criteria (see Table 1), 3) identification of treatment and/or exposure to art therapy or music therapy interventions, and 4) containing outcome measures [i.e., BPSD, quality of life (QOL), or wellbeing (subjective or composite)] prior and after the intervention. Articles were excluded if they did not meet the criteria mentioned above in addition to: articles containing combined art-based approaches such as art and dancing, intervention was aimed at caregivers rather than patients and if they did not meet criteria 2 (Table 1). We also decided to extend our exclusion criteria to include articles relating to music interventions, as this both had generated a larger than anticipated scope of research articles and there have already been recent reviews conducted into the efficacy of music-based interventions. The remaining articles included in this review referred to visual arts as defined as the arts of painting and sculpture, rather than literature and music (https://dictionary.cambridge.org/) and did not include ceramic art, printmaking, design, crafts (i.e., knitting, calligraphy, sewing, woodworking, etc.), photography, architecture, film, and video.
Inclusion and exclusion criteria used in the systematic review. The criteria were based on the PICO framework:
Identification of eligible studies
A comprehensive search of the literature yielded a total of 661 studies meeting the search terms. Out of the total of 111 articles eligible for screening meeting the initial inclusion criteria by their title and abstracts, only17 articles from the initial search were eligible for full-text screening and were included in the present review (Fig. 1 for the PRISMA flow diagram of article eligibility). Eligible articles were then coded by contributors according to relevant study characteristics: 1) number of participants, 2) experimental design, 3) clinical measures, 4) effect of QOL and/or BPSD, 5) type of art intervention, 6) benefits to patients, and 7) limitations and implications for future research. Both authors (SYME and EBM-L) reviewed the articles.
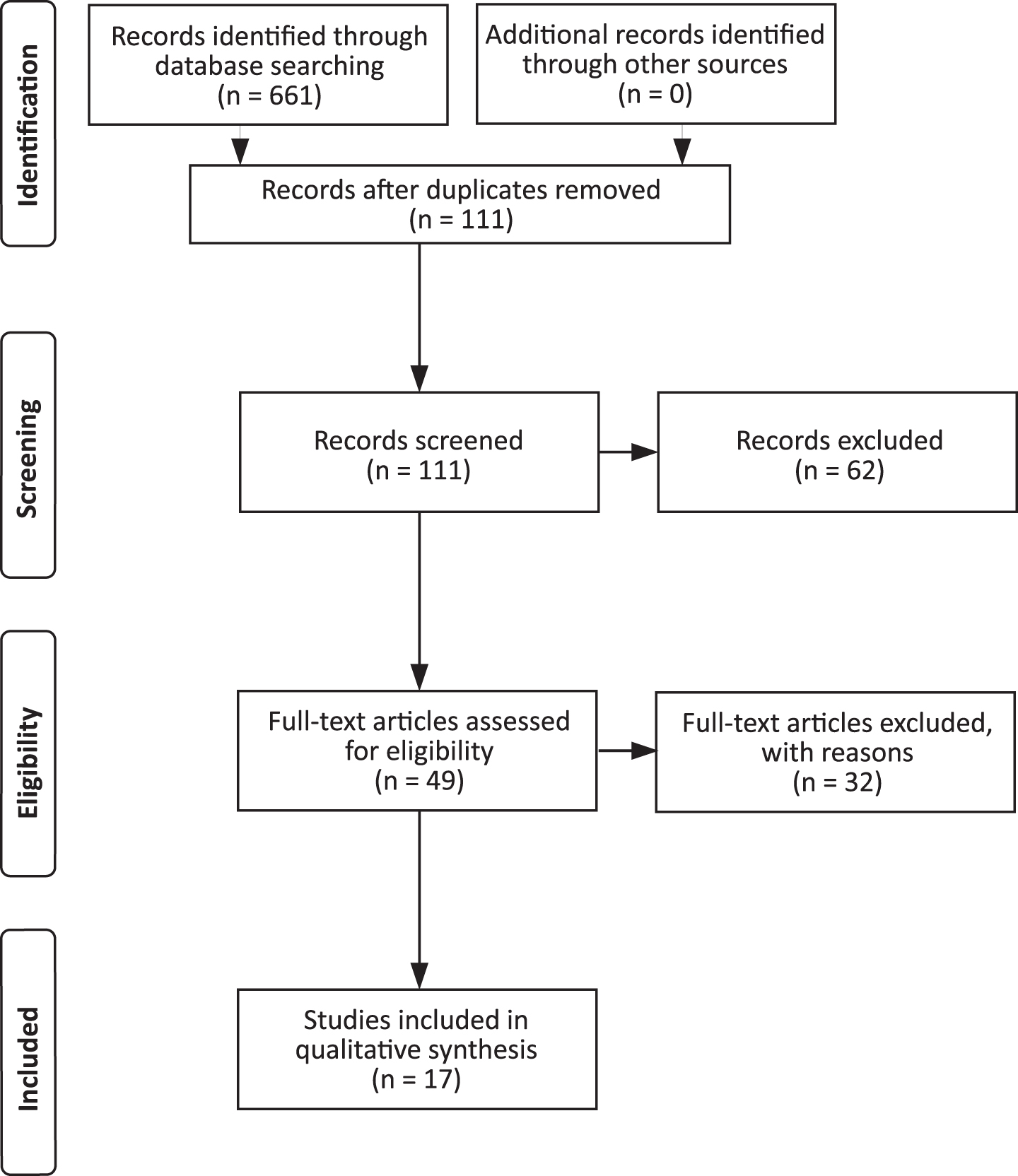
Flow diagram of articles eligibility for inclusion in the current review.
RESULTS
We present a summary of the findings according to creative art interventions, capturing the efficacy of each individual form and the impact it has on patients with dementia (Table 2). A total of 853 subjects (657 people with dementia, 180 formal and informal carers, and 16 volunteers) participated in these studies including two long-term secure care facilities (76 total residents, 54–102 years of age, of which 20 partook in the study; [11]). Across the included studies, we identified three different forms of Creative Art therapy: Visual Art Making (seven studies [11–13, 25]), Art Appreciation (six studies, [3, 23], and a combination of both (four studies [2, 24]) (Table 2). 88% of articles (15/17) reported clinical measures pre-and post-intervention. These studies used quantitative measures of cognition (Mini-Mental State Exam (MMSE); Alzheimer’s Disease Assessment Scale-Cognitive Subscale, Mini-Addenbrooke’s Cognitive Examination), Activities of Daily Living, Neuropsychiatric Inventory, The Cohen-Mansfield Agitation Inventory (a 29-item scale to assess agitation completed by a proxy, i.e., family carer or staff member), Geriatric Depression Scale, outcome measures for quality of life for people with dementia (DEMOQOL) etc. (see Table 2, with the full list of rating scales and assessments completed in the reviewed studies). Graham and Fabricius [11] and Mondoro et al. [21] were the only two of the seventeen studies that used a qualitative approach. Graham and Fabricius [11] protocol consisted of observations and field notes which were later translated and analyzed following inductive thematic analysis. Although Mondro et al. study used a questionnaire, this was to be completed by the caregivers and results were analyzed using thematic analysis [21]. The approach in these two studies enabled extraction of themes, a method which lends itself to capturing the essence of an experience.
Summary of eligible studies
ADAS-Cog, Alzheimer’s Disease Assessment Scale; ADL, Activities of Daily Living; BCRS, Brief Cognitive Rating Scale; BADL, Bristol Activities of Daily Living Scale for dementia; BPSD, Behavioral and Psychological Symptoms of Dementia; CBS, Cornell-Brown Scale for Quality of Life; CMAI, The Cohen-Mansfield Agitation Inventory; CWS, Carer Well-Being and Support Questionnaire; DAS-D, Dementia Attitudes Scale; DEMOQOL, Dementia Quality of Life Instrument; DEMOQOLC, DEMOQOL-Carer; FAHW, Questionnaire of General Habitual Well-being; VAS, Visual Analogue Scale; GCCWBOT, The Greater Cincinnati Chapter Well-Being Observation Tool; GDS, Geriatric Depression Scale; GWQ, General Wellbeing Questionnaire; HCS, Holden Communication Scale; M-ACE, Mini-Addenbrooke’s Cognitive Examination; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; QOL, Quality of Life; QOL-AD, Quality of Life in Alzheimer’s Disease; SFAS, Smiley-Face Assessment Scale; SM-GCCWOT, The Scripps Modified Greater Cincinnati Chapter Well-Being Observational Tool.
Bias in eligible studies
The presence of bias was examined in two ways: 1) as a whole, for the review process and then 2) within each individual article. We looked at how each study reported being impacted by the risk of bias (see Fig. 2 for a summary of the reported biases).
The articles reported several limitations and biases that would have influenced their generalizability and efficacy of the intervention. The limitation that was most often reported among all the studies was the heterogeneity of the analyzed sample. However, this was to be expected with specificity of the condition. Thereafter, in eight of the seventeen studies it was reported that there were instances of selection bias, sample size and gender (see Table 2).
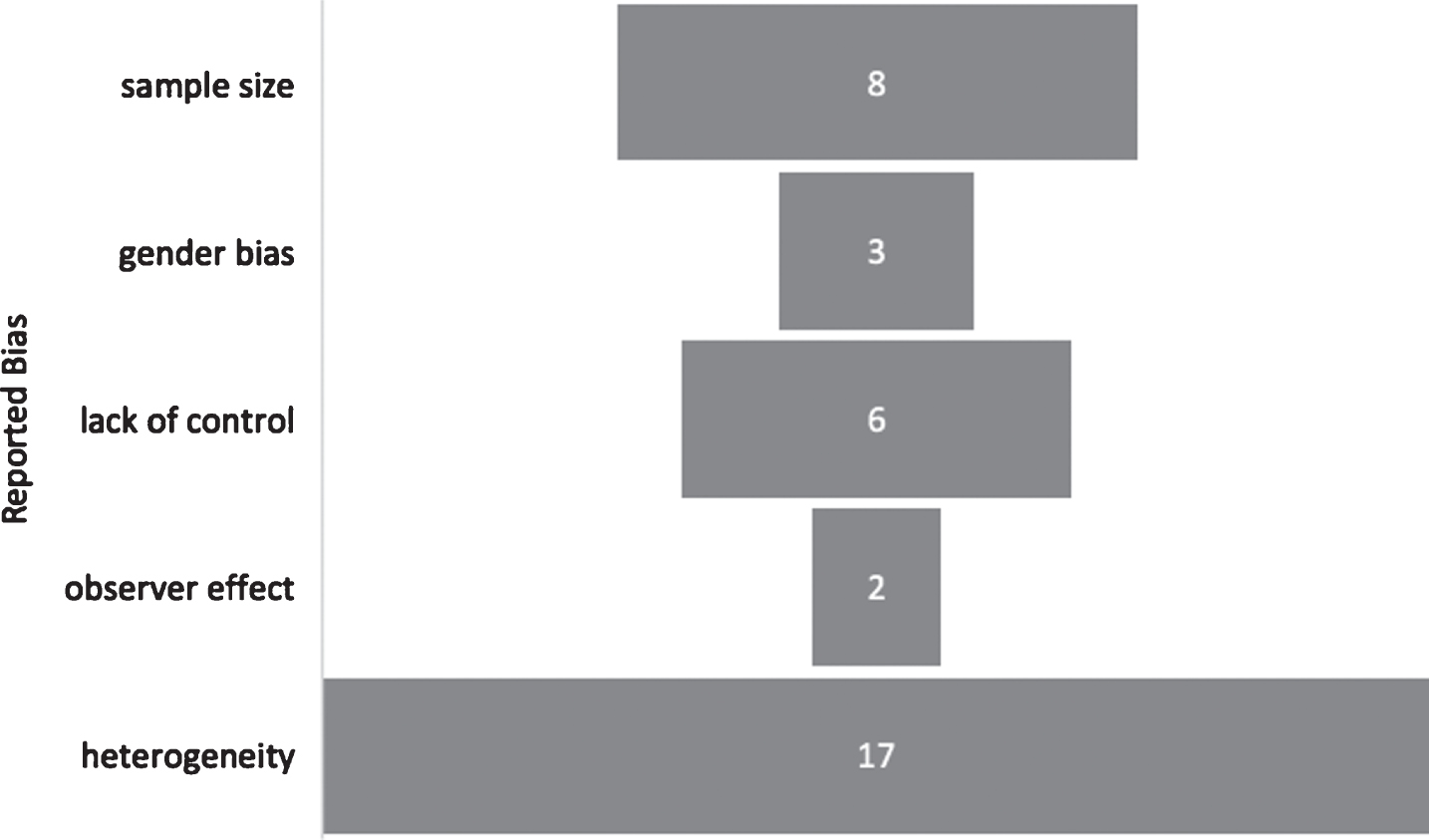
Summary of Report Bias.
Efficacy of creative art therapy
In order to compare the potential benefits of different creative arts interventions we calculated the proportion of studies that reported statistically significant effect/outcome. Fifteen out of seventeen of the studies (88%) reported at least one outcome to be of statistical significance, whereas all three outcomes were considered statistically significant in three out of the seventeen studies (17%) (Fig. 3).
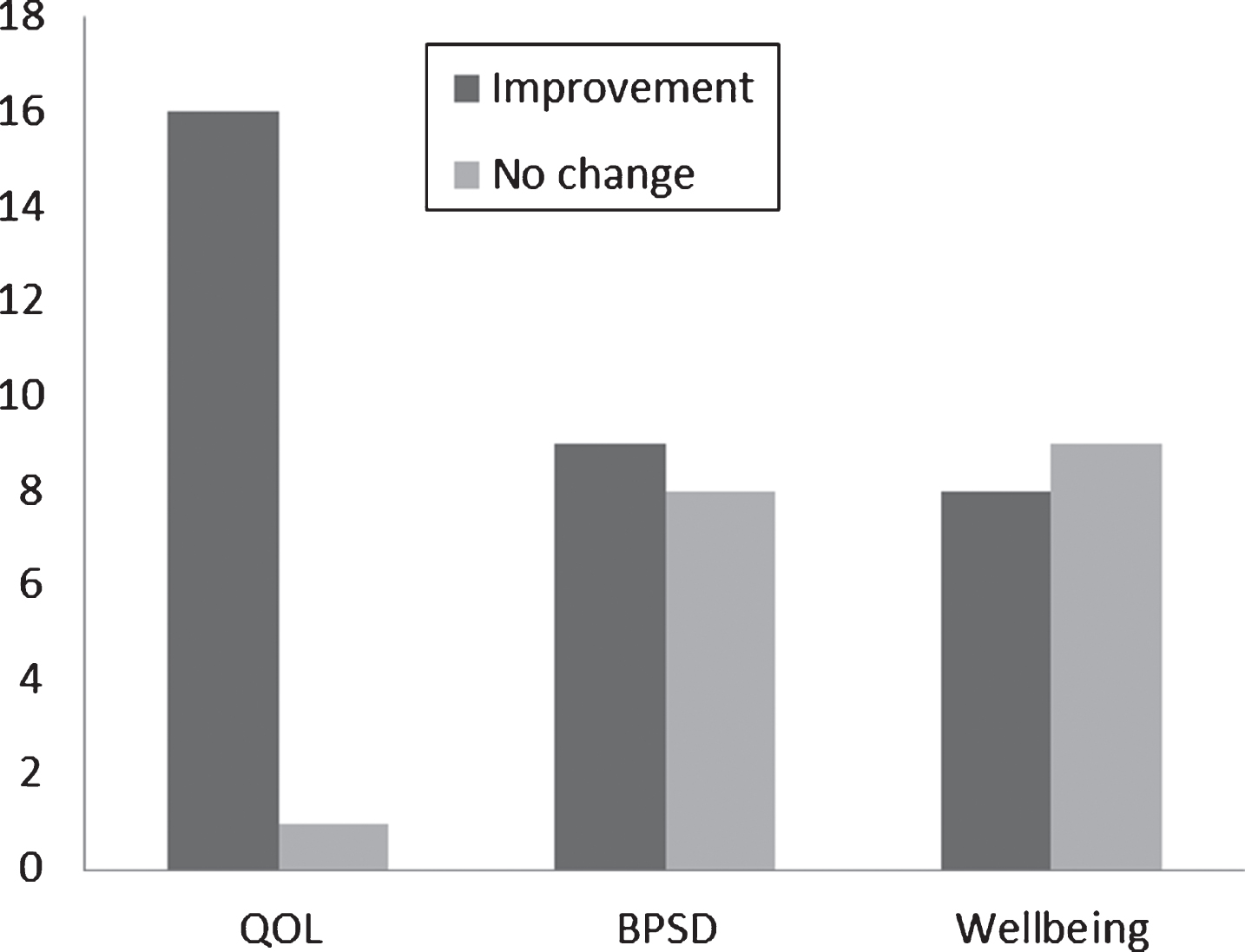
Summary of intervention effects. Columns denote number of studies. QOL, quality of life; BPSD, behavioral and psychological symptoms of dementia.
The following outcome measures were more frequently commented on during creative art interventions: mood (including depression), agitation, well-being, concentration, communication, apathy, motivation, and attention. Of primary interest we decided to focus on Quality of life, wellbeing, and general reduction in BPSD: 16 of the 17 studies (94%) reported improvements in quality of life, 9 (53%) reported reduction in BPSD, and 8 (47%) found improvements to patient wellbeing specifically (Fig. 3). Interestingly, one study reported only positive changes in two specific BPSD symptoms, mood and agitation [4].
Figure 3 demonstrates the general trend in efficacy of creative art interventions, with improving quality of life being most effective, whereas there was no real indication of efficacy in improving wellbeing. It is difficult to make general inferences about the overall impact of creative art interventions on BPSD from the eligible articles since majority of the papers either do not report effects on BPSD or do so inconclusively. Moreover, most of the studies failed to report well-being measures.
Visual art therapy refers to any activity where patients are making or producing art [8]. In the current review, out of the seventeen studies, seven were intervention based around visual art therapy. The majority of these were painting (see Table 2, column six). The exception to this is the Seifert et al. study [13] that used sculpture making to form the basis of their intervention group, while implementing a control group that participated in non-art-based activities. They observed continuous positive improvements in several subscales of wellbeing: mental state and concentration, self-reliance, self-esteem and enhancing individual’s physicality [13]. The results of their stud indicate that the intervention was effective in producing multi-dimensional effects and could potentially improve other areas of psychological functioning.
A small number of studies combined Visual Art Making and Art Appreciation [10, 25]. Art Appreciation encompasses all those interventions whereby art is being viewed in a variety of forms such as galleries or museums [3, 22], tablets [4], and care facilities [10, 25]. Some of the observed benefits are that it allows for people with dementia to reconcile former memories with the artwork being exhibited, thus improving their mood, self-esteem and reducing the strain of caregivers. The studies we reviewed [10, 25] all reported similar findings: meaningful engagements and improvements across clinical measures. All the interventions were able to break the figurative walls of silence and increase communication between caregivers and patients.
DISCUSSION
Creative arts therapies have been investigated as supplementary non-pharmacological interventions for dementia with somewhat conflicting findings. To date, there is no consensus which specific approach of creative art therapy lends itself to be the most effective. As such, this warrants further investigation into which approach is the most effective in alleviating distressing challenging dementia symptoms and improving wellbeing. For the purpose of this review, we have grouped outcome measures together to form coherent themes. In general, the results from this review showed that people with dementia were improving during creative arts therapies across four domains: Cognitive function (included outcomes relating to changes in attention, concentration, and memory); Biological and psychological symptoms of dementia (outcomes relating to changes in motivation, mood, apathy, instances of aggressive behavior or agitation and sadness); Wellbeing with outcomes related or encompassed all subdomains of wellbeing, with outcome measures often redefined for every study; and Quality of life (outcomes relating to changes in communication, fulfilment, engagement as well as general quality of life measures).
One separate theme emerged throughout the data analysis and that was the notion of ‘in the moment’ interventions. Hazzan et al. (2016) program on ‘Artful Moments’ highlighted the feasibility of implementing an art-based intervention in care homes [18]. This study revealed increased levels of engagement between both caregivers and patients, which in turn improved their ability to communicate.
The majority of the studies had one aim, to produce good quality data, whether that be in support or not of evidence-based practice guidelines. Two of the papers from this review discussed novel and innovative concepts: one addressed the possibility of changing how to view art therapy as a global entity [12], whereas the second introduced the idea of testing physiological responses [23]. Ramsey et al. (2018) study outlined a potential new direction for creative art therapy in dementia care [12]. Namely, the proposition is to move away from the concept that creative art therapy should be used as a medical intervention with the purpose of alleviating symptoms and caregiver burden and, instead, incorporate art production as an activity for the purpose of life fulfilment and creative expression [12]. This should lead to the focus being on more person-centered care outcomes such as quality of life and wellbeing [12]. D’Cunha et al. (2019) studied the physiological responses in people living with dementia during art appreciation intervention [23]. They found that elevated cortisol levels were associated with cognitive impairment, whereas diurnal variations in cortisol rhythms were associated with greatest frailty. As participants engaged with the art appreciation intervention their hypothalamic-pituitary-adrenal (HPA) axis function improved. This study is among the few that investigated the impact of creative art intervention upon physiological outcomes, highlighting that the positive effects of art appreciation upon mental and physical wellbeing as re underpinned by dynamic physiological response. Whether this response is sustainable beyond the duration of the intervention (i.e., 6 weeks, [23]), remains to be determined in longer duration studies.
Our study has limitations. Firstly, the study population in the analyzed studies was rather modest (as low as 8 people and did not include a control group [12, 24]). In addition, we identified only one randomized control trial (RCT) study [10]. This was due to the majority of RCTs being on the topic of music. We are aware that this increased the risk of sampling bias as well as any occurrence of detection bias related to the outcome of quality of life. Therefore, without the rigor keenly associated with the process of randomization and concealed allocation in RCTs we are increasing the likelihood of bias. In addition, except for one study that included participants with Alzheimer’s disease only [19], heterogeneity of the dementia etiology appears not to have been considered critical, since the art impact upon the mental attributes, such as mental and cognitive state, was not expected to be dementia subtype-specific [13].
During the review process, it became apparent that it was not possible to review all the literature on art therapies available to patients with dementia. To name a few: music, dance, photography, and writing were among those that were not within the scope of this review. The recent scoping review on creative arts, including visual arts, literary arts, comedy, music, and dance identified only 26 studies [26], providing further support that this field remains largely under researched. Nevertheless, there is strong evidence in support of using participatory and participating arts for both people with dementia [26] and their informal carers [27], irrespectively of the art form. Despite the emerging extensive body of literature over the last five years, there is a lack of consensus in defining quality of life for people with dementia, or what actually encompasses it. During the review process, we decided that all variations of the definition would be accepted as long as studies clearly outlined the definition they utilized in their protocol.
CONCLUSIONS
Retaining the principles of a systematic review we examined the existing knowledge about art therapy for people with dementia. The handful of art studies as an adjunction to standard dementia care (including both pharmacological and non-cognitive/behavioral treatments) although showing some therapeutic efficacy (i.e., upon cognition, affect and emotional well-being, social functioning, behavior, and quality of life) are limited to a small number of participants and have been described of low quality [28]. The latest systematic review, similarly, found art therapy in general or specific art therapies (i.e., performing or creative arts) to have a rather modest cognitive impact on people with dementia [29]. However, all these studies included poorly defined samples, were conducted over a brief period of time (for up to 5–10 weeks), with standardized cognitive tests (i.e., MMSE, ACE-III) used to assess the therapeutic outcomes [29] that may not capture the benefit of treatment in people with dementia over a brief period of time [30]. These shortcomings seem to have been addressed in a most recent randomized control feasibility study conducted on participants with mild cognitive impairment. who were assessed with a more elaborate battery of neurocognitive assessments, including the Rey Auditory Verbal Learning, Delayed Recall and Recognition Trial, tasks from the Wechsler Adult intelligence Scale-3rd edition (WAIS-III), and Colour Trails Test. In this study, participants in the art therapy group had significant improvement in memory domains which were sustained at 9 months [31].
These clinical findings parallel those of neuroradiological and neurophysiological studies that showed reorganization of prefrontal white matter to accompany the visual artistic creativity, i.e., drawing, painting, with multivariate patterns of cortical and cerebellar activity evoked by these tasks [32]. Likewise, activation of prefrontal and parietal lobes was seen in visual artistic creativity (drawing and painting) and aesthetic appreciation of both representational and abstract art, respectively [33]. Similar neuroplastic changes, as demonstrated with enhanced visual and auditory evoked potentials, were recently confirmed in visual and/or music therapy study and these were sustained for up to 3 months [34]. These studies provide further evidence that art provokes plasticity in neural pathways that mediate creative cognition and perceptuomotor integration [32]. More importantly, these studies show the involvement of the fronto-parietal network that is involved in executive function and goal-directed behavior. Bearing in mind that apathy, a decrease in motivation and goal-directed behavior, is the most common neuropsychiatric symptom in people with preclinical [35] and overt dementia [36], art can find its place in both prevention and potential treatment of this syndrome.
In general, many of the studies reviewed here were designed to be observational or as pilot studies opting for the recruitment of smaller samples that met the very specific criteria of the diagnosis. We observed that the mode of delivery had less of an impact on outcome measures then initially assumed. Whether an individual was passively interacting with the artwork itself in an act of appreciation, or actively partaking in developing a piece of artwork seemed to have no influence—it was the creative element of the intervention that had the positive effects on people with dementia.
Viewed as a limitation in many ways as the results cannot be generalized, this form of research is vital in paving the way for future larger studies. Future research would benefit from including larger samples, follow-up after the intervention to measure whether there is a sustained benefit and looking at the influence of intervention on symptom change overtime. It would be beneficial to compare how quality of life changes along the evolution of the disease and how patients respond to creative art therapies. Finally, interventions should look at incorporating more elements of person-centered therapeutic activities and being ‘in the moment’. This will help foster an environment for communication that is meaningful and fulfilling between caregiver and patient dyads.