
Abstract
BACKGROUND:
The ability to reflect on one’s own performance, attitudes, and knowledge is an essential attribute of a competent allied health professional (AHP). Traditionally, reflective practice skills have been fostered during clinical placements via dyadic or narrative means (e.g. face-to-face supervision, journal writing, and observational assessment). However, with the onset of the COVID-19 pandemic, students face reduced opportunities for traditional clinical learning experiences, and embraced telepractice, simulation-based learning and other technology-based learning opportunities.
OBJECTIVE:
Research is limited regarding the use of digital technologies to facilitate the development of students’ reflective practice skills, therefore the best ways to facilitate this novel learning are not fully known and students may be disadvantaged as a result. As such, a scoping review was conducted to identify studies addressing the enablers and barriers to facilitating reflective practice skills of third level healthcare students, including speech and language therapy students, through technological means.
METHODS:
Five electronic databases were searched for studies published between 2016 to 2020. Identified records were imported into Covidence and titles and abstracts were screened by two independent reviewers. Data charting and critical analysis was completed by both authors independently.
RESULTS:
Six studies were ultimately included in data charting. These were of heterogeneous design and mixed quality. Four themes and a range of subthemes were identified regarding enablers and barriers to the facilitation of reflective practice via technological means.
CONCLUSIONS:
This research has provided critical information which may support the future use of technology in facilitating reflective practice among students. Competency in reflective practice is crucial to the professional development of students, yet COVID-19 and resultant restrictions present challenges to implementing the processes traditionally involved in developing such skills. This research highlights potential avenues for future developments in higher education which may overcome these barriers and augment the professional development of students.
Introduction
Accrediting bodies across the spectrum of allied health professions stipulate that registrants must demonstrate reflective practice (e.g. CORU, 2021). Likewise, in third level education of allied health disciplines, reflective practice has been described as a learning tool that supports the development of pre-registration students’ professional and clinical competence (Cook et al., 2019). The emphasis of reflective practice is not on simply pausing to think and problem-solve through the mindset of a technician who is following a list of instructions (Rolfe, Freshwater & Jasper, 2001). Instead, reflective practice affords active attention to self-development and self-growth by analysing and navigating through complex clinical encounters in order to develop new theories of practice to enhance client-centred care (Fook, 2002). Nguven et al. (2014, p. 1176) define reflective practice as “the process of engaging self in attentive, critical, exploratory and iterative interaction with one’s thoughts and actions, and their underlying conceptual frame, with a view to changing them and a view on the change itself”.
Benefits of reflective practice are often personal, including deeper learning, greater self-awareness, acquisition of new knowledge and skills, enhanced critical thinking skills, socialisation into a discipline’s community of practice, and increased confidence (Edwards & Thomas, 2010; Kinsella, 2006; Mann, Gordon & McLeod, 2009). Broader advantages have also been documented in terms of enhanced group dynamics, development of the professional knowledge base, and safer, more equitable and ethical healthcare provision as practitioners are supported to link theory to practice (Caty et al., 2016; Kember et al., 2008; Kinsella et al., 2012; Wald et al., 2009). Reflective practice can assist students to balance their dual commitments of a student who is both scientific and caring (Hinckley, 2010). It can help students to find new ways of making sense of a clinical experience and actively seek and create pathways to address situations that are more complex or challenging (Bay & MacFarlane, 2011). Within the discipline of speech and language therapy (SLT), the importance of reflective practice is stressed by accrediting and professional bodies internationally (e.g. Irish Association of Speech and Language Therapists (IASLT, 2015) and Speech Pathology Australia (SPA, 2011)). Reflective practice has been identified as a method for student SLTs to make sense of new learning and merge it with prior knowledge (McAllister & Lincoln, 2004). It is also considered to support student SLTs to develop new skills to enhance their clinical practice, such as problem solving, clinical reasoning, working through the emotions of difficult clinical experiences, and appreciating the impact of their personal values, attitudes and culture on the client-clinician relationship (Caty et al., 2015; Cook et al., 2019; Hill et al., 2012). Therefore, supporting the development of reflective practice is paramount in order to prepare students for entering the workforce and the realities of modern healthcare where adaptability, advanced problem-solving and critical analytic skills are required (Caty et al., 2016: McGuire, Lay & Peters, 2009).
However, there are numerous documented challenges to supporting the development and assessment of reflective practice. Fundamentally, confusion exists regarding what is entailed in reflective practice (Thompson & Pascal, 2012). For instance, some disciplines construe reflective practice as something measurable that is taught and assessed through positivist and quantitative methods, while other professions tend to view reflective practice as something more constructive in nature and assessed through qualitative methods with greater emphasis on the reflective practice process (Norrie et al., 2012). Moreover, studies have shown that reflective practice takes time to develop, and many educators struggle to facilitate meaningful reflection that is integrated with the rest of the curriculum (Braine, 2009; Cook et al., 2019; McMullan et al., 2003). Other studies indicate that reflective practice can lead to galvanising of students’ existing beliefs rather than facilitating assumptions to be critically analysed (Brockbank & McGill, 1998). It is suggested that reflective practice has become oversimplified as simply pausing for thought and therefore has become divorced from its theoretical aspirations (Thompson & Thompson, 2008). Ethical issues have also been raised when students haven’t been adequately prepared for reflective practice, the learning environment is not conducive for the self-disclosure elements, or confidentiality is not safeguarded (Brown et al., 2013; Fook & Askeland, 2007). ‘Reflection fatigue’ has been reported by some students (Coward, 2011), while others describe conflict when they realise through reflective practice that their own values and beliefs do not conform with those of the organisation and they fear disclosing them (Boud, 2001; Siebert & Costley, 2013).
Some of the former challenges have been addressed through drawing on tried and tested, established frameworks to explicitly teach, facilitate and assess reflective practice.
Frameworks for reflective practice
There are numerous frameworks of reflective practice available to teach and assess reflective practice. The frameworks may be used as a tool to support an individual student’s self-reflection or to facilitate reflective practice with peers, supervisors or critical friends (Norrie et al., 2012). These frameworks have been categorised into those that are iterative or those that are vertical in nature (Mann et al., 2009).
An example of an iterative framework of reflective practice is the seminal and broadly influential work of Schön (1983, 1987) who introduced the term ‘reflective practitioner’ and distinguished between two forms of inquiry: reflection in action and reflection on action. Reflection in action occurs during a clinical interaction, whereby a practitioner’s attention is drawn in the moment to their thoughts, feelings and actions. Reflection on action occurs after the event. Through Schön’s iterative conceptualisation of reflective practice, students are encouraged to engage with concrete problems that can be solved through existing theoretical knowledge and techniques (“high ground”) as well as the messy, unpredictable, nuanced complexities of clinical practice that have no clear technical solution (“swampy lowlands”) (Schön, 1983).
Many additional frameworks draw on Schön’s distinctions and propose cycles of learning that encourage students to evaluate their own practice, including strengths and areas to develop, thereby promoting self-development and direction for future encounters. For example, Kolb (1984) described an experiential learning cycle that includes four elements: concrete experience; reflective observation; abstract conceptualisation; and active experimentation. This cycle stresses the role of reflection in the transformation of a concrete experience to new ideas that can lead to new experiences. Similarly, Gibbs’ (1988) reflective cycle supports students to attend to what happened (i.e. description), what they were feeling and thinking (i.e. feelings), what was good and bad about the experience (i.e. evaluation), what sense they can make of the situation (i.e. analysis) and consider what else they could have done or would do in the future (i.e. conclusion and action plan).
More recently, Wareing (2016) proposed a Me, My, More, Must model of reflection that is more vertical in nature and lists several writing prompts under each stage to facilitate values-based reflective practice. The stages move from individual values and beliefs, to impact of values, to deepen understanding and planning action (e.g. Me: What values are important to me as a person?; My: What impact have my values had on the people involved in this experience?; More: what questions have been generated from this experience; and Must: What values must I explore in order to become the healthcare worker I wish to become?).
Although the former frameworks of reflective practice provide scaffolding and concrete support for healthcare students to move through the stages of reflective practice, the models have been criticised for a relatively underdeveloped theory and evidence-base that underpins them (Priddis & Rogers, 2018; Shea et al., 2016). In addition, criticisms centre on how their intended purpose has been oversimplified and they lack recognition of forethought and the need to plan in advance (Thompson & Pascal, 2012). Others argue that existing reflective practice models fail to take account of the wider social context within which reflective practice is taking place, such as organisational cultural, available reflective space or power dynamics (Fook et al., 2000). Despite these shortcomings, frameworks of reflective practice are the predominant tool used to in the assessment of reflective practice in third level education, including SLT pre-registration programmes (Hill et al., 2012).
Assessing reflective practice
Current available methods of assessment of reflective practice are typically diverse and developed for a variety of objectives. This may be a consequence of the variability in how reflective practice is construed, implemented, and supported. For example, some assessment instruments focus on self-reported capacity and the process of reflective practice (iterative or vertical), while other assessment measures evaluate the product of reflective practice (Phan, 2009; Priddis & Rogers, 2018).
Two predominant assessments tools most frequently used that are focused on the process of reflective practice emerged from a recent systematic review of reflective practice questionnaires and scales for healthcare professionals: the Reflective Questionnaire (Kember et al., 2000) and the Self-Reflection and Insight Scale (Grant et al., 2002; Min Ooi, Fisher & Coker, 2021). The Reflective Questionnaire explores the impact of the teaching and learning environment on reflective thinking over four scales: habitual action, understanding, reflection, and critical reflection (Kember et al., 2000). The Self-Reflection and Insight Scale places its emphasis more on the individual than the environment by evaluating reflective thinking over three scales: engagement in self-reflection; need for self-reflection, and insight.
In parallel, a number of assessment methods are available to examine reflective practice products. A common assessment method is to ask students to submit a written reflection piece such as an essay, report, field note, journal, reflective log, diary entry or presentation (e.g. Hills et al., 2012; Norrie et al., 2012; Roji et al., 2017; Van Winkle, 2016). This written reflective piece may be unstructured and non-guided or semi-structured through writing prompts such as vignettes, case studies, videos, feedback on clinical performance or scaffolding questions (Bruce et al., 2001; Caty et al., 2015; Cook et al., 2019). Written reflective journals are the most frequently administered assessment method of reflective practice documented in third level speech and language programmes (Hill et al., 2012). Portfolios are also a common tool to collate written reflective pieces. Then, written reflective pieces are appraised through qualitative criteria and rubrics that define ‘quality’ reflective practice (Dyment & O’Connell, 2011). For instance, Plack et al.’s (2005) coding schema evaluates written reflective practice pieces across nine domains of breadth (e.g. reflective practice elements over time, content and stage) and three degrees of depth (i.e. an overall skill level categorisation of non-reflector/emerging reflector/reflector). It is argued that such products provide a vehicle for reflection to take place and tangible evidence of reflective practice completed (Lauterbach & Hentz, 2005; Stewart, 2012). However, cautions have been issued that reducing reflective practice to written products promotes a technical viewpoint of reflective practice that contradicts its theoretical foundations and values grades rather than the process of reflection (Eaton, 2016). In addition, two studies focusing on the assessment of student SLT’s reflective practice reported poor inter-rater reliability, highlighting the inherent subjectivity of these forms of assessment (Cook et al., 2019; Hill et al., 2012). To overcome these challenges, it is recommended that educators grade submissions as simply ‘complete’ or ‘incomplete’, design and structure tasks to aid students’ reflective practice, deliver appropriate training in the principles of reflective practice, and provide formative feedback in a timely manner (Hill et al., 2012 Pack, 2014; Wald & Reiss, 2010).
Online reflective practice
As Selwyn (2014, p.7) identified, “digital technologies are now an accepted and expected feature of higher education –part of the everyday furniture of universities rather than an exotic novelty”. Moreover, COVID-19 resulted in a rapid shift to online teaching and learning as over one billion students were unable to physically attend university (UNESCO, 2020). This global pandemic has provided a catalyst for third level education to quickly transition to remote online teaching and to reconceptualise traditional assessment measures of reflective practice to alternative online assessment approaches. Consequently, online tools that were implemented in the past to support the teaching and assessment of reflective practice have been in high demand and introduced to increase flexibility and to engage students who are geographically dispersed (e.g. Phillips & Morrow, 2008).
It has been suggested in the past that digital platforms for reflective practice may engage more students using modern, interactive, multi-media technologies such as blogs, wikis, podcasts, or videos (Sandars & Murray, 2009). In addition, it was reported that online media for supporting reflective practice are often more active, contextual, collaborative, and multidimensional (Gikandi et al., 2011). For example, ePortfolios were found to be portable, easy to share, and increased the efficiency of learning for students (Bate et al., 2016). Some disciplines have used existing university virtual learning environments to house online reflective practice activities and assessments (Pack, 2014), while others have employed open-source software such as WordPress or Mahara (Avila et al., 2016; Maher & Gerbic, 2009) or commercially available packages such as Taskstream or Chalk & Wire (Batson, 2002; Lorenzo & Ittleson, 2005). However, many existing studies of online reflective practice tools are focused on students of medicine and nursing (e.g. Hall et al., 2012; Levine 2014; Ross et al., 2009) and not students of allied health professions such as SLT, whose structure, focus, and discipline-specific competencies differ from medical and nursing colleagues (McAllister et al., 2011).
Aims
This scoping review was conducted in order to systematically map the research completed on facilitating reflective practice skills of third level allied health students through digital and technological means. In addition, we aimed to identify factors that facilitated and supported online reflective practice (i.e. enablers) as well as factors that hindered or presented challenges to online reflective practice (i.e. barriers). Ultimately, our objective was that the former synthesis of the literature would help inform future blended approaches to curriculum design and delivery that intend to develop students’ reflective practice skills.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement for Scoping Reviews (Tricco et al., 2018) informed the conduct of this scoping review. The protocol for this review was prospectively published on the Open Science Framework database (Registration number: DOI 10.17605/OSF.IO/8NFMV).
Eligibility criteria
Eligible studies
Randomised and non-randomised, published and unpublished reports investigating the enablers and barriers to facilitating reflective practice for practice education through technological means for third level allied health professional students were eligible for inclusion, with no language, geographic, or study design limitations. Studies published in the last 5 years were eligible for inclusion to ensure that the technology solutions employed were contemporaneous.
Eligible participants
Participants who were educators of allied health professional students within a third level institution, or allied health professional students, were included with no other professional or qualification limitations. The allied health professions included were speech and language therapy, occupational therapy, physiotherapy, radiation therapy, play therapy, audiology, clinical biochemistry, clinical engineering, clinical measurement, clinical perfusion science, counselling and psychotherapy, dietetics, medical physics, optometry, orthoptics, phlebotomy, podiatry, radiography, social care and social work. These professions were selected according to the Health Service Executive of Ireland’s categorisation of health and social care professions (HSCP) (HSE, 2021). Studies were excluded if participants were not educators or students of one of the former allied healthcare professions.
Information sources
The following databases were searched from 01/01/2016 to 09/11/2020 by both authors: Medline, PubMed, CINAHL, Web of Science, and Science Direct. Grey literature was not searched due to time and resource limitations. Further information was sought from authors of primary studies when required (e.g. for article access or access to missing data) using a standardised email template.
Search
A systematic search strategy was developed by both authors, with initial application to PubMed, and adaptation subsequently for use in other databases listed. Search limits regarding publication date were implemented during the screening phase to ensure that contemporaneous technological methods were found, with articles published in the last 5 years only included (2016–2020). No other language or location of study or publication restrictions were applied. The reproducible search string for Pubmed (09/11/2020) is outlined in Fig. 1.
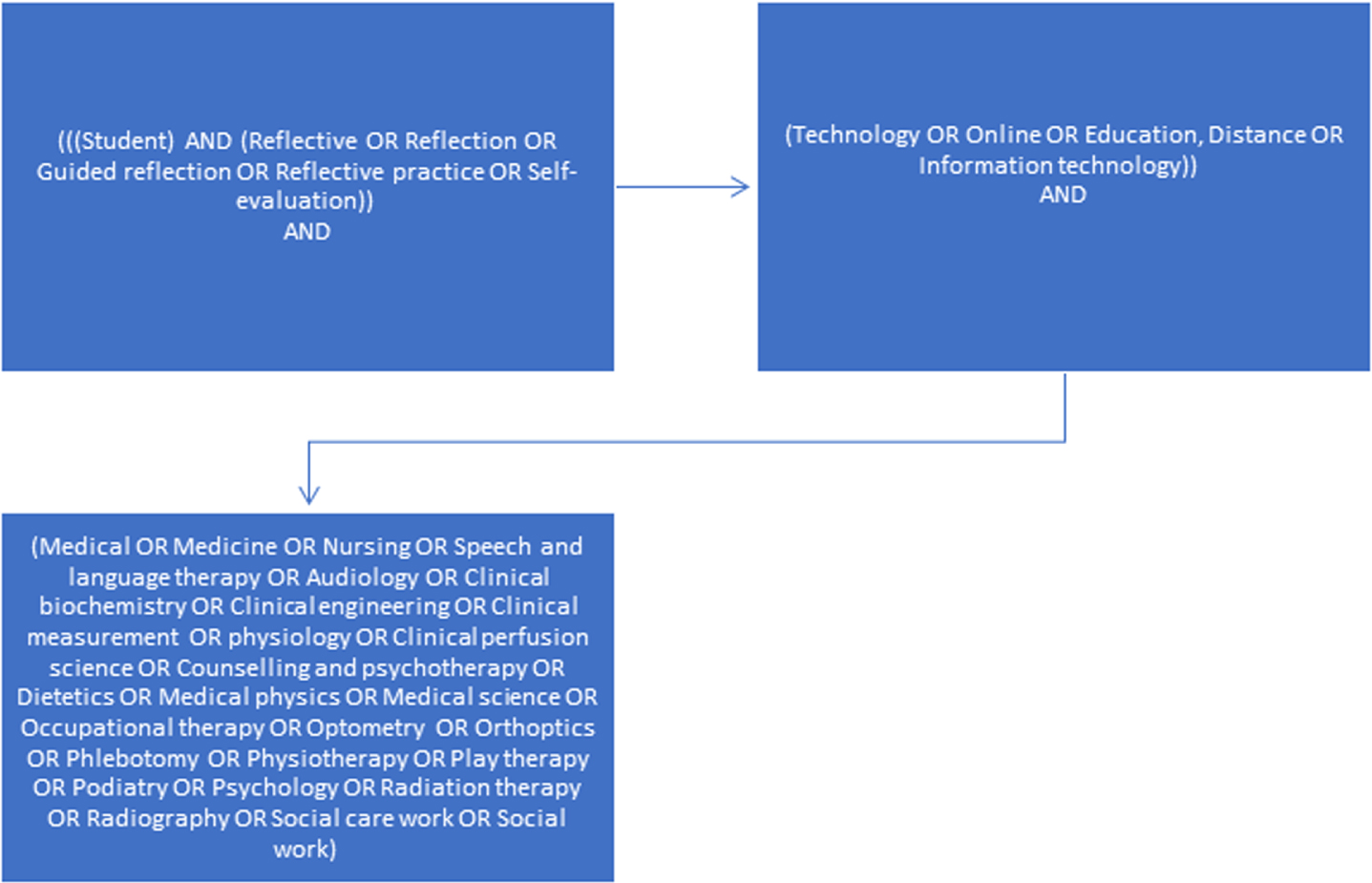
Search string.
This search returned 3076 results in PubMed on the day of searching. Although these professions were not the focus of this search, terms pertaining to “medicine” and “nursing” were still included to capture research where one of the included professions were recruited as part of a larger study which targeted all medical, nursing and allied health professions.
The titles and abstracts of all potentially relevant records identified via the database searches were exported to the Zotero platform (Roy Rosenzweig Center for History and New Media, 2016), with subsequent exportation to the Covidence platform (Covidence systematic review software, 2020) for automatic duplicate deletion and title-abstract and full-text screening. Both authors independently screened all records across both title-abstract and full-text screening, with 100% agreement. A third independent researcher was available to mediate results if required, although this option was ultimately not required. Those which did not meet the objectives of the review were excluded, while those which were appropriate were included for data charting and synthesis.
Data charting process
An adapted version of the Joanna Briggs Institute template (The Joanna Briggs Institute, 2020) and the Covidence data extraction template (Covidence systematic review software, 2020) was used to chart data by the two authors. This data charting form was continuously reviewed and iteratively updated in response to emerging data from the included studies. Each author charted data from 50% of included studies, with subsequent discussion and cross-checking to ensure reliability and agreement, with agreement reaching 100%.
Data items
Data items charted here included: general study details (e.g. author, title, year, language, aims, sponsorship source, country), methodological details (e.g. study design, setting, participant demographics, sampling, recruitment, eligibility criteria, ethical approval, method of data analysis), details of online reflective practice tools (e.g. reflective practice tool used, online platform, details of reflective practice activities facilitated online) and outcomes and conclusions. In line with Levac and colleagues’ (2010) suggested enhancements to the original Arksey and O’Malley (2015) framework, thematic analysis was used at this stage to support and bolster the data charting process (Peters et al., 2015; The Joanna Briggs Institute, 2015). This thematic analysis was conducted in line with the established Braun and Clarke (2014) thematic analysis framework.
Critical appraisal of individual sources of evidence
While critical appraisal of individual sources is not mandatory within scoping reviews (Lockwood et al., 2019; Munn et al., 2018), research suggests that such assessment can strengthen the value of a scoping review, especially if critical appraisal on the topic of interest is lacking (Sucharew & Macaluso, 2019), as is the case here. Critical appraisal of evidence was approached here with flexibility, in line with the underlying framework of the scoping review study design. This allowed for selection of study design-specific tools to ensure that the potential for unique bias across designs was accounted for, as opposed to using one generic tool. For mixed-methods studies, the Mixed Methods Appraisal Tool (MMAT) [National Collaborating Centre for Methods and Tools, 2015) was used, whereas the Centre for Evidence-based Management (CEBM) Survey Tool (The Centre for Evidence Based Medicine, 2020) was used for descriptive survey research, and the CEBM Qualitative Tool (The Centre for Evidence Based Medicine, 2020) was used to appraise the quality of qualitative research.
Synthesis of results
Data were initially synthesized using narrative methods and thematic analysis on Microsoft Word and Excel. Descriptive statistics were then used to subsequently explore data using Microsoft Excel. Data were displayed using accessible graphs and charts to visually synthesise findings.
Results
Selection of sources of evidence
A total of 6411 results were found in the original search (see Fig. 2). Using the Covidence platform, 1424 duplicate records were automatically excluded. Both authors independently screened the titles and abstracts of all remaining 4987 records using the Covidence platform (Covidence systematic review software, 2020), with 4565 obviously irrelevant results excluded at this stage. In total, 422 full-text records were examined by both authors, with 416 records excluded due to various reasons (Fig. 2). Subsequently, six studies were deemed eligible for inclusion in the final analysis.
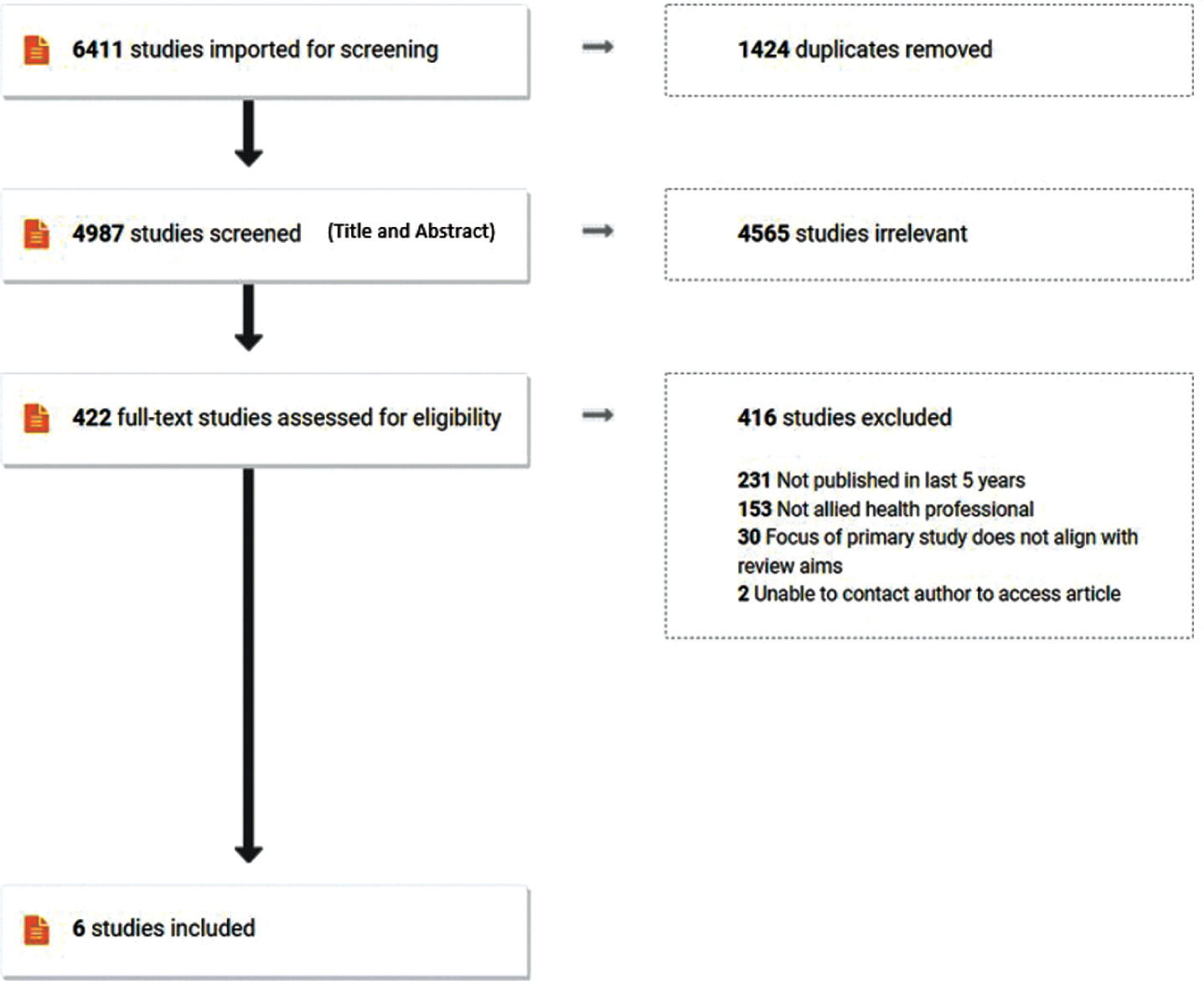
PRISMA flow diagram.
As demonstrated in Table 1, the included studies were published over a 3-year period (2016–2018), with region of origin spanning Europe, North America, and Australasia. The study designs of these articles spanned mixed methods studies (Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018), descriptive survey research (Urpi-Sarda et al., 2016), action research (Thompson, Smythe & Jones, 2016), and qualitative research (Cohn & Plack, 2017; Finger-Ossinger & Löffler-Stastka, 2018). The majority of studies aimed to describe differing aspects of the implementation of online technology to facilitate reflective practice (Table 1).
General characteristics of included studies
General characteristics of included studies
Study locations were HEIs, with one study also partnering with a local hospital (Thompson, Smythe & Jones, 2016) (Table 2). With regards to sampling methods, convenience sampling methods were used in 4/6 studies (Cohn & Plack, 2017; Cleveland, 2018; Finger-Ossinger & Löffler-Stastka, 2018; Hanbidge, McMillan & Scholz, 2018), while 2/6 did not specify the methods used (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016). Similarly, recruitment methods were under-specified, with only 2/6 providing details (Thompson, Smythe & Jones, 2016; Hanbidge, McMillan & Scholz, 2018). All included studies provided details of inclusion criteria, focusing primarily on students enrolled in professional allied health courses, with two studies also recruiting practising AHPs (Thompson, Smythe & Jones, 2016; Hanbidge, McMillan & Scholz, 2018). However, no included studies specified exclusion criteria.
Demographic characteristics of participants within included studies
In total, 172 students and 14 AHPs were recruited across all included studies. Students were studying a range of courses including medical imaging technology (MIT) (n = 4) (Thompson, Smythe & Jones, 2016), nutrition and dietetics (n = 46) (Urpi-Sarda et al., 2016), physical therapy (n = 40) (Cohn & Plack, 2017), counselling n = 30) (Cleveland, 2018), psychotherapy (n = 41) (Finger-Ossinger & Löffler-Stastka, 2018), and medical social work (MSW) (n = 11) (Hanbidge, McMillan & Scholz, 2018). Practicing clinicians were recruited from MSW (n = 10) (Hanbidge, McMillan & Scholz, 2018) and MIT (n = 4) (Thompson, Smythe & Jones, 2016).
The reflective practice tools used in included studies were primarily ePortfolios (4/6) (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018), Word Clouds (1/6) (Cohn & Plack, 2017) and Online Essays (1/6) (Finger-Ossinger & Löffler-Stastka, 2018), and the use of these tools was facilitated via a range of online platforms, and data collected via a range of heterogeneous methods (Table 3). A range of reflective practice activities were facilitated across included studies, as shown in Table 3. Commonalities across studies were that the majority were compiled within a multi-media learning portfolio with frequent information required within the reflections including: background/personal information portfolio (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cleveland, 2018), details of the management of patient cases (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Hanbidge, McMillan & Scholz, 2018), and targeted clinical reflection activities (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018). Within the realm of portfolios, other less frequent prompts included: descriptions of the context of clinical placements and common practices within these settings (Urpi-Sarda et al., 2016; Cleveland, 2018); prompts for practice and/or additional clinical resources (Thompson, Smythe & Jones, 2016; Cleveland, 2018); and explicit discussion/documentation of formal competencies achieved during placement (Hanbidge, McMillan & Scholz, 2018). Within studies which did not include such e-portfolios (Cohn & Plack, 2017; Finger-Ossinger & Löffler-Stastka, 2018), reflective prompts focused on the iterative development of a concept of “professionalism” (Cohn & Plack, 2017) and one’s own personality development via the generation of Word Clouds, acquired theoretical knowledge, and practical experience via the generation of online essays (Finger-Ossinger & Löffler-Stastka, 2018).
Characteristics of reflective practice activities within included studies
Three studies provided initial formal training in the use of online reflections for participants (Urpi-Sarda et al., 2016; Hanbidge, McMillan & Scholz, 2018; Cleveland, 2018). With regards to the timing of reflection submissions, three studies had a rolling submission throughout placements and across semesters (Thompson, Smythe & Jones, 2016; Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018), with two studies having two timepoints for submission: before and during placement (Urpi-Sarda et al., 2016) and across two semesters (Cohn & Plack, 2017), while one study sought reflections after attending a course (Finger-Ossinger & Löffler-Stastka, 2018). With regards to the provision of external feedback to learners, two studies did not explicitly discuss the feedback process (Urpi-Sarda et al., 2016; Finger-Ossinger & Löffler-Stastka, 2018). Cohn and Plack (2017) discussed an informal formative feedback process in which the Word Clouds generated in Semester one were used to prompt a discussion of what “professionalism” means, although feedback on the second Word Clouds was not discussed in the article. Feedback provision was differentiated within Cleveland’s (2018) study, with one group provided with weekly formative feedback on reflections via completion and sharing of marking rubric, while the other group was provided with summative feedback on one occasion at end of the semester. Finally, Thompson, Smythe and Jones, (2016) provided iterative feedback within a formalised five-step supervisory framework, which incorporated formative case-based discussion, observation, questioning and clarification, and review of the student’s practice, among other facets.
While results of included studies were primarily qualitative (Table 4), some quantitative results were also posited (Table 5). Quantitative results related to broadly to the development of reflective skills in response to use of the online tools (Finger-Ossinger & Löffler-Stastka, 2018), the ability of students to reflect on changes in their conceptualization of professional topics (Cohn & Plack, 2017), and response of students to isolated summative versus regular formative feedback (Cleveland, 2018). Urpi-Sarda et al. (2016) presented primarily quantitative findings, overall focusing on the student’s low level of prior knowledge of and experience with ePortfolios, yet their subsequent positive response to the use of this tool, its ease of usage, and its positive impact on their learning as compared to other, more traditional methods of documenting learning.
Qualitative Outcomes of included studies
Quantitative Outcomes of included studies
Qualitative findings relating primarily to the use of online reflective practice activities may be synthesised into four overall themes, with a range of sub-themes also identified: Theme 1: Enablers of online reflective practice activities on student learning (seven subthemes): Deep and active patient-centered learning: Most studies reported that through the completion of these online reflective activities, students developed a greater level of patient-centered clinical knowledge and skills (Cohn & Plack, 2017), with improved levels of active engagement in this learning (Cleveland, 2018) Social learning: Unlike traditional individual summative assessments, some students reported that being able to review peers’ work, being able to engage over the virtual platforms, and attending training webinars in the use of these activities facilitated greater inter-connectivity and social learning when compared to traditional learning (Hanbidge, McMillan & Scholz, 2018; Finger-Ossinger & Löffler-Stastka, 2018) Creativity in problem solving: The use of non-traditional learning methods was a driver for the development of creativity, with students able to personalise their submissions in a manner which suited their unique learning strengths (Hanbidge, McMillan & Scholz, 2018; Cleveland, 2018) Flexible monitoring and communication of one’s own progress and potential: Overall students reported flexibility and ownership while engaging in online activities (Cleveland, 2018). These activities allowed students to actively review and monitor their progress in learning, which was beneficial in building confidence (Thompson, Smythe & Jones, 2016), and acted as a resource when searching for jobs and attending interviews (Cleveland, 2018) Virtually seeking clarification/help: Some students reported greater access to clarification/additional support from their supervisors via the online format, as opposed to waiting for traditional class discussions (Thompson, Smythe & Jones, 2016) Efficiency in learning to use tool and ease of organization of learning materials: Some students reported ease in engaging with online reflective practice activities, with associated high levels of satisfaction in the use of the online platforms to organise their clinical reflections and learning resources (Urpi-Sarda et al., 2016) The provision of a more holistic viewpoint of a student’s competencies: Some students cited that in comparison to traditional summative assessments, the online reflective activities allowed for the creation of a more holistic viewpoint of their competencies, with inclusion of experiential, personal, and integrative aspects of learning which may have previously been overlooked (Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018) Theme 2: Enablers of online reflective practice activities on teaching and supervision (two subthemes) Improved efficiency in the feedback process: The process of providing summative and formative feedback to students on their online reflections was reported to be efficient and completed with ease via online platforms (Urpi-Sarda et al., 2016). This led to more manageable workloads for educators (Cleveland, 2018), with greater visualisation of learning and feedback facilitated, improved sharing of feedback among stakeholders, and increased depth of reflection and application of learning (Urpi-Sarda et al., 2016; Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018; Thompson, Smythe & Jones, 2016) Educators were motivated to continue their own CPD via use of online reflective practice activities: Some supervisors reported that using the new technology highlighted their own CPD needs and prompted them to upskill in this area, which was subsequently beneficial to their overall practice (Thompson, Smythe & Jones, 2016) Theme 3: Barriers to students using online reflective practice activities (two subthemes) Need for greater training and ongoing support when engaging in online reflective practice activities: Hanbidge, McMillan & Scholz (2018) reported that some students required a greater level of pre-training and ongoing support to: effectively understand the intended learning outcomes; engage in these activities; overcome technical difficulties, and to connect learning from the reflective tasks to other course modules, especially among those with lower comfort levels with technology use (Hanbidge, McMillan & Scholz, 2018) Issues with the receipt of feedback: Hanbidge, McMillan & Scholz (2018) also flagged that technological issues can disrupt the smooth and effective provision of feedback on their reflections, with additional input in this area advised Theme 4: Barriers to educators using online reflective practice activities (two subthemes) Additional time commitments: While most academic educators reported that the use of online activities were efficient, Thompson Smythe and Jones, (2016) discussed that when clinicians are involved in provision of feedback, they found themselves working additional hours to do so, which was deemed by some to be too time-consuming Need for greater training and ongoing support: A cohort of clinical educators reported that they required additional training in the effective use of online reflective activities and online platforms to adequately provide feedback to students, citing that peer-training from experienced colleagues may be helpful to facilitate this training (Hanbidge, McMillan & Scholz, 2018)
These findings led the authors of included studies to conclude that the use of online reflective activities, although heterogeneous in their nature, was valuable in supporting overall teaching and learning (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cohn & Plack, 2017), and helped students to: develop reflective skills (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cohn & Plack, 2017; Cleveland, 2018; Finger-Ossinger & Löffler-Stastka, 2018; Hanbidge, McMillan & Scholz, 2018) develop critical thinking skills (Urpi-Sarda et al., 2016) increase student’s meta-cognition in relation to their own learning (Cleveland, 2018) enhance professional communication skills by describing their reflections on their own clinical skills (Cleveland, 2018) embed reflection on competency and performance as an everyday clinical activity (Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018)
However, some authors also cautioned that the ongoing use of such online reflective activities must be supported by greater training for and monitoring of educators as well as students completing the assessments (Thompson, Smythe & Jones, 2016; Hanbidge, McMillan & Scholz, 2018) and embedding of quality assurance into the future development and use of such online reflective practices (Cleveland, 2018).
Critical Appraisal of Qualitative Studies based on the CEBM Qualitative Tool (The Centre for Evidence Based Medicine, 2020) (Green = yes; red = no; Orange = unclear)
Both authors independently reviewed half of included studies each (3/6), with appraisal results subsequently cross-checked, discussed, and agreed upon. Due to the heterogeneous study designs utilised within included studies, a variety of critical appraisal tools were required to ensure that appropriate criteria were considered, as discussed above (see Tables 6, 7 and 8). Items contributing to positive ratings across all study type included clarity within research questions and aims, alongside the appropriateness of the study design and methods of data processing selected. The main items responsible for lower ratings of methodological quality across all study types were the lack of clarity regarding potential bias within the representativeness of sampling and recruitment methods, the true validity and reliability of data collection tools, and the potential role, influence, and reflexivity of researchers.
Critical Appraisal of Mixed-methods Studies based on the Mixed Methods Appraisal Tool (MMAT) [National Collaborating Centre for Methods and Tools, 2015 (Green = yes; red = no; Orange = unclear)
Critical Appraisal of Mixed-methods Studies based on the Mixed Methods Appraisal Tool (MMAT) [National Collaborating Centre for Methods and Tools, 2015 (Green = yes; red = no; Orange = unclear)
Critical Appraisal of Descriptive Survey Studies based on the Centre for Evidence-based Management (CEBM) Survey Tool (The Centre for Evidence Based Medicine, 2020) (Green = yes; red = no; Orange = unclear)
In this study, a scoping review was conducted to explore the existing literature on the enablers and barriers to facilitating the development of reflective practice skills of third level healthcare students through technological means. A comprehensive and exploratory approach to searching the literature was conducted, with six studies ultimately included in the narrative synthesis. While a range of enablers and barriers were identified which will provide direction for future research and practice, results must also be interpreted with caution due to limitations within the process and product of this scoping review.
Key findings of this study indicated that there is limited available evidence regarding the use of online technology to facilitate reflective practice within pre-registration third level education, thus suggesting an area of future research need. None of the included studies were conducted with student SLTs reinforcing this gap for the SLT profession. It is notable that many studies were excluded as they were conducted by non-AHP professionals, for example within medical and nursing disciplines. This suggests that SLT and other AHP fields could benefit from investigation and emulation of the work conducted in other healthcare disciplines. In addition, many studies were excluded as they were published more than five years ago, suggesting that little research in this area has been conducted with emerging and developing technology, potentially indicating areas for subsequent investigation. Building on this point, it was noticeable that most included studies primarily referenced standard ePortfolios (Thompson, Smythe & Jones, 2016; Urpi-Sarda et al., 2016; Cleveland, 2018; Hanbidge, McMillan & Scholz, 2018), or essays (Finger-Ossinger & Löffler-Stastka, 2018). While some of these methods allowed for uploading of clinical artefacts or multimedia data, many of the features included in these studies could have been conducted on- or off-line (e.g. hand-written clinical reflections, essays, competency forms). Only one included study (Cohn & Plack, 2017) referenced the use of novel methods in collecting reflections, via the selection of word clouds. It is advised that future research investigates the unique features that technology may offer to this area, such as the use of video or voice recordings, the creation of innovative clinical resources online, or the use of increased connectivity to facilitate active and deep learning across disciplines and geographic locations in real-time. For example, using digital technology to facilitate reflection in action as well as reflection on action as promoted by Schön 1987), which are equally important with SLT clinical practice that is rooted in interpersonal relationships in the therapeutic moment (Hill et al., 2012). Finally, it was noticeable that studies differed greatly in their timings of reflective submissions (e.g. before, during, after placement), the methods of providing feedback to learners (e.g. verbal, written), and the means and purpose of assessing (e.g. corrective feedback/forensic diagnosis, or feedforward feedback) (Price et al., 2010). It is essential that the influences of such factors are explored within future research, in addition to consideration of the impact of assessor relationships, dialogic methods, and definitions of effectiveness, among other key components of reflective feedback provision (Price et al., 2010).
It was noticeable in this study that the enablers and benefits of facilitating online reflective practice resembled those listed for “traditional” methods of reflective practice, including deep learning, increases in critical thinking, and improved linking of concrete clinical learning to theoretical concepts (Edwards & Thomas, 2010; Kinsella, 2006; Mann, Gordon & McLeod, 2009; Caty et al., 2016; Kember et al., 2008; Kinsella et al., 2012; Wald et al., 2009), suggesting foundational commonality across methods. However, seemingly unique to the online methods was increased reports of creativity in problem-solving, the ability to continually monitor one’s own learning through a central focal point, and the ability to iteratively seek help and feedback from peers and supervisors via increased connectivity. Within higher education, students are required to demonstrate core skills in independent thinking, effective communication, responsible action, and continuous professional development (Student Learning Development, 2021). As such, we suggest that using more responsive and intuitive technological methods of reflective practice may support students in SLT and other allied health disciplines to develop these skills, while also enabling them to create an online record of learning and reflection which may serve as the basis of their future professional identity development.
With reference to barriers, both students and educators recommended increased support and training in the use of these online methods, compared to the use of more “traditional” means. We noted in our examination of the details of reflective practice activities and tools used that there was a lack of underlying theoretical frameworks (e.g. Kolb, 1984; Gibbs, 1988; Wareing 2016) referenced within primary studies to explicitly guide the development, production, and assessment of reflective practice. Such established frameworks may have provided the necessary structure and scaffolding requested. It is unclear if students and assessors had access to guiding frameworks or rubrics to scaffold both their writing and marking of these pieces, thus potentially creating uncertainty and a perceived need for additional support and education. It is acknowledged that the use of reflective models facilitates students to develop and demonstrate meta-cognition and meta-reflection, while also providing templates upon which solid rubrics for assessment of these reflections can be constructed (Norrie et al., 2012). Therefore, we suggest that the design of future online reflective practice activities for student SLTs and other allied health disciplines adopts and champions existing reflective models in order to guide all involved through core components of the reflective process, thus potentially overcoming an identified barrier to their use. Enhanced reflective practice skills will lead to enhanced clinical competence of our future colleagues, as they will have developed the ability to work through common challenges as well as solve the unpredictable problems that will no doubt arise in the workplace, which will ultimately result in enhanced client-centred care and a stronger profession (Cook et al., 2019).
Limitations
No research is without limitations, and while this research presents a novel synthesis of the existing literature in this area alongside guidance for HEIs in instructional, pedagogical, and curricular reflection and planning (Kreber & Cranton, 2000), some process and product limitations must be acknowledged. With regards to process limitations, authors excluded non-AHP professionals as this was the focus of the review. In addition, grey literature and records older than five years were excluded to ensure peer-reviewed and contemporaneous literature on recent technology was prioritised. However, the broadening of this criteria could have enriched the findings of the review and provided greater insights into practice in this field. With regards to limitations of the product of this review, it must be acknowledged that study designs were highly heterogenous with mixed quality and that the sample included in the qualitative synthesis was small, with a range of different technologies used, thus limiting generalizability. In addition, SLT and some other AHP professions were not represented in the included studies, thus potentially impacting relevancy and application. As reflective practice has been described as a mechanism for facilitating professional identity development (Bass, Fenwick & Sidebotham, 2017), it is essential that innovative reflective practice is encouraged and emphasized within education and practice to prompt a broader movement towards the development and consolidation of not only individual, but sector-wide, professional identity to meet registration standards and to continue to deliver and enhance the standards of patient care into the future (Bass, Fenwick & Sidebotham, 2017; Caty, Kinsella & Doyle, 2016; Beecham, 2004). Finally, it is worth noting that as the search was completed in November 2020, authors may not have identified all studies reporting the use of technology for reflective practice that was used in response to the COVID-19 pandemic. Therefore, it would be prudent to update this search in future reviews to capture any contemporaneous innovations.
Conclusions and future directions
It is recommended that researchers extend their sampling strategies to include the broad spectrum of AHPs to ensure that all professions are represented. There is a clear need for specific up-to-date SLT research on online reflective practice. In addition, with regards to the practical design of these online tools and the subsequent reflective activities which are facilitated on these platforms, we advise greater integration of theoretical frameworks (e.g. Gibbs’ (1988) or Kolb’s (1984) models) to scaffold student learning and support each step of the reflective practice process. Also advised is early integration of reflective practice into the curriculum, with links to developmental competencies across pre-registration programmes and explicit integration of reflection to standards of proficiency requirements in order to promote early and ongoing development of the reflective practitioner (Schön, 1983). Finally, in relation to the practical design, implementation, and assessment of such online activities, it is advised that the views of both students and practice educators are sought and integrated, to augment the clinical utility of these tasks and to boost their potential real-life impact on reflective practice.
In conclusion, this review suggests that the use of online reflective practice activities supports the development of critical thinking, meta-cognitive, and communication skills, while also embedding reflective practice as an everyday clinical activity, thus supporting the potential growth of SLT and AHP students into modern reflective practitioners (Schön, 1983). Although limitations within the research were identified, a range of enabling and hindering factors to inform the potential use of these online activities were identified. If accounted for, online reflective practice through technological means has the potential to facilitate, support, and augment the use of reflection to enhance the quality of professional education and healthcare delivery, both during the current COVID-related remote teaching period, and indeed, into the future of post-pandemic blended teaching approaches.
Footnotes
Acknowledgments
No funding was secured to support this research.
Conflict of interest
The authors declare no conflicts of interest.