
Abstract
Background and aims
Many undergraduate medical curricula include reflective practice sessions based on traditional Balint-groups. Those sessions can help students to acknowledge that experiencing ‘negative’ feelings in relation to patients is normal and may contain important information about the clinical encounter. They may also help to protect students from some of the emotional challenges of studying medicine. The Edinburgh University scheme provides all students in their first clinical year with two dedicated reflective practice sessions. Here we report on experience of the first two years.
Methods
Students’ attitudes to the sessions were ascertained using a questionnaire, and views of the group leaders were assessed using a questionnaire and through informal verbal and email discussions. Practical difficulties were recorded as they arose.
Results
Students generally rated the sessions positively with regard to exploring relationships and self-reflection, and they found the sessions interesting and helpful. The sessions did not seem to affect career choice. The free-text comments suggested four positive themes and four areas for future modification.
Conclusion
We have succeeded in providing all undergraduate students with an opportunity to take part in a reflective practice. We have highlighted aspects which have been successful and suggested future improvements.
Background
There is a gradual reduction in empathy as medical students progress through their training, 1 with a significant decline during the first clinical year. 2 Various factors have been hypothesised to contribute to this, including: a lack of positive senior role models, 3 experiencing being put down by senior colleagues,4,5an overemphasis on the technological aspects of care in medical education, 6 and the challenge of sustaining empathy as students face emotionally challenging and draining clinical situations.1,7
This decline in empathy is important, as higher empathy in clinicians is associated with better patient satisfaction and collaboration with treatment, 8 lower rate of malpractice litigation 9 and reduced medical errors. 10 A study of 1098 medical students found that lower empathy was associated with higher burnout and reduced wellbeing. 11
In terms of emotionally challenging clinical situations, it is to be expected that medical students and doctors will have a range of feelings in response to clinical situations such as working with patients who have a complicated relationship with care (e.g. patients who reject or criticise offered care).7,12Chronic illness can also be difficult for clinicians to tolerate, as this may conflict with unrealistic personal aspirations and expectations about patients getting better. 13 With regard to challenges to medical students’ identity and sense of self, a recent study by Stubbing et al. 14 of Aberdeen medical students investigated the interaction between students’ preconceptions of being a doctor with their newly developing professional identities in their first year at medical school. They found that early preconceptions about being a doctor, to do with helping and making a difference and ‘to be a leader’, conflicted with the realities they experienced at medical school, creating an emotional tension of ‘being unable to help’ and ‘lacking power’.
It is increasingly recognised that processing and reflecting on the various emotional challenges of clinical work has a key role for clinicians in sustaining empathic patient care and staff wellbeing. The GMC’s Outcomes for Graduates states that students should be able to ‘manage the personal and emotional challenges of coping with work and workload, uncertainty and change’ and ‘develop a range of coping strategies, such as reflection, debriefing, handing over to another colleague, peer support and asking for help, to recover from challenges and set-backs’. 15 Most modern undergraduate curricula incorporate some self-reflection, usually embedded within the general curriculum. Of course, the potential benefits of self-reflection are set in the context of the system the doctor works in, including adequate staffing levels and organisational culture. 16 Notwithstanding these limits, medical educators increasingly recognise that self-reflection should be addressed as a specific learning activity.
The risks of avoiding reflection and the importance of reflecting on clinical encounters
If students believe that having feelings in relation to clinical situations is somehow unprofessional or weak, that can lead them to become anxious when they do experience emotions and to believe they are somehow failing. 17 In Also human: the inner lives of doctors, Elton 18 describes how some doctors develop an unhelpful way of dealing with difficult or painful feelings that arise in clinical work: ‘difficult emotions are pushed out of the conscious mind entirely’ (58). If clinicians avoid reflecting on their emotions, that can contribute to low morale and burnout and can lead to boundary transgressions. 19
By contrast, reflection may help students to work through some of the emotional challenges of studying and practising medicine. When clinicians view (or learn) that having a range of feelings in relation to patients and clinical work is simply part of the work, they may feel able to discuss those feelings with others and thus help protect themselves from burnout. This view is supported by a recent survey of 7584 physicians, which found that clinicians who were better able to describe and identify their feelings to do with clinical work were less prone to emotional exhaustion and experienced more compassion towards patients. 20 Furthermore, if clinicians’ feelings in relation to encounters with patients can become open to reflective discussion within a safe space, there is the potential for clinicians to realise that these feelings may actually contain useful and important information about the interaction itself. 19
One approach to introducing reflective practice is through small-group discussions based on the teaching of Balint. 21 Traditional Balint-groups provide a confidential and supportive setting in which a facilitator helps clinicians to make sense of the dynamics between them and their patients. The clinician is encouraged to reflect upon the feelings arising from clinical encounters and to consider how those emotions might affect their responses to patients.
Balint-groups may improve resilience amongst doctors and protect against burnout and compassion fatigue.22,23Practical benefits include improved therapeutic relationships with some of the most unwell patients, a reduction in counterproductive clinician responses24,25and lower risk of boundary transgressions between patients and staff. 26
Student Balint-groups have been incorporated into undergraduate medical curricula in some European countries, 27 the USA 28 and Australia. 29 Twenty out of the UK’s 34 medical schools offer undergraduate Balint-groups of some sort, and the Royal College of Psychiatrists advocated the introduction of psychotherapy schemes into all medical schools by 2017. 30
O’Neill et al. 29 identified a number of significant challenges in providing student Balint-groups: (i) finding the right place in the curriculum – the first clinical year might be too early because students have insufficient clinical experience; (ii) recognising that because of the short duration of clinical attachments, students generally do not have in-depth knowledge of patients; (iii) acknowledging the tendency for students to revert to problem-solving rather than exploring the emotional components of a case; (iv) ensuring that students clearly understand the purpose of the sessions; (v) identifying suitably qualified group leaders; and (vi) timetabling.
Student Balint schemes have mostly involved self-selected students, which might maximise student engagement but risks just including students who are already comfortable discussing their emotions. Most initiatives have been instigated and delivered by departments of psychiatry or psychotherapy, which ensures expertise in group leaders, but may give the impression that self-reflection is only relevant for students who are interested in psychiatry. It may be more appropriate therefore to situate student Balint-groups in ‘less alienating environments’, such as general practice attachments. 31
The Edinburgh Balint scheme
Our student Balint scheme is run jointly by the departments of psychotherapy and general practice. That collaboration reinforces that self-reflection is important for future medical generalists (i.e. GPs) not just for specialists in mental health. It also maximises tutor availability and facilitates timetabling. Each student attends two sessions during their GP attachment in year 4 (the first clinical year of a six-year curriculum).
In the first two years, half of the groups were facilitated by PW (a psychotherapy trainee), and half by GP-tutors, who were provided with written guidance. In their GP attachment, students were introduced to the Balint approach, and further background was provided in the first session.
Overview of a typical group session
Sessions follow the format of a traditional Balint-group: a participant (the ‘presenter’) describes a clinical encounter; other participants can then ask the presenter to clarify factual aspects; the presenter then sits back, allowing discussion amongst the other participants; and finally the presenter is brought back into the discussion.
Using a combination of observation of reflective practice groups and qualitative accounts from participants, McAvoy 32 describes the course of a typical session from a group perspective as shown in Figure 1.

Stages in the Balint group.
At a group level, there is typically a sequence of:32,33
Starting the group: introductions; setting its purpose, frame and structure; setting key principles, including being non-judgemental and supportive. Finding a topic. The facilitator helps the group decide who will describe a patient encounter, which may include salient clinical situations such as conflicts, distress and perceived threats to competence. The presenter describes the encounter and is encouraged by the facilitator to include feelings that arose for them. Ideas are exchanged, as group members respond to what they have heard. Understanding deepens as the group ‘tries to digest’ aspects of the presenter/patient relationship ‘that could not be seen before’.
34
Differences in opinion might emerge – the facilitator helps the group to make use of disagreements to better understand the interpersonal situation.
Participants typically experience a sequence of attending to the presented topic, reacting to the topic and then, if they feel able, describing this reaction to the group. The views put forward by the group and facilitator often result in participants reflecting upon and re-evaluating their initial response.
Assessing the effect of student Balint-groups
Assessing the effect of student Balint-groups or indeed of any educational intervention on student wellbeing is difficult. Evaluations have used questionnaires, 35 participant observation, 36 leaders’ observations and students’ reflective essays, 31 formal qualitative analysis 28 and randomised controlled trials. 37 A recent systematic review of Balint-groups in undergraduate medical education 38 found just eight studies (four quantitative, one qualitative and three multi-method) which met the authors’ inclusion criteria of ‘relating to undergraduate medical students’ and ‘relating to interventions which had been labelled as Balint-groups’. It concluded that Balint-groups might help medical students to become more patient-centred, increase students’ empathic abilities and support personal and professional growth. To our knowledge, ours is the first study of student Balint-groups in Scotland.
Aim
Our aim was to report a new educational development with an internal evaluation. The evaluation aimed to gain an understanding of the Balint-group experience of students and facilitators and to identify practical issues.
Methods
Balint-style groups (two 1 h sessions in 32 courses) were provided for all 240 year 4 medical students, with 7–8 students per course. Students’ attitudes were ascertained using a simple six-item questionnaire, administered at 16 of the 32 courses (50%) which took place over one academic year. The questionnaire was developed by PW in discussion with AP. It included six closed Likert-scale questions which had a five-point scale from 1 to 5, and space for free-text comments. A higher score indicates a more positive response. It was designed to be brief, to make the evaluation practical and easy to complete within the available time for sessions. The first two questionnaire items pertain to self-reported agreement as to whether two central purposes of Balint-groups were met, namely whether the groups facilitated exploration of the doctor/patient relationship, and whether they allowed for reflection on feelings in relation to patients. 21 Items 3 and 4 pertain to participants’ self-reported interest in the sessions and whether they were felt to be useful, i.e. basic measures of whether the sessions were successful. Item 5 asks whether interest in psychiatry increased as a result of the Balint sessions – this item was included as this is key aim of the Royal College of Psychiatrists Balint-group strategy. 30 Item 6 asked whether interest in general practice increased.
The questionnaire was handed out in the second session and students were invited to complete this. Completed questionnaires were left on a table in the room and subsequently collected by the group facilitator.
The mean score was calculated for each item. HR reviewed all the free-text comments and from this overview formulated themes. These themes were shared with the other authors – the co-authors agreed with the themes chosen. Illustrative quotes from each theme were selected and reported verbatim.
One psychotherapy tutor (PW) and three GP-tutors (HR, ER and HY) delivered the sessions. The GP-tutors were experienced in delivering small-group teaching but were new to reflective practice.
Views of the facilitators were ascertained using a questionnaire and through verbal and email discussions with HR. Practical difficulties were recorded as they arose.
This report is a simple educational evaluation and did not require ethical approval.
Results
Student feedback
Across the 16 Balint courses under evaluation, 81 out of a possible 120 students attended. All of those who attended completed the questionnaire (n = 81). Results are presented in Table 1.
Student questionnaire results.
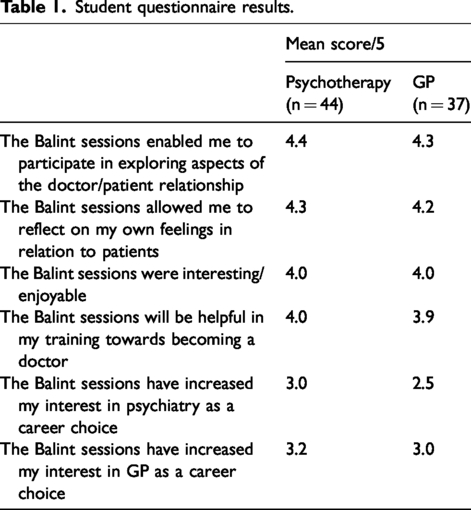
With regard to exploring relationships and self-reflection, the sessions were rated positively. The students found the sessions interesting or enjoyable and helpful. The sessions run by psychotherapy scored slightly higher than the GP sessions. The scheme did not seem to increase interest in either general practice or psychiatry.
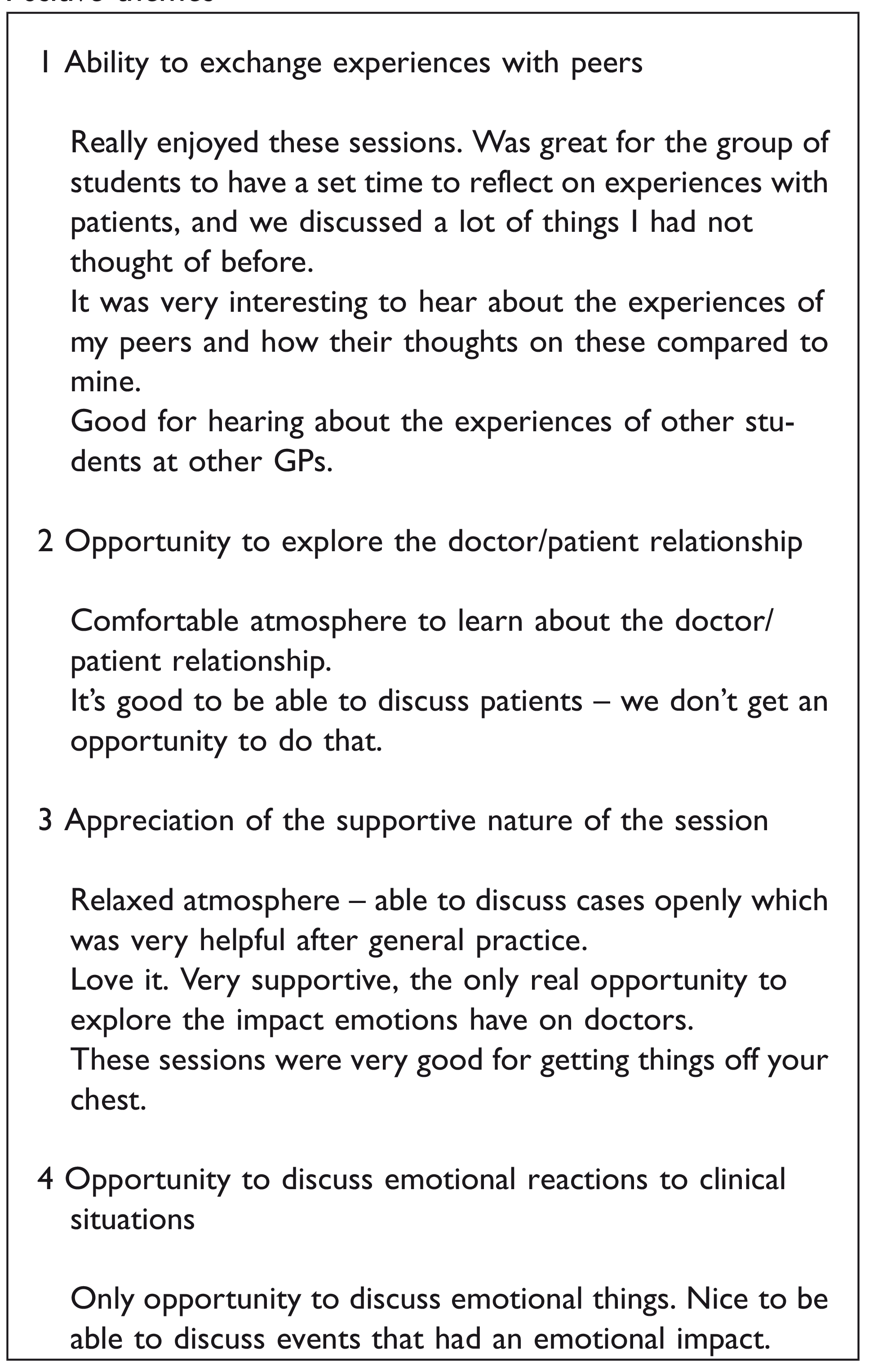
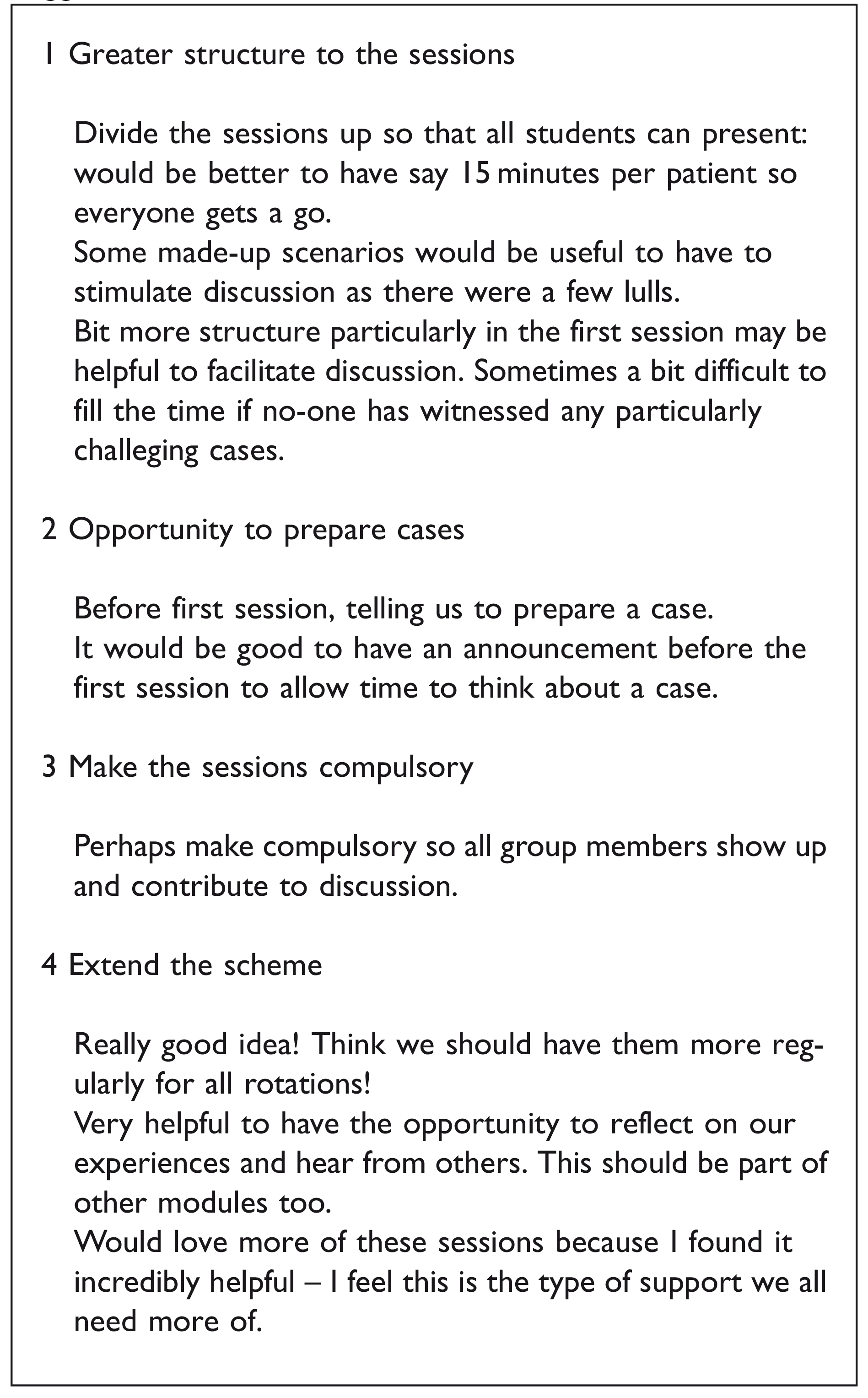
The free-text comments were nearly all positive, although several students expressed initial scepticism: ‘sceptical at first but ended up enjoying the sessions a lot and they got me thinking’. Analysis highlighted four positive themes and four which suggested a need for modifications. The quotes below are all from different students and come from a mixture of the GP-led and psychotherapist-led sessions.
Positive themes
Suggested modifications
Tutor feedback
Three common concerns were identified by GP-tutors: (i) lack of confidence running the groups and a need for more guidance; (ii) lack of clarity about how to deal with silences; and (iii) queries about whether pre-prepared cases should be used. Those concerns were not expressed by PW.
Concerns raised by the GPs were addressed in a training session run by AP who reminded tutors that in several respects, the sessions are different from true Balint-groups, and that expectations must be realistic: first, they are compulsory; second, participants have minimal clinical experience; and third, each student attends just two 1 h sessions. AP also suggested: (i) pre-prepared cases should not be used as this allows responses to be rehearsed, but vignettes can be helpful to stimulate discussion; (ii) students should be reassured that cases do not have to be dramatic; and (iii) students should be steered away from factual content and encouraged to engage in emotional aspects. GP-tutors were also directed to further training with the Balint Society.
Discussion
Our student Balint scheme, running for three years at the time of writing, is unusual in that it involves all students, and it is run collaboratively by the departments of general practice and psychotherapy.
This paper describes the experience of the first two years and includes some basic evaluation. Student feedback was generally positive and highlighted the importance of a safe environment to discuss emotional aspects of cases and doctor/patient interactions. The main concerns raised were lack of structure to the sessions and feeling uneasy about silence.
It soon became evident that whereas the psychotherapy tutor felt confident to run the groups, the GP-tutors did not. They felt uneasy about the sessions’ lack of structure and uncertain about what sort of cases should be discussed. They wondered whether the groups would run better if the scenarios were pre-prepared. Most previously reported student Balint-groups have been led by experienced group leaders and some have involved an accredited Balint leader as well as a co-leader. 31 Inclusion of GP-tutors meant the scheme could cater for all students, and reinforced the important message that the groups are not just for those interested in psychiatry. However, in retrospect, the GP-tutors should have been better prepared.
Limitations
This evaluation would have been strengthened by using standard tools39,40to measure students’ resilience and wellbeing, before and after their Balint sessions. We note that the quality of the free-text evaluation would have been improved by more formal qualitative analysis methods, including analysing whether responses and themes varied according to who led the groups. Finally, we note that risk of bias in outcome evaluation would be lowered by the administration and analysis of questionnaires being carried out by independent researchers who were not those carrying out the intervention. Such work would build on the present educational development and evaluation study and we plan to use these additional measures and improvements in a future research project.
Modification of the Balint method
It has been suggested that student Balint schemes should be modified to take into account students’ lack of clinical experience, their relative immaturity and the fact that they attend fewer sessions than in a traditional Balint scheme. Modifications include allowing discussion of non-clinical issues arising from the students’ educational experience, and allowing group leaders to provide scenarios if volunteers are not forthcoming. Our student and tutor feedback mirrored those observations, and GP-tutor instructions have been modified. Future evaluation of this student Balint scheme is planned, to investigate whether feedback changes following the above modification for groups run by GP-tutors.
Should the sessions be compulsory?
We considered whether the sessions should be compulsory. Traditional Balint-groups are based on voluntary participation, and most student Balint-groups have taken that approach. 38 In our scheme, attendance was initially optional but some students chose to skip the second session, especially in the run-up to examinations. Olds and Malone 36 reported that for two out of their six student sessions, just one of the nine expected students attended, because of ‘medical appointments’ and ‘other teaching commitments’. In our scheme, poor attendance had a negative impact on the students who did attend – some sessions were cancelled because of poor attendance. Poor attendance may suggest that students believe the groups have little educational value or that they are of low priority. After discussion, we decided that the educational value of the sessions justified making them compulsory, in line with practice for first-year Core Trainees in psychiatry.
The embedding of Balint-style sessions into the Edinburgh medical curriculum builds on existing components in the curriculum to do with reflection. Reflective activities are part of the ‘Personal and Professional Development’ theme that runs throughout medical school; topics such as clinician wellbeing and the therapeutic role of the doctor/patient interaction are covered in General Practice modules; and some aspects of the psychological impact of working with patients are covered in psychiatry placements. However, in common with most medical school curricula, we think there is gap for specific teaching about important aspects of reflection captured in this paper, namely interpersonal dynamics, how people (including clinicians) regulate feelings, common emotionally challenging clinical situations and how to process these, common identity challenges for medical students and doctors and how to work these through. Whilst, in some ways, these interpersonal dynamics and aspects of our inner world are less immediately visible than the more technical aspects of medicine, it does not stop these aspects from having a significant effect on both patient care and staff wellbeing. More formal coverage in the curriculum would pave the way for medical students and doctors to access (and provide) reflective spaces such as Balint-groups, and know what they are for and how they work.
Interestingly, in recent years, momentum has grown and a number of Balint-groups and other reflective spaces are now running in medical settings in Edinburgh, such as in Medicine of the Elderly, Accident and Emergency as well as whole hospital reflective practice groups (Schwartz rounds 41 ).
In summary, the Edinburgh University scheme has provided all students with an opportunity to experience student Balint-groups. Student feedback was generally positive and has been used to modify the running of the groups. From this evaluation, we concluded that the scheme should continue to be an integral component of the curriculum. Two areas for improvement were identified: (i) better training and support for GP-tutors by accredited Balint leaders and (ii) better explanation of the purpose of the sessions to the students.
The prevailing climate of a pressured health service, fragmentation of medical care and increasing patient demand means that self-reflection and an ability to manage their own emotions is more important than ever for clinicians. It is hoped that schemes such as ours will help medical students to develop those attributes.
Footnotes
Acknowledgements
We would like to thank the three anonymous reviewers for their detailed and helpful comments which have enhanced the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.