
Abstract
A paramount, yet unresolved issue in personalised medicine is that of automated reasoning with clinical guidelines in multimorbidity settings. This entails enabling machines to use computerised generic clinical guideline recommendations and patient-specific information to yield patient-tailored recommendations where interactions arising due to multimorbidities are resolved. This problem is further complicated by patient management desiderata, in particular the need to account for patient-centric goals as well as preferences of various parties involved. We propose to solve this problem of automated reasoning with interacting guideline recommendations in the context of a given patient by means of computational argumentation. In particular, we advance a structured argumentation formalism ABA+G (short for Assumption-Based Argumentation with Preferences (ABA+) and Goals) for integrating and reasoning with information about recommendations, interactions, patient’s state, preferences and prioritised goals. ABA+G combines assumption-based reasoning with preferences and goal-driven selection among reasoning outcomes. Specifically, we assume defeasible applicability of guideline recommendations with the general goal of patient well-being, resolve interactions (conflicts and otherwise undesirable situations) among recommendations based on the state and preferences of the patient, and employ patient-centered goals to suggest interaction-resolving, goal-importance maximising and preference-adhering recommendations. We use a well-established Transition-based Medical Recommendation model for representing guideline recommendations and identifying interactions thereof, and map the components in question, together with the given patient’s state, prioritised goals, and preferences over actions, to ABA+G for automated reasoning. In this, we follow principles of patient management and establish corresponding theoretical properties as well as illustrate our approach in realistic personalised clinical reasoning scenaria.
Introduction
In the context of medical reasoning, patient management involves careful consideration of the patient’s condition and applicable treatments which should lead to a desired state. Clinical guidelines (such as [44]) are used as the textbook source offering best practice recommendations in general patient management. These documents are by-and-large designed to target single health conditions, leading to issues in the presence of multiple health conditions (multimorbidities). Indeed, in such situations, clinical guidelines should be combined, hence raising the need to consider multiple interactions that impact the evolution of a patient [41,49]. These interactions may render suggested recommendations inapplicable, conflicting, overlapping and so forth. Thus, multimorbidities create obstacles to clinicians in the application of clinical guideline recommendations. In this context, knowledge representation methods from AI may offer mechanisms to ease these obstacles.
Easing the application of clinical guidelines is the objective of the Transition-based Medical Recommendation model (TMR) [108,109], a state-of-the-art formalism [82] for representing computerised clinical guideline recommendations. TMR components and relations reflect knowledge and occurrences typical of multimorbidity situations: the basic components are clinical care actions and their respective effects on the patient’s physical properties; the relations amount to interactions among those actions and their effects. Given the paramount importance of recommendation interactions, TMR provides a mechanism to identify various types of interactions, such as contradiction, repetition and alternative. Therefore, TMR is a comprehensive model for clinical guideline recommendations and situations spawning from their application. However, TMR does not provide reasoning mechanisms to resolve the interactions automatically and thence select recommendations for specific patients.
Reasoning is also limited in several other proposed formalisms for clinical guideline representation, particularly when conflicts come into play [41,75,82]. (A notable exception is the recent CONSULT project [19,20,59,107], which we discuss in Section 7.2.) Additionally, the representations afforded by such formalisms rarely take into account the context of the patient, namely patient-specific conditions, patient-centric goals, and preferences from the various parties involved [75,83,99]. Indeed, integrating all these elements is no easy task. The Ariadne principles [72] attempt to take into account all these elements and provide a conceptual structure for patient management in the context of multimorbidities, stressing the importance of interaction assessment, individual management and patient’s and/or clinician’s goals and preferences. Inspired by these Ariadne principles, in this work we propose a formal framework using a TMR-based and argumentation-enabled approach to reason with interacting clinical guideline recommendations in the context of specific patients, taking into account their state, goals and preferences.
Argumentation is fit for this task as it allows for reasoning with uncertain and conflicting information. Argumentation models reasoning of autonomous agents in multi-agent systems in a way that emulates human reasoning, see e.g. [10,55,74,80]. It has been widely applied to support medical reasoning, see e.g. [29,40,52,63,73,94]. The interest in argumentation from a medical domain perspective is related to the ability of argumentation to allow “for important conflicts to be highlighted and analysed and unimportant conflicts to be suppressed” [6]. We employ structured argumentation (see e.g. [80, Part II] and [11] for overviews) in the form of Assumption-Based Argumentation with Preferences (ABA+) [15,27,33] to automate patient-centric reasoning based on conflicting guideline recommendations, goals, and preferences.
The choice of ABA+ is motivated by several of its characteristics. On the one hand, the nature of knowledge representation and reasoning in ABA+ suits the task of reasoning with interacting clinical guidelines well. Indeed, the rule-based specification of ABA+ frameworks allows for a natural representation of TMR concepts, particularly recommendations, which are essentially of the form “assuming you follow recommendation R, perform action A, which will bring about effect E that affects property P, leading to a change from the initial value
On the other hand, we are strongly driven by practical concerns of deployment of our envisaged argumentation-assisted clinical decision support system. To this end ABA+ is a particularly suitable choice. For one, ABA+ has some known complexity results, first established for the underlying ABA formalism [15] in [34] and recently for its extension with preferences (ABA+) in [60]. Very importantly, ABA+ is equipped with working implementations, for instance the stand-alone1
and web2 applications as described in [7] and a stand-alone development3 built on [56]. These make it easy to implement ABA+G, connect it to TMR (via an implementation4 of [109] and its programming interface TMRweb [20]) and thus lay grounds for the decision support system in question.We use ABA+ to reason with the TMR representations of recommendations and interactions via rules and arguable elements (i.e. assumptions representing applicability of recommendations) from which arguments (as deductions) are constructed. We integrate patient-specific information as well as preferences over actions (effectively, over recommendations) alongside TMR representation in ABA+. We use extension-based semantics for reasoning, thus providing an assumption-driven method by which the applicability of recommendations is argued for or against in light of a patient’s condition. This ensures that all the interactions amongst the suggested recommendations have been resolved. To incorporate treatment goals, we augment ABA+ to form ABA+G by introducing a goal-driven reasoning mechanism to select the best interaction-free (sets of) recommendations based on the importance of patient-centric goals. These knowledge representation, reasoning as well as conflict and preference handling mechanisms used in our approach allow us to meet the Ariadne principles. We illustrate our approach to patient-centric reasoning with interacting recommendations, goals and preferences using a TMR-based case study and show arguably desirable outcomes.
We summarise the main contributions of this paper as follows:
We enable automated reasoning with interacting clinical guidelines represented in the Transition-based Medical Recommendation model (TMR), by mapping recommendations and interactions (of types contradiction, repetition, alternative, and repairable) to a structured-argumentation formalism, ABA+;
We embed patient’s conditions and preferences in ABA+ for assumption-based reasoning with conflicting recommendations and patient-specific information;
We augment ABA+ with prioritised goals for goal-driven patient-centric reasoning with recommendations, to obtain ABA+G;
We establish some theoretical properties of ABA+G, relating them to the Ariadne principles of patient management;
We illustrate the reasoning with a realistic set of guideline recommendations in different patient contexts;
We scrutinise some conceptual and technical choices of our approach and discuss it in relation to argumentative and non-argumentative works in medical reasoning and decision making.
The present work is based on and significantly extends the work in [30] by incorporating additional TMR artefacts, broadening the theoretical exposition of ABA+G and providing an extensive case study illustration. Specifically in terms of TMR, we deal with target values of the properties affected by recommended actions (see Section 3.1.1) and several types of interactions (see Section 3.1.2). As regards ABA+G, we additionally model non-applicability of recommendations and the logic of repairable interactions (see Section 4.3), and slightly generalise the theoretical results regarding the desirable properties of dealing with interacting recommendations (see Section 4.3.3). The case study illustration (see Section 5) is completely new and provides a detailed exemplification of all these aspects.
Currently, an end-to-end proof-of-concept system encompassing electronic health record (EHR) information about patients, TMR via its implementation TMRweb, and ABA+G to provide decision support to clinicians is under development within the ROAD2H project.5
In this paper we provide the theoretical framework for both ABA+G and its implementation6 which is compatible with a wrapper interface that integrates TMRweb, EHR hooks and other relevant functionalities (such as for preference elicitation). The specification of algorithms and other engineering details pertaining to this implementation of ABA+G is beyond the scope of this paper and is left for better suited future publications describing the overall decision support system.We structure this paper as follows. In Section 2 we consider desiderata for our approach in terms of patient management principles from medical literature. We then describe, in Section 3, the problem of reasoning with interacting recommendations in the context of a patient. In Section 4 we propose to use ABA+ and its development ABA+G for assumption-based patient-centric reasoning with recommendations, goals and preferences. We discuss some design choices as well as limitations of our approach in Section 6. In Section 7 we place our work in the context of several related works. We end in Section 8 with conclusions and a summary of future work directions.
In this work we consider the medical reasoning aspect of patient management in a multimorbidity setting. Various works acknowledge several principles of patient management [41,49,75,83,99], but their respective analyses are neither systematic nor provide the necessary level of detail. In contrast, [72] stands out with a comprehensive enumeration and description of patient management principles, therein called
Rather than providing specific methods to handle conflicts stemming from clinical guideline recommendations, the Ariadne principles point out which aspects should be considered in medical reasoning involving multimorbidities and patient context. As for treatment goals, it is stated that information about the effect of treatments on general goals such as increasing life expectancy or quality of life are often unavailable. Instead, restricting treatment goals to tangible effects brought about (or not) by treatments, such as symptom relief, disease prevention, and avoidance of unwanted outcomes, seems to be more effective in this situation. Additionally, the Ariadne principles establish that patient and physician should discuss preferences over actions and priorities over treatment goals, which should be taken into account when devising a treatment plan for the patient.
Reasoning with clinical guidelines in the context of multimorbidities involves aggregation of discordant guideline recommendations and respective interactions. While TMR provides an expressive representation template for this information, it does not enable the above-mentioned aggregation for reasoning to produce patient-specific solutions in a multimorbidity setting. Thus, adhering to the Ariadne principles, even when using TMR for representation, calls for establishing foundations for reasoning in the context of a patient. We answer this call in this paper by situating the TMR model and patient context for reasoning with in ABA+G.
Problem setting
We here describe the problem of reasoning with interacting clinical guideline recommendations in the context of a patient. We first review the TMR model and interactions among recommendations. We then discuss the context of a patient.
Alongside theoretical developments we are concerned with an end-to-end implemented system for reasoning with interacting guideline recommendations. We thus provide details on TMR following [108] but focus on the core features that are already largely implemented and present in [109] and TMRweb, and that will be handled by ABA+G. In what follows we may detail which features of the latest as yet unimplemented theoretical development [108] of TMR we are not making use of (indicated with *).
TMR model
We first give the TMR model together with guideline recommendation interaction representation. They will be used to construct ABA+ frameworks for reasoning with guidelines. (As in [108], we assume that a set of guidelines is merged into a single guideline so that recommendations are delivered by the same larger guideline.)

Figure 1 depicts an instance of a graphical schema for representing recommendations in TMR. (Here, the recommendation concerning NSAID7
Non-steroidal anti-inflammatory drug. NSAIDs are medicines that are widely used to relieve pain, reduce inflammation, and bring down a high temperature, see e.g. www.nhs.uk/conditions/nsaids/.
The original description of recommendations, with components as functions/relations, more suitable for implementation efforts, is long and unnecessary for the purposes of this paper. Instead, we give an intermediate representation which carries the necessary aspects required in this work, following the alternative formal description (and visualisation) in [108] of TMR instances, faithful to the original but omitting certain aspects (as indicated below).
(We write
A unique associated
In practice, indeterminate values do not appear at all, because concrete raw values appearing in the patient’s EHR are processed by a parser to instantiate an ‘intermediate’ patient’s record with the qualitative values as they appear in TMRweb. We will thus henceforth instantiate any indeterminate values with specific qualitative values, without any loss of generality.
In this paper we will not make use of, but mention for completeness, two quantitative values associated with the effect of the contribution: causation probability – e.g. often – representing the likelihood of the action bringing the effect about; and belief strength – e.g. normal level – representing the level of evidence regarding bringing the effect about. We will also not make use of the overall value of the contribution, in the range of
A name R, action A, deontic strength δ, a set of contributions property P affected, effect E on the property, initial value target value
Whenever
We identify any recommendation with its name R and with an abuse of notation may write
Using TMR, one can identify interactions among recommendations [108,109]. Intuitively, interactions record various relationships between different recommendations. In particular:
Contradiction in case a particular recommendation urges avoiding the action suggested by another recommendation.
Repetition in case recommendations suggest taking or avoiding the same action.
Alternative in case recommendations concern different actions having the same or similar consequences.
Repairable in case the consequences of following one recommendation revert the (negative) consequences of following another recommendation.
Interactions and their identification are formally defined in [108,109], but those details are not important for the purposes of this paper. We treat interactions of various types as outputs of (the implementation of) TMR for argumentation to reason with. While several types of interactions can be identified in principle [108], the existing implementation of TMR affords identification of, specifically, Contradiction, Repetition, Alternative and Repairable types of interactions. These are the types of interactions we focus on in this paper and show how they can be naturally resolved by means of argumentation.
Formally, we define:
An
From now on,
The recommendations
Note that a hierarchy of actions is assumed in [108, p. 79] to obtain interactions. For instance, the action to administer NSAID subsumes both actions to administer Aspirin and Ibuprofen. This hierarchy is used when specifying actions in TMRweb, but is not important for our purposes.
When reasoning with interacting clinical guideline recommendations, the goal is to resolve the interactions to be able to follow the recommendations. In particular, Contradiction, Repetition and Alternative interactions are the kind that a clinician aims to avoid having among the recommendations they intend to follow. In other words, no two recommendations R and
The above interpretation of interactions gives rise to the following notions of interaction-free and interaction-resolving sets of recommendations.
Let
Intuitively, interaction-free sets of recommendations consist of recommendations that are safe to follow without the risk of performing a) incompatible (in the case of contradictions), or b) superfluous (in the case of alternatives and repetitions) actions. In addition, interaction-resolving sets of recommendations aim to avoid the risk of performing c) insufficient actions (in the case of repairability). For a recommendation that is repairable, one repair suffices to resolve the interaction, but there may in principle be multiple repairs in an interaction-resolving set of recommendations.
The set
Our representation of recommendations and interactions as afforded by the TMR model will contribute to our approach meeting the 1st and the 3rd Ariadne principles as presented in Section 2.
Recommendations
Consider
The patient information can be understood as the context in which reasoning happens (see e.g. [83]). To resolve the conflict in Example 3.4, one could administer a different NSAID, such as Ibuprofen. However, in more complicated situations such alternatives may not be available. In those situations, preferences may be a part of the context that help to resolve the conflicts argumentatively.
Continuing Example 3.4, suppose that only Aspirin is available. The patient may insist that medication should be given to them, thus preferring taking Aspirin over not taking it, whence only
In general, preference information of various parties often needs to be taken into account to deliver the best care, see e.g. [75,83]. Thus, the context includes not only the patient’s state, but also various preferences. For instance: a) the patient may prefer one course of action over another; b) the clinician may prioritise treatments in accordance with patient-centric goals and their importance. The TMR model however does not afford representation of such preferences, just as it does not afford representation of patient-specific conditions. Thus, when using argumentation frameworks to reason with guidelines in Section 4, patient conditions will come as information additional to TMR instances. One of our tasks is to augment the representation of recommendations and interactions with the context of a patient so as to enable patient-centric reasoning with clinical guidelines. For this purpose, we define the context pertaining to patient information with respect to recommendations as follows.
The the patient’s state the patient-centric goals preferences ⩽ over actions, priorities ≼ over goals.11 Following the terminology of the Ariadne principles, we distinguish between preferences over actions and priorities over goals for ease of reference.
Preferences over actions and priorities over goals can come from various sources, such as the patient, the patient’s family, the clinician or the clinic, and may involve various considerations, such as the cost, availability or quality of evidence regarding actions and importance of goals. For simplicity, in this paper we often ascribe preferences over actions to the patient and priorities over goals to the clinician, without qualifying the underlying considerations. In the rest of the paper we assume that a context is compatible with given recommendations in the following sense: the patient’s state
Continuing from Example 3.5, by concatenating properties with values or effects the context of the patient can be given by
Here
As usual, the strict (asymmetric) counterpart < of a preorder ⩽ is given by
The elements together form a context for the application of recommendations and ground them to a particular setting. The context of a patient will contribute to our approach meeting the 2nd and the 3rd Ariadne principles put forward in Section 2.
We will use guideline recommendations, their interactions and contexts to construct argumentation frameworks for an agent to reason and resolve interactions among recommendations, given patient-specific conditions, patient-centric goals and various preferences. Specifically, we will use ABA+ frameworks, which we review in Section 4.1, for assumption-based reasoning with guidelines and patient’s preferences over recommendations. We will then, in Section 4.2, augment ABA+ to ABA+G for goal-driven reasoning with guidelines and clinician’s priorities over goals. We finally describe and formalise patient-centric reasoning with interacting guideline recommendations in ABA+G, and establish its properties that pave the way to meet the Ariadne principles, in Section 4.3.
ABA+ background
We provide the background for ABA+ following [15,33].
An
⩽ is a preorder (i.e. reflexive and transitive order) on
For
Throughout, we assume a fixed but otherwise arbitrary ABA+ framework
Assumptions in ABA+ represent arguable information. For instance, assumptions can represent the agent’s potential to follow a recommendation. In such a case, preferences in ABA+ can represent the relative (patient’s) willingness to follow different recommendations.
We next give notions of arguments and attacks in ABA+.
An
For
The subscript < on
either there is an argument
or there is an argument
If A does not <-attack B, we may write
We next give notions used to define ABA+ semantics in terms of extensions, i.e. sets of arguments meeting given requirements.
Let A is <-conflict-free iff A <-defends A is <-admissible iff it is closed, <-conflict-free and <-defends itself.
We consider one particular ABA+ semantics, namely <-preferred extensions:
A set
Note that the above effectively defines non-flat ABA+, i.e. generic (non-flat) ABA frameworks with preferences as introduced in [25]. Whenever the preference relation ⩽ on
We extend ABA+ with a mechanism to distinguish among preferred extensions based on goals fulfilled. Goal seeking mechanisms in structured argumentation are introduced in [73] to rank extensions according to the relative priorities over goals fulfilled in the extensions. We import this goal-driven reasoning into ABA+ to define ABA+G, and thus cover the important aspect of reasoning with patient-centric goals.
An ≼ is a total preorder on
In what follows,
In ABA+G, concluding goals amounts to fulfilling them. We hence define (preferred) goal extensions in terms of goal-conclusions thus:
Let E be a <-preferred extension of
In other words, a goal extension consists of the goals in the conclusions of a <-preferred extension. We use priorities over goals to rank goal extensions and define ABA+G semantics:
Let
Note that
Our choice of ordering is motivated by the requirements of a patient management setting, within which priorities over goals may convey a sense of urgency and severity that must be addressed when reasoning. Hence, we assume that an agent should always aim to fulfil the top preferred goals, regardless of the goals with lower priorities. In general, preference aggregation is a rich and complex area of research. Other orderings could be applied, see e.g. [53] for a comparison of various orderings, but we chose the above in accordance with our interpretation of priorities over goals.
We now introduce the representation in ABA+G of TMR instances, interactions and context. We start with an intuitive illustration, then give the formalisation and establish how it meets the Ariadne principles.
Intuition
At a high-level, assumptions will represent (the defeasible potential to follow) recommendations, whereas the corresponding actions and their effects on properties will be modelled via rules, and the deontic strength will determine whether the actions and their consequences are sought after or not, as represented by adding the syntactic
For a step by step illustration, we use recommendations
and interactions
First,
The following rules model the effects the actions
Then, the following rules encode that the specific target values of the properties can be expected (to be avoided) given the effects of the actions and the initial values of the properties:
Now, the additional assumptions
Here,
Arguments against the presumed non-applicability of recommendations will be available whenever the presence of the potentially affected properties can be argued for, allowed by the following rules:
Now,
Dealing with Repetition and Alternative interactions is similar to dealing with Contradiction interactions as suggested above. The intuition is that repetitive or alternative actions are superfluous, and could possibly lead to adverse effects, whence they should not be taken in tandem. That is, recommendations suggesting repetitive or alternative actions will be mutually conflicting in ABA+G. This is in accordance with the desirable reading of interactions as in Section 3 and in [108, p. 91].
Repairable interactions, on the other hand, are more nuanced. Intuitively, following a recommendation
As regards the context
Lastly, as in Example 3.6, goals
Formally, mapping recommendations, interactions and context to ABA+G goes as follows.
Given recommendations Throughout,
rules in
rules in
rules in
Note the symmetry of the rules given an interaction, in accordance with the symmetry of elements of
rules in
The asymmetry of these rules is in accordance with Remark 1. Note also that presence of these rules results into non-flatness of the framework.
⩽ is a preorder over
≼ is either empty or a total preorder over
By convention,
Regarding interactions and rules in
Finally, we define when a recommendation is applicable.
We say that a recommendation
Intuitively, a recommendation is applicable if the patient presents with a state in which the recommendation can affect at least one property. Only applicable recommendations are acceptable in ABA+G, in the sense that no <-preferred extension can contain an inapplicable recommendation, because otherwise it would be <-attacked by the empty set, and hence <-self-attacking.
Given recommendations
Now, if the patient had no preferences, i.e. if
Having formally defined and illustrated a mapping from TMR recommendations, interactions and the context of the patient to ABA+G, we next study some properties of ABA+G patient frameworks.
Modelling recommendations and interactions argumentatively allows to exploit properties of ABA+ to ensure desirable features of our approach. In this section we assume
First, <-preferred extensions in ABA+G patient frameworks are interaction-free (Definition 3.3) as sets of recommendations (recall that we identify a recommendation with its name, see note after Definition 3.1):
(Interaction-freeness ).
For a <-preferred extension E of
Suppose
Thus, top goal extensions (induced by <-preferred extensions) in ABA+G are guaranteed to yield goals achievable without the risk of performing incompatible actions:
For every top goal extension
We argue that this property of ABA+G frameworks is desirable, because it ensures that outcomes of reasoning with guidelines and patient information resolve the interactions arising among the applicable recommendations, as intended by the Ariadne principles.
The second property of ABA+G frameworks states that interaction-resolving sets of recommendations (Definition 3.3) are closed and <-conflict-free in ABA+G:
An interaction-resolving set
Consider
Since
Since closure and <-conflict-freeness are fundamental requirements for any semantics in ABA+, Lemma 4.3 ensures that interaction-resolving recommendations meet the fundamental requirements for acceptance in ABA+G.
Another property states that if the patient expresses preferences over all recommendations, then the most preferred interaction-resolving applicable recommendations (see Definition 4.5) will be followed:
Let ⩽ be a total order over
Let Concerning reverse attacks (see Section 4.1), as recommendations in Concerning normal attacks, suppose for a contradiction that for some First suppose Now suppose Since both E and If Since E is <-preferred, <-defends the closed
So E <-defends
Thus, E <-defends
We thus obtain a contradiction to E being a <-preferred extension. Therefore, by contradiction it holds that
As priorities over goals are used to select among goal extensions induced by <-preferred extensions, top goal extensions (under the same conditions) are obtained by following the most preferred interaction-resolving recommendations:
Let ⩽ be total and
Follows from Theorem 4.4, since top goal extensions are selected among the goal extensions induced by the <-preferred extensions of
We argue that this property of ABA+G frameworks is desirable, because it ensures that the patient’s most preferred recommendations, if applicable, are returned as part of the outcomes of reasoning with guideline recommendations, as intended by the Ariadne principles.
In general, Theorems 4.1 and 4.4, together with Corollaries 4.2 and 4.5, pave the way for ABA+G to meet the three Ariadne principles of interaction assessment, prioritisation and patient preferences and individualised management when applied to patient-centric reasoning with conflicting medical recommendations.
We exemplify the use of ABA+G with a case study from [108], focusing on interactions among Breast Cancer (BC), Osteoarthritis (OA), Hypertension (HT) and Congestive Heart Failure (CHT) guidelines. Graphical representation of the relevant guideline recommendations as well as interactions thereof are depicted in Fig. 2, as taken from [108, Fig. 5, p. 87]. (The underlying details can be found in [108, p. 90, Table 9, p. 91, Table 10].) Our results will accord with the informal discussion on the case study in [108].
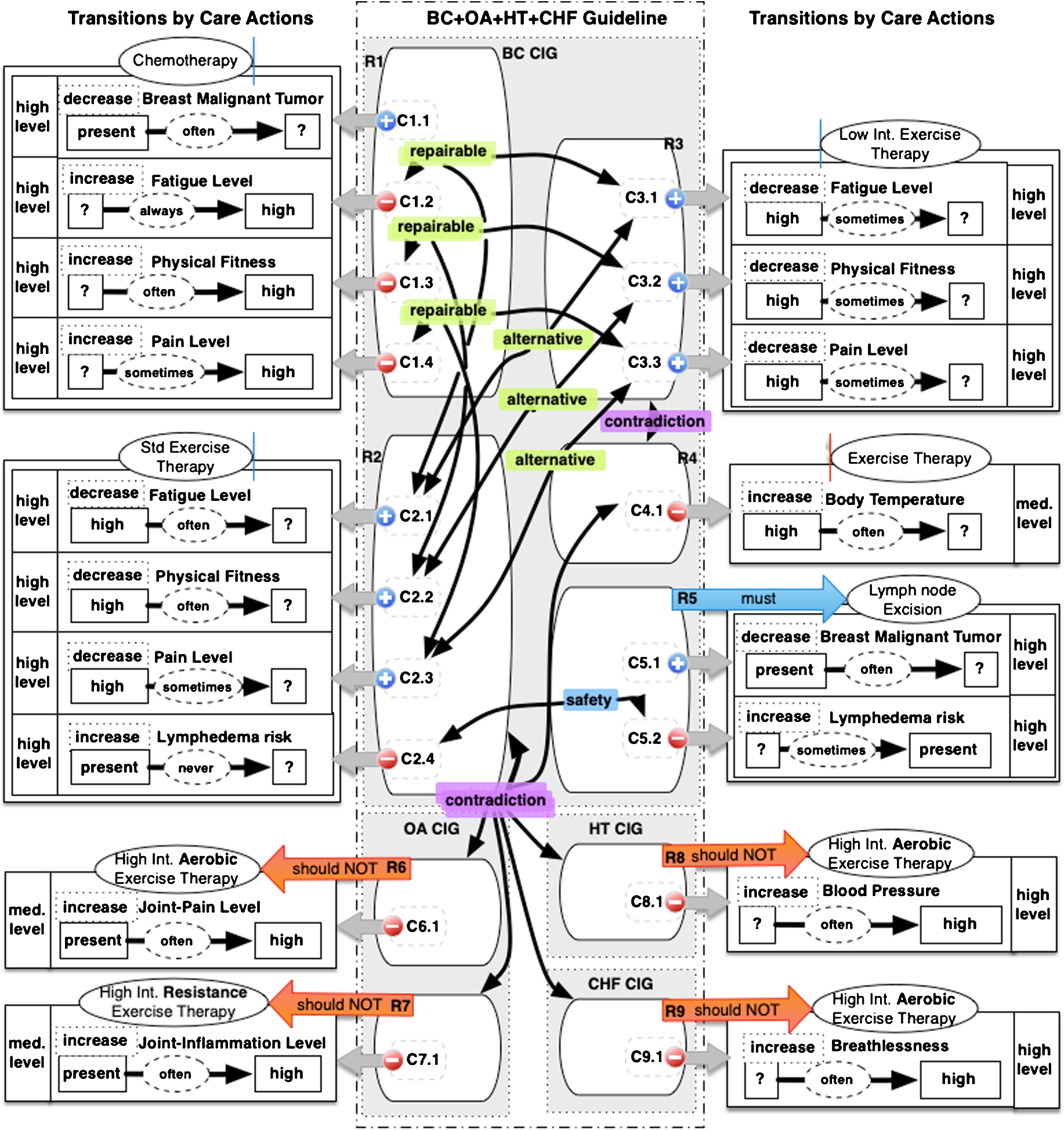
TMR recommendations and interactions in case study for a merged breast cancer, osteoarthritis, hypertension and congestive heart failure guideline [108, p. 87, Fig. 5]. The black arrows indicate which recommendations (or more precisely, contributions) are in an interaction of the specified type. (Figure kindly provided by the authors of [108].)
Dictated by the design choices of ABA+G, we make the following adaptations regarding recommendations and interactions used in this case study.
First, we assume that the deontic strengths of all the recommendations are discretised as Second, as already mentioned in footnote 9, we instantiate all the indeterminate values with values such as Further, as in [108], a hierarchy of actions associated to recommendations is assumed (cf. footnote 10). In particular, the actions concerning various exercises are related in the following way. (a) We omit the word ‘Therapy’ for concision.
Finally, note that contribution
We now spell out the (adapted) recommendations and interactions thereof appearing in this case study.
Let
We then have the following interactions.
Without any information about patients,
Patients and their contexts
We will consider four patients in the following contexts.
We assume all patients to have Breast Cancer present and exhibit fatigue. To illustrate a basic scenario of reasoning with guideline recommendations and interactions, we assume that the first patient has no preferences and also that no explicit goals are set for them:
We assume the second patient to have comorbidity Osteoarthritis and so complain of joint-pain and joint-inflammation. They thus express the preference to not exercise intensely:
Patient 3, in addition to Breast Cancer, has Hypertension and thus suffers from elevated blood pressure. Accordingly, the clinician sets the goals to first and foremost alleviate the breast tumour, followed by not sending the blood pressure even higher, and, if possible, relieving the anticipated fatigue, fitness and pain issues:
visualised below.

The fourth patient is in the same situation as the third one, but also has a preference for low intensity exercise therapy (as per recommendation
We are now ready to construct four ABA+G patient frameworks
We now execute patient-centric reasoning with interacting clinical guideline recommendations in ABA+G.
Patient 1
Consider first
So concerning the remaining applicable recommendations, note first that
Note first that
In the end,
In accordance with Theorem 4.1, both extensions are interaction-free sets of recommendations. The conclusions of either extension indicate (i) the state the patient is already in and the suggested recommendations, (ii) the actions implied by the suggested recommendations, (iii–v) the foreseen consequences of those actions, and (vi–vii) other information pertaining to other available recommendations. In particular, ABA+G suggests that Patient 1 should undergo chemotherapy as well as lymph node excision, accompanied by either standard or low intensity exercise therapies, in order to alleviate Breast Cancer and ease fatigue.
Patient 2
We now consider
Note that
Patient 3
In
In addition to the relevant <-attacks due to interactions as in
The induced goal extensions are as follows.
Note that, in accordance with Corollary 4.2, the goal extensions are induced by interaction-free sets of recommendations.
Now, using priorities over goals we find that
Patient 4
These illustrations show how ABA+G enables reasoning with interacting clinical guideline recommendation in a patient-centric way, whereby the patient’s state and preferences, as well as any goals, set and prioritised by the clinician, are taken into account to provide suggestions as to which recommendations to follow among the many applicable ones. All the <-preferred extensions of each ABA+G patient framework
Discussion
We here discuss some of our design choices concerning ABA+G in this paper. This discussion pertains to some limitations as well as the potential of the integration of TMR, patient context and ABA+G. A discussion regarding the more general properties of the ABA+G formalism as an extension of ABA+ (e.g. in terms of goal orderings and computational complexity) is omitted because it is beyond the scope of this application-targeted paper.
Choices in contrast to [30]
We here discuss two TMR-to-ABA+G mapping differences between this paper and [30].
On Definition 3.2 . Afforded by TMR, one can in principle identify an interaction’s modal strength μ, which reflects the conclusiveness of the interaction, and make use of it when reasoning with interacting recommendations. For instance, following the exposition in [108], one could assume, as in [30], that the interaction’s modal strength can take two values □ and ♢, where □ means ‘the interaction will certainly occur if the related recommendations are prescribed’ and ♢ means ‘the interaction is uncertain to happen’ [108]. In principle then, interactions could also be rendered defeasible in ABA+G so as to allow one to argue about the interactions themselves. However, an interaction’s modal strength depends on a number of parameters, including the knowledge about the hierarchy of actions (see footnote 10), which is not available in the TMR implementation. We are therefore leaving the defeasibility of interactions for future work.
On Section
4.3.1
. In contrast to [30], in Section 4.3.1 we omit an additional condition to rule
Nuances of ABA+G frameworks
Default applicability of recommendations
We have used predicate
Repairable interactions
On Theorem 4.1 and Corollary 4.2 . Regarding the way ABA+G resolves interactions among recommendations by yielding <-preferred extensions that are interaction-free as sets of recommendations, we note that, in principle, Theorem 4.1 and Corollary 4.2 cannot be strengthened to yield interaction-resolving sets of recommendations, as witnessed in the following fictitious example.
Consider recommendations
Consider the set
Nonetheless, in practice, a situation such as in Example 6.1 could hardly arise. Indeed, in case of a Repairable interaction between two recommendations, they would be either both applicable or both inapplicable in ABA+G, because the identification of a Repairable interaction in TMR pertains to finding a property that is inversely affected by the actions of the recommendations. In this setting, we would find the <-preferred extension yielding an interaction-resolving set of recommendations by using the following line of reasoning. If
In any event, our focus was not on unpacking the intricate details of TMR in order to delineate the space of its outcomes. We did not want to couple ABA+G to TMR too tightly either, so as to be able to accommodate possible changes in TMR interaction detection mechanisms (cf. [109] versus [108]). It would nevertheless be interesting to study in the future which restrictions on TMR outputs would allow to strengthen the results from Section 4.3.3.
On Definition
4.4
. Regarding the modelling of Repairable interactions in ABA+G itself, there are other candidate definitions. For instance, one could define
One could also instead define
We lastly discuss briefly our theoretical results concerning preferences over recommendations.
Note that the preference relation over recommendations in Theorem 4.4 and Corollary 4.5 is required to be total. Indeed, with partial preferences the results would not hold in general. This is illustrated in the following example, which is a reformulation of a canonical counter-example [92, Example 4.1] to capturing the so-called preferred sub-theories [17] (in the general case of partially ordered defaults without linearisation of preferences) in structured argumentation.
Consider fictitious recommendations (with some components left unspecified, indicated with ‘?’):
Thus
It would be interesting to investigate other restrictions on preferences over
We stated in the Introduction that the main reasons for using ABA+ in this work are its rule-based nature together with preference-enabled, extension-based reasoning mechanisms as well as the availability of implementations of ABA+. The rule-based formalisation allows ABA+G to naturally model recommendations and their components expressed in TMR. The mechanism of dealing with preferences in ABA+ allows ABA+G to express preferences over recommendations and ensure that interactions among them are resolved. The semantics of <-preferred extensions allows for credulous choices in ABA+G among interacting recommendations. Very importantly, existing complexity analysis [15,34,60] of (versions of) ABA and ABA+ as well as their implementations [7,56] enable rapid development of ABA+G for deployment in an argumentation-assisted DSS.
Predominantly for these reasons, we chose ABA+ instead of some other prominent argumentation formalisms. For instance, Value-Based Argumentation [8,9,54] could potentially be used to reason about different values brought about by following recommendations. However, since TMR lends itself to be naturally formulated using rules and arguably less so using abstract arguments and values, we chose a structured argumentation formalism appropriate for TMR. Carneades [45,47] could also potentially be used in modelling TMR representations via argumentation schemes, yet this would introduce another layer of formalisation and complexity. It also, along with Defeasible Logic Programming (DeLP) [43], employs a sceptical reasoning mechanism, whereas ABA+G instead follows a credulous semantics to allow for choosing among equally legitimate options in the context of contradiction, alternative and repetition interactions among recommendations.
ASPIC+ [67,68,76] is another natural candidate for reasoning with TMR representations, as posited in [29]. One major difference between the use of ASPIC+ and ABA+ could be their treatment of preferences and, specifically in our setting, asymmetric attacks. Indeed, if more nuanced interactions among recommendations were allowed, as is envisaged in the future, then their knowledge representation would entail that the attacks between, say, two recommendations in contradiction, would not be symmetric as it is now in ABA+G, but instead depend on the deducibility of other sentences. As a consequence, reversing (as in ABA+) and deleting (as in ASPIC+) attacks would not result into the same conflict-free sets, and consequently the same desirable outcomes.
In depth analysis is beyond the scope of this paper but it would indeed be interesting to see in the future whether the reasoning as in ABA+G could be enabled by other formalisms, including those discussed above and e.g. Deductive Argumentation [12,13,48] and DefLog [97,98].
We have argued for certain desirable characteristics of our mapping from TMR and patient context into ABA+G, and illustrated that it is applicable in practice. It would nonetheless be interesting to study in the future its possible improvements conceptually and reasoning-wise, especially the currently unaddressed aspects of TMR.
Related work
Argumentation (with or without preferences) has been successfully applied in health care, see e.g. [6,63] for overviews. We discuss several strands of research in this setting with notable examples.
Argumentation for medical reasoning in general
Several works use argumentation semantics for reasoning with medical knowledge and employing preferences. For instance, in [52], manually extracted evidence from randomised clinical trials and systematic reviews is synthesised to form arguments for treatment superiority, with attacks among arguments with conflicting claims. Based on treatment outcome indicators and the importance of evidence, user-specified preferences over arguments and argumentation semantics [35] are used to discard certain attacks, whence semantics of grounded and preferred extensions are used to identify the acceptable arguments. The focus is determining superiority among treatments, not concerning guideline recommendations or conflict resolution among those.
Other works, e.g. [40,78,94], integrate argumentation with preferences to help clinicians to construct, exchange and evaluate arguments for and against decisions. For instance, in [94] argumentation with its semantics as well as preferences are used in multi-agent setting deliberation about organ transplantation. Experts use argumentation schemes [46,102] to construct arguments and attacks concerning viability of transplantation. A mediator agent evaluates the arguments by determining their strength using guideline knowledge as preferences, knowledge about past transplantation as well as about the interacting agents. Similar in spirit is the system ArgMed [78] that allows to document and turn clinicians’ discussions into argumentation frameworks using argumentation schemes, whence preferred semantics is used to find the best claims. On the other hand, to automate medical reasoning, in [40], agents are proposed to exchange arguments structured with claims and backings, and thus arguable against via the latter, but instead of (classical) argumentation semantics various argument weighing and aggregation mechanisms are intended to be used to support decision making. In any event, these works do not concern reasoning with guidelines.
Argumentation for reasoning with clinical guidelines
Argument aggregation for reasoning with guidelines is used in e.g. [50,106]. Specifically, in [50] argumentation schemes are used as templates for generating arguments that correspond to statements in guidelines. In particular, an argument consists of assumptions, claim, polarity (for or against the claim), confidence (e.g. quality of evidence, likelihood of an outcome) and precondition (i.e. whether the argument is applicable). To perform reasoning, a single goal must be specified, whence confidence of arguments is aggregated to identify the acceptable arguments so as to achieve that goal. Similarly, [106] employs a form of argumentation to weigh and aggregate arguments for and against candidate decisions constructed from guidelines towards achieving specified goals. The focus of these works is enacting recommendations from a single guideline, rather than reasoning with interacting recommendations from multiple guidelines.
In terms of reasoning with multiple guidelines in the setting of multimorbidities, the recent CONSULT project [19,20,59,107] applies argumentation to reason with guidelines and patient preferences for managing patients with comorbidities. Specifically, they use structured metalevel argumentation frameworks (MAFs) based on either, essentially, second-order logic as in [107], or first-order logic as in [59], to construct arguments using argumentation schemes and particularly the critical questions pertaining to the latter. Their newly introduced argumentation schemes with their critical questions serve as templates for structuring arguments about statements manually extracted from clinical guidelines. They further integrate preferences modelled as attacks on attacks, following [65], into MAFs to resolve conflicts among arguments. What is more, they also consider conflicts among guideline recommendations by means of TMR as an external service to the argumentation engine [19]. Importantly, the CONSULT project has developed and uses TMRweb. We likewise rely on TMRweb in our implementation efforts, but in our theoretical foundations instead use the TMR model to represent guideline recommendations and identify their interactions, which we then together with patient information map directly into ABA+G frameworks (using effectively a fragment of Horn logic contrasting greatly complexity-wise with first- and second-order logics). We also incorporate preference information directly in the construction of attacks when resolving interactions. In addition, we allow for reasoning with prioritised goals in ABA+G. Importantly, our approach enables us to meet the Ariadne principles of patient management.
Non-argumentative approaches to medical decision making
Non-argumentative approaches to reasoning with clinical guidelines exist too, see [75,82] for overviews. A recent work concerning reasoning with interacting guidelines, patient conditions and preferences represents guideline recommendations as actionable graphs [105], mapping them into first-order logic (FOL) rules, while representing patient conditions and preferences as FOL revision operators. Then, reasoning (guideline mitigation) amounts to applying revision operators to account for patient-specific conditions and preferences, and then finding models of the resulting FOL theory. Our approach is different in both knowledge representation – the TMR model is richer than the mitigation-specific FOL, and computation mechanism – model finding is undecidable as opposed to finding preferred extensions. We also believe argumentation-based reasoning to be more transparent, as one can inspect the arguments, attacks among them and their interplay with preferences, in contrast to interpreting workings and results of a FOL theorem prover.
Other approaches to reasoning with guidelines focus on execution of single guidelines, e.g. [61,89], or identification of incompatibilities among guidelines. As to the latter, answer set programming is for instance used in [91] to check temporal conformance through a posteriori verification of a single guideline with the recommendations actually followed, motivated by the patient state. On the other hand, statistical preference learning is used in [96] to identify inconsistencies in antibiotic therapy guidelines. The objectives of these works are thus different from the objective of the work herein.
Yet other works concern preference elicitation to facilitate clinical decision making. In particular, in [83] the authors incorporate patients’ preferences in terms of QALY (quality-adjusted life-year), utilities and costs into the shared decision making model. In effect, they propose a framework that supports patient preference elicitation and integrates them with patient health record to feed into decision models (particularly, decision trees) so as to facilitate shared (clinician-patient) decision making. This allows to better inform both the clinician and the patient about the alternatives, but does not afford automatic resolution of interacting (e.g. conflicting) recommendations. It would be interesting nonetheless to see how this line of work could inform knowledge representation in our approach.
Goal-driven argumentative decision making
Goal-driven argumentative decision making (possibly with preferences) has been explored, see e.g. [2,36,71,110]. For instance, the approach of [2] concerns general multiple criteria decision making in argumentation with preferences via reasoning backwards from goals to arguments. A follow-up application-specific approach (see [71]) affords goal-driven argumentative documentation, analysis and making of decisions. On the one hand, the settings there do not apply to reasoning with guidelines. On the other hand, ABA+G differs from these approaches in at least two other aspects. First, in terms of using preferences (over goals) to select among extensions, as in e.g. [4,100]. Second, in terms of the direction of reasoning – from arguments to goals, which is more similar to assumption-based reasoning with goals and preferences as in [36], which we discuss in more detail below.
In [36] ABA frameworks without preferences are used for contract negotiation. The frameworks are however equipped with goals and preferences among them. Therein, a goal corresponds to the conclusion of a rule and preferences over goals follow a total preorder. These ideas are also adopted in our work, along with the reasoning principle of pursuing higher-ranked goals at the expense of lower-ranked goals. Thus, comparing solutions in the form of <-preferred extensions amounts to comparing goal states in [36], which correspond to goal extensions in our work. The approaches are however slightly different in details. For comparison, we reproduce here their definition of an ordering of goal states: For G and there exists a goal g that is satisfied in G but not in for each goal
where P is a ranking function mapping goals to natural numbers.
Now, for contrast, let G and
In [36], the authors further elaborate on goal states by proposing minimal goal states from a set of states promoted by a decision. Therein, a decision is an accepted assumption and all assumptions representing decisions are mutually exclusive. The possible minimal states stemming from decisions are used to characterise single assumptions and establish preferences among them. In ABA+G instead, assumptions representing recommendations are not generally mutually exclusive, with preferences among them used for establishing acceptable recommendations and goals thereof. Overall thus, the objectives of our work and that of [36] are rather different. It would nonetheless be interesting to investigate the formal relationships with this work in the future.
In relation to argumentative decision making, we also mention the general approach of [2], where several principles for the comparison of decisions are established. The aims of that work and ours are significantly different, however. The authors of [2] analyse abstract argumentation for the purpose of general decision-making and use pre-established candidate decisions within the argumentative reasoning. Differently, here we deploy structured argumentation in the form of ABA+ and augment it with goals to accommodate the TMR model and meet the Ariadne principles for a domain-specific application, whereby decisions are formed after the argumentative reasoning with extension-based semantics.
We lastly note that an argumentative approach to explainable decision making with contextual goals was recently proposed and illustrated with a medical decision making example in [110]. There, context rules and primitives involving patient state properties are used to assert defeasibility of logical implications between decisions, attributes, and goals. While the approach focuses on explainability issues in decision making and is thus not directly related to this paper, it shows that context-sensitivity is an important and desirable property in both medical and argumentative settings, that we specifically addressed in this work.
Conclusions and future work
We have shown how ABA+G, a structured-argumentation formalism proposed in [30] and extending the ABA+ [15,27,33] formalism with prioritised goals, can be used to automate patient-centric reasoning with interacting clinical guideline recommendations. Specifically, we mapped Transition-based Medical Recommendation (TMR) [108,109] representations of guideline recommendations to ABA+, incorporated in ABA+ patient-specific conditions and their preferences, and augmented ABA+ to ABA+G so as to deal with patient-centric goals and priorities among them. We showed, among other properties, that ABA+G yields interaction-free sets of recommendations taking into account the context of the patient in terms of their state, preferences (over recommendation actions), and prioritised achievable goals. We illustrated our approach to patient-centric reasoning with interacting guideline recommendations by using a TMR-based use case, complementing it with various patients and their contexts. We posited that our approach meets the set-out Ariadne principles [72] of patient management, thus establishing a unique relationship between features of argumentative reasoning and personalised care in multimorbidity settings.
The most important milestone in the future is carrying out an evaluation of ABA+G as well as integrating it within an overall decision support system (DSS) assisting with decision making in multimorbidity settings, for instance as envisaged within the ROAD2H project21
in real clinical settings. A crucial aspect of such an evaluation will be the explainability of the overall system. Argumentation is indeed well-suited for explainable reasoning [6,40,70] with argumentative explanations proposed in various settings, see e.g. [1–3,5,14,16,18,21–24,26,28,31,32,37–39,42,43,51,57,58,62,64,66,69,70,77,79,81,84–88,90,93,101,103,104,110–112]. We hope to exploit the well-established as well as novel ABA+ mechanisms to our advantage of providing various explanations to accompany the decisions supported by ABA+G. In addition to several other future work directions mentioned in Sections 6 and 7, we will aim to extend ABA+G to take into account various TMR artefacts not yet present in ABA+G. This may yield additional preferences and result in a probabilistic extension of ABA+G, requiring further study.Footnotes
Acknowledgements
The authors are grateful to colleagues in the ROAD2H project for many fruitful conversations, particularly to Dr Jesús Domínguez, Dr Martin Chapman and Dr Vasa Curcin regarding TMRweb and the development of a DSS, as well as to Denys Prociuk and Prof Brendan Delaney, MD regarding the clinical input to this work. We also thank other medical experts for their helpful feedback. We are extremely grateful to Veruska Carretta Zamborlini, Annette Ten Teije and other co-authors of [![]() ] for permitting to use and supplying us with the figures from their paper to be used herein. Finally, we thank the anonymous reviewers of this article for their helpful feedback too.
] for permitting to use and supplying us with the figures from their paper to be used herein. Finally, we thank the anonymous reviewers of this article for their helpful feedback too.
Kristijonas Čyras, Amin Karamlou and Francesca Toni were supported by EPSRC Grant
Tiago Oliveira was supported by JSPS KAKENHI Grant Number
Data access statement
No new data was collected in the course of this research.