
Abstract
Historically, the concept of childhood mental illness as distinct from that in adults did not arise until the early part of the 20th century [1]. The first English language text on child psychiatry was published in 1935 [2], but research into treatment of childhood mental illness did not begin until the latter part of the century. During the 1980s researchers began to assemble information on childhood mental problems from various treatment sources such as schools, children's social services and the medical profession [3–5].
In 2003 in Australia, mental disorders (particularly anxiety and depression) were the leading cause of burden of disease and injury for 15–24 year olds [6]. The most recent detailed information on the mental health of children aged less than 18 years in Australia is the 1998 National Survey of Mental Health and Wellbeing. Results showed that 14% of children aged 4–17 years had mental health problems [7], and of these, only a quarter had attended a professional service (such as a clinician or school counsellor) for emotional and behavioural problems in the previous six months [8]. Seven years later, a study of Canadian children produced very similar estimates [9]. In the USA in 2003, 9.2% of children aged 3–17 years were reported to have moderate or severe difficulties in the area of emotions, concentration, behaviour or getting along with others [10]. Again the literature suggests that the proportion of children who actually attend a general practitioner (GP) for mental problems is far lower: an international review of frequency of child and adolescent psychiatric disorders among children who attend primary care clinics found that some 2–5% of children present with psychological problems, [11] and in the Netherlands about 7% of children and adolescents who had visited their GP received a psychological diagnosis [12].
There has been rising concern over the extent of mental health problems in children in recent years. In Sweden between 1988 and 2005 psychosomatic health deteriorated among 15–16 year olds, particularly among girls [13]. Similarly, in Scotland the incidence of self-reported psychological distress increased significantly for 15 year old girls between 1987 and 1999 [14], while in the USA the rate of 5–14 year old children's hospitalizations for mental illness rose 22% during the 1990s and mental illness surpassed injury as the leading cause of hospitalization among children and adolescents [15]. A related area of concern was highlighted in an Australian study which found an increase of 87% in stimulant dispensing between 2002 and 2009, with dexamphetamine and methylphenidate most commonly dispensed to patients aged 10–14 years [16].
In general practice in Australia, the management rate of psychological problems for patients of all ages rose significantly from 10.3 per 100 encounters (95%CI = 9.8–10.8) in 2002–2003 to 11.5 (95%CI = 10.9–12.0) in 2007–2008 [17]. This coincided with increased government funding through Medicare (the national healthcare system) for GP mental health treatment as part of the 2006 initiative, Better Access to Psychiatrists, Psychologists and General Practitioners, allowing GPs to refer selected patients to psychologists for subsidized services [18]. One of the objectives of this paper was to determine whether there was a similar trend in GP management rates of mental problems in children.
In a previous publication we reported that GP management rates of a number of ‘traditional’ childhood illnesses such as otitis media, asthma, tonsillitis, acute bronchitis, and gastroenteritis decreased significantly between 1990–1991 and 2001, and a descriptive comparison with a similar study conducted from 1969–1974 suggested this trend had been apparent since 1970–1971 [19]. However, the rate and management of psychological problems in children in Australian general practice has not been examined. The current study aims to fill this gap in the literature by examining changes over the last four decades in children's mental health problems managed in general practice, and to describe recent management of these problems.
Method
The BEACH (Bettering the Evaluation and Care of Health) programme is a continuous, national, cross-sectional study of general practice activity in Australia, which began in April 1998. The methods are described in detail elsewhere [20]. In brief, an ever-changing random sample of recognized GPs drawn from Australian Government GP Medicare claims records is invited to participate throughout each study year which runs from April–March. About 1000 GPs, approximately 80% of those who agree to take part, complete the study annually. Each GP records details on structured paper forms for 100 consecutive encounters with consenting patients, including surgery, home or hospital visits, and indirect encounters (patient not seen) where a clinical action is taken.
Morbidity managed was classified according to the International Classification of Primary Care Version 2 (ICPC-2) [21], and coded more specifically in an Australian general practice interface terminology, ICPC-2 Plus [22]. ‘All psychological problems’ are those problems classified in the psychological chapter of ICPC-2. Single ICPC-2 rubrics defined sleep disturbance, suicide, attention deficit hyperactivity disorder (ADHD), post-traumatic stress disorder, anorexia nervosa/bulimia, enuresis and encopresis. Grouped rubrics and terms are defined in Box 1.
Box 1. ICPC-2 rubrics and ICPC-2 Plus terms included in grouped psychological problems.
Anxiety: feeling anxious, stress, adjustment disorder and phobias (ICPC-2 codes P01, P02, P74, P79, and ICPC-2 Plus codes P22007, P29003, P29024, P29006).
Depression: feeling depressed, depressive disorder and affective psychosis (ICPC-2 codes P03, P76, P73).
Substance abuse: alcohol, tobacco, medications and illicit drugs (ICPC-2 codes P15, P16, P17, P18, P19).
Intellectual impairment: delayed development, learning difficulties and intellectual disability. (ICPC-2 codes P24, P28, P85, and ICPC-2 Plus codes P22012, P22013, P22014, P22015, P22016)
Behaviour disorders: eating disorders, emotional disturbance, defiance, tantrums and personality disorders. (ICPC-2 codes P11, P23, P80 and ICPC-2 Plus codes P22001, P22002, P22004, P22005, P22008, P22009, P22010, P22011, P22018, P29001, P29023, P29029)
Autism spectrum disorders: autism and Asperger's syndrome. (ICPC-2 Plus codes P99005, P29006, P29010)
Medications were classified according to the Anatomical Therapeutic Chemical (ATC) index [23]. All psychotropic medications (defined as ATC groups N05 and N06) recorded at consultations with children were included.
Data from 2000–2001 and 2008–2009 of the national BEACH programme are compared with data from the year-long national Australian Morbidity and Treatment Survey 1990–1991 (AMTS) [24] on which two of the authors of this paper were researchers. Differences are regarded as significant by non-overlapping 95% confidence intervals. Descriptive comparisons with the second year of a 1969–1974 study utilize previously published data in which confidence intervals were not provided [25].
Data sources
In the 1970–1971 year of the Australian General Practice Morbidity and Prescribing Survey 1969–1974, 769 volunteer GPs each recorded details of surgery consultations and home visits for one week. Morbidity data were classified by the clinicians according to 200 codes selected from ICD-8 [26]. Prescribing data for children were not reported.
A sub-sample of 24 237 encounters from 769 GPs with children aged 0–14 years.
In the AMTS 1990–1991, a random sample of 495 GPs each recorded details of surgery and home encounters for two periods of 1 week, 6 months apart. Problems managed were classified according to ICPC (Version 1)[27] and medications were classified according to an in-house system that is compatible with the ATC index.
A sub-sample of 17 830 encounters from 470 GPs with children aged 0–14 years (for comparison with 1970–1971).
A sub-sample of 20 630 encounters from 471 GPs with children aged 0–17 years (for comparison with BEACH).
In BEACH, January 2000 to December 2001, a random sample of 1931 GPs recorded details of 191 762 patient encounters (at all locations).
A sub-sample of encounters with children aged 0–14 years: 24 616 consultations from 1892 GPs.
A sub-sample of encounters with children aged 0–17 years: 28 907 consultations from 1911 GPs.
In BEACH, January 2008 to December 2009, a random sample of 2054 GPs recorded details of 204 425 patient encounters (at all locations).
A sub-sample of encounters with children aged 0–14 years: 23 384 consultations from 2010 GPs.
A sub-sample of encounters with children aged 0–17 years: 27 399 consultations from 2030 GPs.
In order to achieve comparability when comparing results with both earlier surveys, the more extensive BEACH data set was reduced to surgery and home visits by excluding indirect encounters and hospital consultations. Likewise, in comparisons with the 1971 published results, the age group analysed in BEACH and the AMTS was restricted to children aged less than 15 years, and problems managed shown as percentages of all problems or of all psychological problems managed. The comparison between the two later studies used an existing map between ICPC Version 1 (AMTS) and the more detailed ICPC-2 (BEACH), and this was adequate for most problems recorded. Autism was an exception because it was part of a wider ICPC-1 rubric ‘Other unspecified psychosis’ in the AMTS, but was defined by separate ICPC-2 Plus terms in BEACH.
Data recorded in BEACH between January 2008 and December 2009 were used in the analysis of current practice for total psychological problems and specifically for depression, anxiety and ADHD. As no comparisons were being made with other studies, all encounters were included and, in line with a number of recent international studies, the age group analysed was children aged less than 18 years. Analysis of medications was based on all psychotropic medications recorded for children of this age, irrespective of indication recorded.
The AMTS and BEACH studies used national random samples of Australian GPs, each providing data about a cluster of encounters. Robust 95% confidence intervals which account for the cluster sample design are reported around the point estimates, using procedures in SAS software [28].
The BEACH study is approved by the Ethics Committee of the University of Sydney.
Results
Changes over time 1971–2009
In 1971, 2% of all problems managed for children aged less than 15 years were of a psychological nature. The proportion dropped to 1.3% in 1990–1991 and showed a similar level in 2000–2001 (1.4%; 95%CI = 1.3–1.6). In 2008–2009, the proportion significantly increased to 2.6% (95%CI = 2.3–2.9) of all problems (results not tabled).
Enuresis of non-organic origin accounted for 30% of children's psychological problems in 1971 but enuresis/encopresis accounted for only 2.7% in 2008–2009. Insomnia, which represented 20% of children's mental problems in 1971, was compared with all sleep disturbances (including nightmares and sleepiness) in the later studies, and accounted for only 10.8% in 1990–1991 and 11.8% in 2008–2009. In 1971 and 1990–1991, behavioural problems accounted for about one in five psychological problems managed in children, but this had decreased to 11.6% by 2008–2009. However, while ‘behavioural problems’ decreased between 1990–1991 and 2008–2009, the proportion of psychological problems that were ADHD increased from 0.8% to 14.7% over the same period. Anxiety, as a proportion of all problems, increased from 11.9% in 1971 to 18.4% in 2008–2009, and depression increased from 1.4% of psychological problems managed in 1971 to a high of 9.8% in 2000–2001. Intellectual impairment was not reported among the common problems managed in 1971, but accounted for one in ten psychological problems managed at child encounters in 1991 and one in six in 2008–2009. There was no specific code for autism in the coding frame used in 1971, nor in 1990–1991 when there were only three cases of ‘other unspecified psychosis’. Between 2000–2001 and 2008–2009, autism spectrum disorders rose from 4.9% to 11% of children's psychological problems (Figure 1).
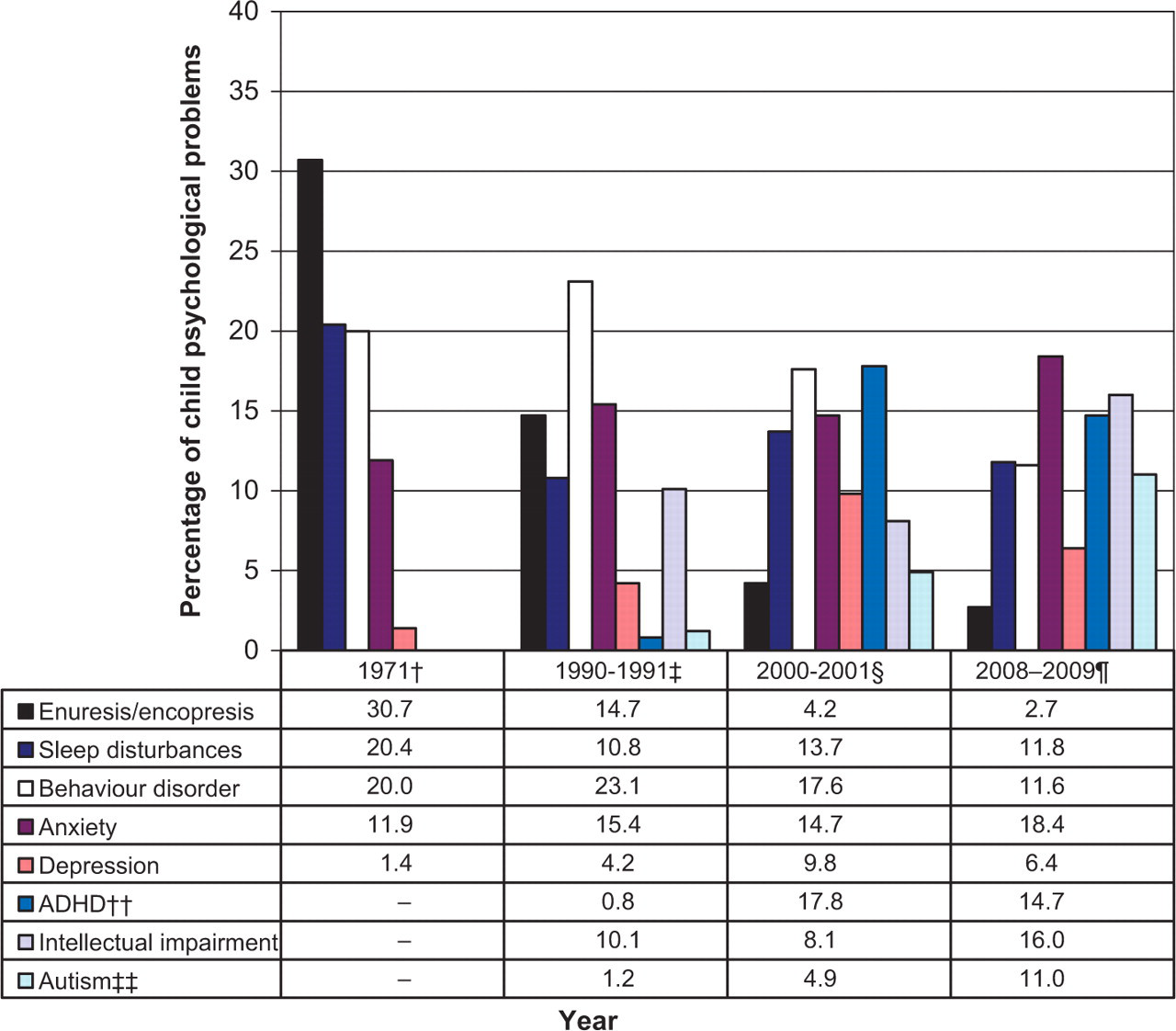
Individual psychological problems managed for children aged. †AGPMPS 1971; ‡AMTS 1990–1991; §BEACH 2000–2001 calendar years; BEACH 2008–2009 calendar years. ††Attention deficit (hyperactivity) disorder, or hyperkinetic disorder. ‡‡In AMTS the ICPC label was ‘Other unspecified psychosis’; in BEACH the ICPC-2 Plus terms autism, autism child, and Asperger's syndrome were selected. ‘–’ not reported among common problems.
Between 1990–1991 and 2000–2001, there was a significant increase in the management rate of psychological problems at encounters with children aged less than 18 years, from 14.4 to 23.8 per 1000 child encounters. By 2008–2009, this had again increased significantly to 39.0 per 1000 child encounters. Between 1990–1991 and 2000–2001 the rate of all medications recorded per 100 children's psychological problems increased from 14.2 to a peak of 28.8 then dropped to 18.3 in 2008–2009. Psychotropic medications followed a similar pattern. Other treatment rates were steady in 1990–91 and 2000–2001 then decreased significantly in 2008–2009. The decrease in medication and other treatment rates coincided with a significant increase in the rate of referrals (Figure 2).
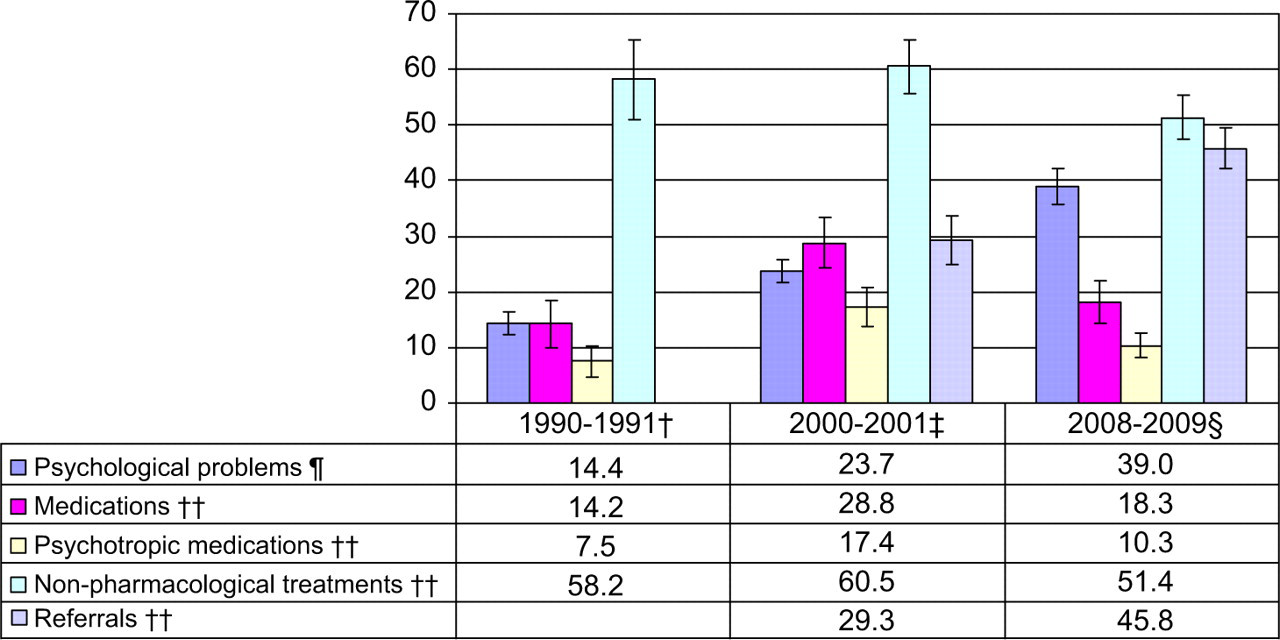
Psychological problems and their management for children aged less than 18 years. †AMTS 1990–1991; ‡BEACH 2000 and 2001 calendar years; §BEACH 2008 and 2009 calendar years. ¶Psychological problems managed per 1,000 encounters with children aged less than 18 years. ††All medications, psychotropic medications, other treatments and referrals per 100 psychological problems managed in children aged less than 18 years. 1990–1991 data did not allow for the linking of referrals to problems being managed.
Current practice
There were 27 399 encounters (including hospital and indirect consultations) with children aged less than 18 years recorded in BEACH between January 2008 and December 2009, and psychological problems were managed 1083 times, at a rate of 40 per 1000 children's encounters. The management rate rose significantly through age groups, from 17 per 1000 encounters with children aged 0–5 years to 52 per 1000 with 6–11 year olds and 73 per 1000 with children aged 12–17 years. Among children aged 0–5 years, sleep disturbance and intellectual impairment (mostly delayed development) were the main problems, while among 6–11 year olds anxiety and ADHD were most common. Depression was the most frequently managed problem for those aged 12–17 years (Table 1).
Management rates of psychological problems in children, 2008–2009.
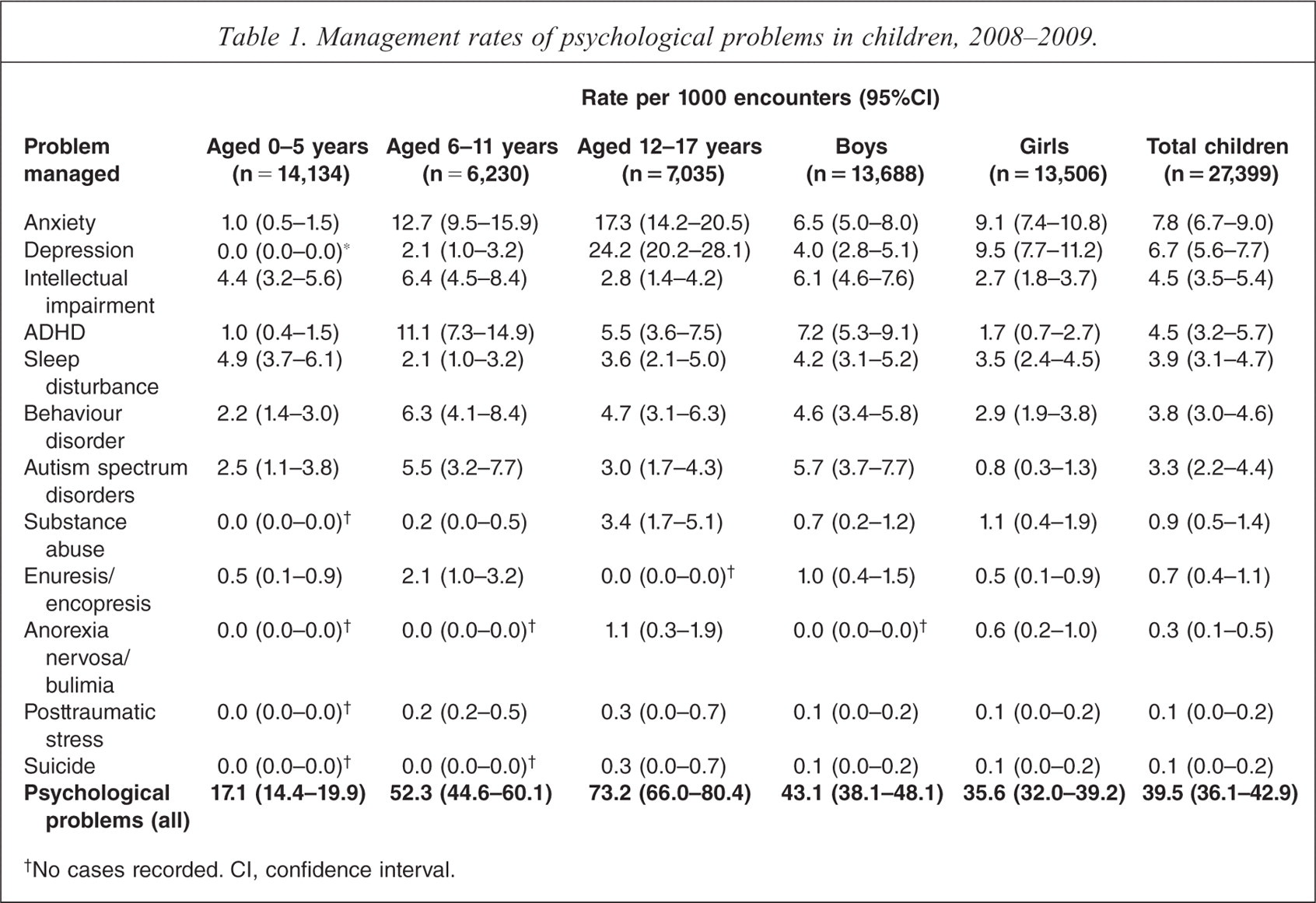
No cases recorded. CI, confidence interval.
Sex-specific analysis showed that boys were significantly more likely to be managed for intellectual impairment (6.1 per 1000 encounters) than were girls (2.7 per 1000). Boys also had significantly higher management rates of ADHD (7.2 compared with 1.7), while autism spectrum disorders were managed at a rate of 5.7 for boys and 0.8 for girls. On the other hand, girls were significantly more likely to be managed for depression (9.5 per 1000 encounters) than were boys (4.0 per 1000). Overall, the most common psychological problems managed for children under 18 years of age were anxiety, depression, intellectual impairment and ADHD (Table 1).
Depression, anxiety, ADHD and total psychological problems
At encounters where depression was managed, seven out of ten children were girls, while four out of five children managed for ADHD were boys. Anxiety, in particular, and depression were commonly managed under a GP Mental Health Treatment Medicare item, [18] whereas ADHD was not (Table 2). Anxiety was significantly more likely than depression and ADHD to be managed as a new problem for the patient, whereas over 80% of ADHD was recorded as ongoing management by the GP.
Depression, anxiety, ADHD and all psychological problems at encounters with children, 2008–2009.
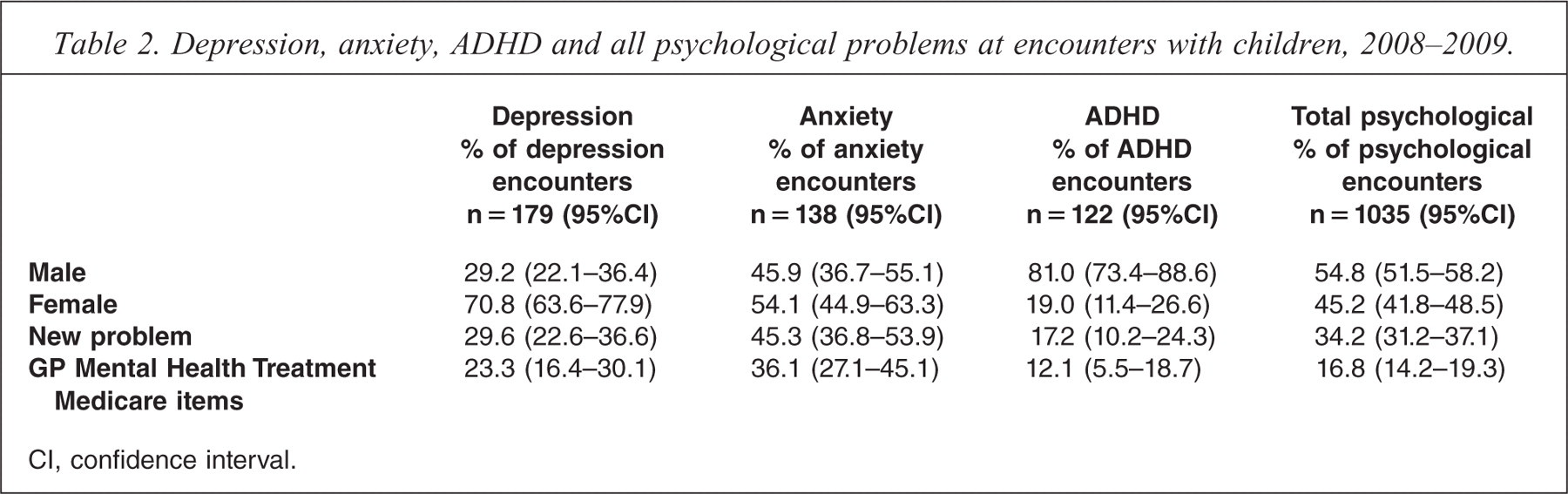
CI, confidence interval.
The overall rate of medications prescribed, supplied or advised was low at 18.8 per 100 psychological problems in children, although the medication rates for depression and ADHD were much higher at about 40 and 30 per 100 problems respectively (Table 3). For depression, selective serotonin reuptake inhibitors were most commonly prescribed, while for ADHD psychostimulants were most common. Other treatments consisted mainly of counselling, and were provided at a high rate, except in the management of ADHD where counselling was provided far less frequently. Referrals were provided for children at the very high rate of 44.4 per 100 total psychological problems managed. Of these referrals, 36.8% were to psychologists, 27.7% to paediatricians, 6.4% to psychiatrists and 6.2% to speech therapists.
Management of depression, anxiety, ADHD and all psychological problems at encounters with children, 2008–2009.
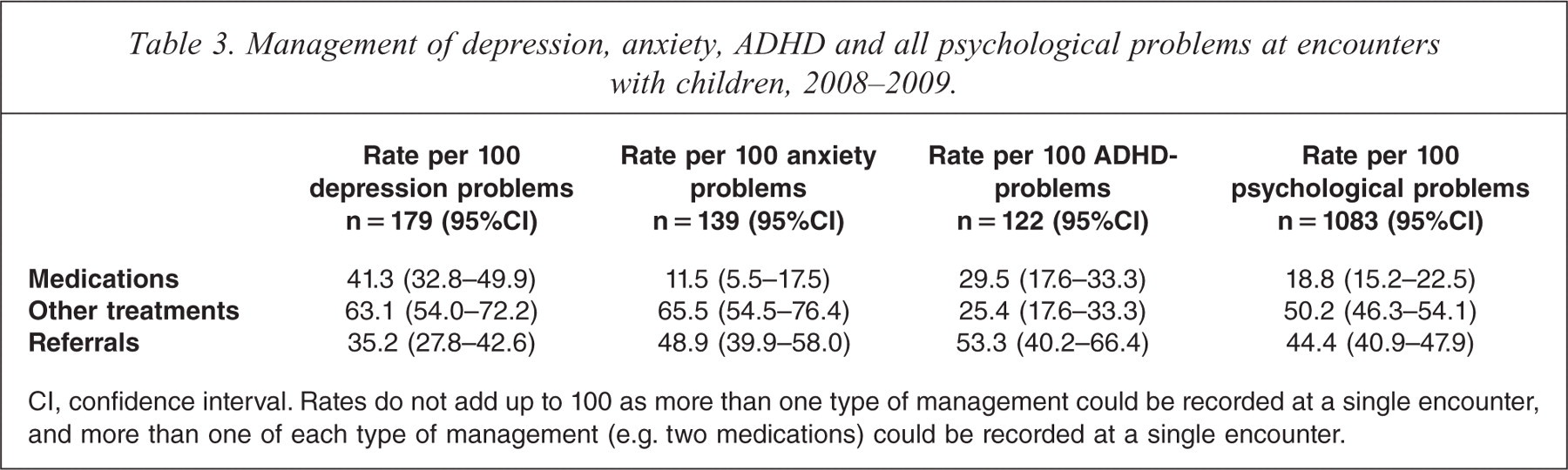
CI, confidence interval. Rates do not add up to 100 as more than one type of management could be recorded at a single encounter, and more than one of each type of management (e.g. two medications) could be recorded at a single encounter.
Discussion
The management rates of childhood mental problems in general practice reported here correspond with the international literature review published in 2001 [11] and confirm low levels of management compared with reported prevalence of these problems among children [8,9].
Over the last four decades, the kinds of psychological problems GPs manage for children have changed. The substantial decrease in the proportion of psychological problems accounted for by enuresis/bedwetting probably reflects the modern trend of greater tolerance of enuresis in children under six years of age [29,30]. Newly defined mental problems emerged during the study period and have taken over from formerly common complaints such as enuresis and insomnia.
ADHD was not included in the Diagnostics and Statistics Manual of Mental Disorders until DSM-III-R in 1987, and was previously referred to as ADD in DSM-III in 1980 [31]. Before that, ‘hyperkinetic impulse disorder’ was discussed in the literature of the 1950s as a childhood behaviour disorder [32]. Our results show that ADHD began to appear as a specific condition managed in general practice in the 1991 survey, but some cases may still have been labelled as ‘behaviour disorder’ which made up a larger proportion of children's psychological problems in 1971 and 1991 than in 2008–2009.
Similarly, autism was not listed in ICD-9 by the World Health Organization until 1975, and in DSM-III it was not included as a separate diagnostic category until 1980 although it had been recognized as a condition since the 1940s [33]. Our data showed only three cases of ‘other unspecified psychosis’ in 1990–1991, yet 10 years later autism spectrum disorders accounted for 5% of children's mental problems, with the proportion more than doubling in the next eight years. The increase may be partly due to earlier diagnosis and wider definition, as well as improved availability of services for patients with an autism spectrum disorder.
Our study supports previous research from around the world showing an increase in mental health problems among children[13–15]. We found that in Australian general practice over the past 20 years, the rate at which children's psychological problems were managed more than doubled. One could argue that the importance of GPs' role in the overall management of psychological problems in children increased proportionally over the same period.
Between 2000–2001 and 2008–2009 we saw a shift in the way GPs managed psychological problems in children, towards transfer of care to other health professionals and away from prescription of medications and use of other treatments. This is probably due to the introduction of the Better Access to Psychiatrists, Psychologists and General Practitioners initiative in November 2006 which made it easier for GPs to refer their patients for subsidized care from psychologists. This theory is supported by the high proportion of childhood psychological encounters claimed as GP Mental Health Care items (16.8%) compared with the proportion of all psychological encounters in BEACH where those items were claimed, which was about 7% in 2006–2008 [17].
The current management methods used by GPs for children with mental problems were of interest. The very low rates of medication show that GPs are disinclined to manage psychological problems in the young with medication. The rate for encounters with patients of all ages in BEACH over a similar time period was three times higher (65 medications per 100 psychological problems managed) [34]. GPs were much more likely to refer than to prescribe. Our results show that despite these referral rates, children with mental problems were still counselled by GPs at the same rate seen in the management of psychological problems in patients of all ages at BEACH encounters – about 50 times per 100 psychological problems managed [34]. Children managed for depression or anxiety were especially likely to receive counselling.
Our study has some limitations. The 1969–1974 Morbidity and Prescribing Survey was a precursor of the 1990–1991 AMTS which was itself a forerunner of BEACH, and the three surveys had some methods in common. Even so, comparisons with the 1969–1974 survey were limited to the published results, and were of necessity descriptive only. AMTS data were classified using ICPC-1, while BEACH data were classified in ICPC-2. Although these two versions are similar, some differences exist as we have seen; for example, with autism spectrum disorder. There is also a limitation in the scope of this paper, which does not investigate management of children's psychological problems by professionals other than GPs.
Access to the three studies allowed us to consider trends in childhood mental health over a 40 year period. We examined the development of newly defined conditions which have replaced traditional childhood diagnoses of past decades. In recent years, GP involvement in mental health care management in children has grown significantly. The GP's role as gate keeper to other mental health specialists was reinforced with the introduction of initiatives such as Better Access. However, the reduction in Better Access payments announced in the Australian government budget of 2011 [35] may have a negative impact on GP participation in this programme, making it more difficult to predict the future role of the GP in children's mental health care.
Acknowledgements
The authors thank the GP participants in the BEACH programme and all members of the BEACH team.