
Abstract
Objective:
This study examines the uptake by children aged predominantly 0–11 years of an Australian primary mental health service – the Access to Allied Psychological Services programme – which began in 2001. In particular, it considers access to, and use of, the child component of Access to Allied Psychological Services, the Child Mental Health Service, introduced in 2010.
Method:
Using routinely collected programme data from a national minimum dataset and regional population data, we conducted descriptive and regression analysis to examine programme uptake, predictors of service reach and consumer- and treatment-based characteristics of service.
Results:
Between 2003 and 2013, 18,631 referrals for children were made and 75,178 sessions were scheduled via Access to Allied Psychological Services, over 50% of which were via the Child Mental Health Service in its first 3 years of operation. The rate of referrals for children to the Child Mental Health Service was associated with the rate of Access to Allied Psychological Services referrals for consumers aged 12+ years.
Conclusions:
The Child Mental Health Service has increased services provided within the Access to Allied Psychological Services programme for children with emotional and behavioural issues and their families, and is potentially filling a service gap in the area of prevention and early intervention for children who have significant levels of need but are unable to access other mental health services. Our findings are policy-relevant for other developed countries with a similar primary mental health care system that are considering means of improving service access by children.
Introduction
Childhood, defined in this paper as ages 0–11 years inclusive, is a crucial developmental period. Childhood emotional and behavioural problems are an important public health concern in Australia and internationally. Early identification of children at risk of emotional and behavioural problems creates opportunities for intervention that can help to avert or ameliorate problems in later life. Access to services tailored to children that focus on early identification and treatment may mitigate the persistence or severity of primary disorders and prevent comorbid disorders (Kessler et al., 2007). Primary mental health services have an important role to play in recognising vulnerable children and offering appropriate care and support. This paper describes utilisation by children of an Australian primary mental health programme, which introduced services specifically tailored for children.
Child emotional and behavioural health in Australia
The most recent Australian survey of child and adolescent mental health, conducted in 2013–2014, recruited 6310 parents and carers of children aged 4–17 years and 2967 children aged 11–17 years and found that 14% of children and adolescents had a mental disorder in the previous year, which was associated with a substantial number of days absent from school (Lawrence et al., 2016). Furthermore, the survey found that 56% of 4- to 17-year-olds with mental disorders had accessed mental health services (e.g. family doctors, psychologists, paediatricians and counsellors/family therapists) in the year preceding the survey (Johnson et al., 2016), which is an improvement on the rate of service use reported in 1997 − 25% in the preceding 6 months (Sawyer et al., 2000).
The Access to Allied Psychological Services programme
The Access to Allied Psychological Services (ATAPS) programme has been delivering primary mental health services to the Australian community since 2001, with an evolving emphasis on hard-to-reach groups. ATAPS was the first programme to provide community access to government-funded psychological treatment of common mental disorders in Australia. ATAPS was implemented through Divisions of General Practice (‘Divisions’), which transitioned to Medicare Locals in 2011–2012 (in a series of funding rounds or ‘tranches’) to support general practitioners (GPs; ‘family physicians’) and mental health professionals to collaborate to provide optimal primary mental health care. ATAPS enabled GPs to refer consumers of any age with high prevalence disorders (e.g. depression and anxiety) to mental health professionals for up to 12 (or 18 in exceptional circumstances) individual sessions, with the option for an additional 12 group sessions of evidence-based mental health care (predominantly Cognitive Behavioural Therapy, or CBT) (Hickie and Groom, 2002). Review by the referring GP was mandatory after each block of six sessions and/or the final session.
During the life of ATAPS, several ATAPS initiatives were introduced that focussed on particular at-risk populations, including women with perinatal depression; people at risk of suicide or self-harm (King et al., 2013); people experiencing, or at risk of, homelessness; people affected by extreme climatic events, such as bushfires (Bassilios et al., 2012b) or floods (Reifels et al., 2015); people in remote locations (Morley et al., 2007); and children with, or at risk of developing, a mental, childhood behavioural or emotional disorder. Some initiatives have also used alternative modalities to face-to-face service delivery, such as telephone- or web-based CBT (Bassilios et al., 2012a). These additional initiatives aimed to enhance capacity to address the needs of these groups and provide increased service flexibility (Reifels et al., 2013). The original ATAPS arrangements came to be known as the ‘Tier 1’ initiative, and the sub-programmes as the ‘Tier 2’ initiatives (Australian Government Department of Health and Ageing, 2012a). These initiatives were introduced at different times since 2008; some of them were mandatory, while others were elective for Medicare Locals.
From July 2016, government-funded primary care psychological treatment for people of all ages will be locally commissioned by 30 Primary Health Networks (which replaced Medicare Locals in July 2015). This reform will be supported by a flexible funding pool for mental health and suicide prevention services that enables targeting services within a stepped care approach according to local population mental health needs (Department of Health, 2014). This policy change has resulted from a major review of national mental health services completed in 2014 (National Mental Health Commission, 2014) and the Department of Health response to this review (Australian Government Department of Health, 2015).
The ATAPS Child Mental Health Service
The ATAPS Child Mental Health Service (CMHS) was introduced in July 2010 and was primarily aimed at children aged 11 years or under with, or at risk of developing, a mental, behavioural or emotional disorder. Its objectives were (1) to increase ATAPS service delivery provided for children with mental health and behavioural issues and their families; (2) to provide a high-quality standard of service that is clinically appropriate for children, including the provision of education and training resources to support service delivery; and (3) to establish and maintain linkages and support networks with mental health service providers and community workers, including school counsellors.
In exceptional circumstances, children aged between 12 and 15 years, inclusive, could also receive services via the CMHS.
The CMHS offered ATAPS providers with greater flexibility to deliver appropriate treatment and support than Tier 1 ATAPS. Specifically, a diagnosis was not mandatory and referrals could be made by school counsellors, school principals and directors of early childhood services (as well as by GPs, psychiatrists, ATAPS mental health professionals and paediatricians who could refer across the whole of ATAPS). Up to the first three sessions could be used for the purpose of assessment. Services could include family interventions based on behaviour therapy, parent training in behaviour management, attachment intervention, parent–child interaction therapy and liaison with key providers in the children’s other environments, such as schools. Finally, sessions could involve parents or the whole family with or without the child present (whereas in other ATAPS initiatives, parents could not attend sessions related to the child unless the child was present).
ATAPS funding was significantly increased in the 2011–2012 Australian Federal Budget to enhance capacity to provide services to an additional 50,000 children and their families over 5 years (Australian Government Department of Health and Ageing, 2012b). Consequently, implementation of the CMHS became mandatory for all Medicare Locals in July 2012. In order to assist Medicare Locals with the quality implementation of the CMHS, the Department of Health provided them with funding for additional supports and resources (Australian Government Department of Health and Ageing, 2012b). For example, Medicare Locals were able to engage staff to a maximum of one full-time equivalent in order to fulfil the function of CMHS Coordination and Liaison – that is, to develop and maintain effective linkages with service providers and community groups to meet the objectives of the CMHS. Medicare Locals were also granted 3 months to enhance and expand existing services in order to more appropriately meet the needs of children and their families. This allowed for the establishment of formal linkages and referral pathways, engagement or up-skilling of mental health professionals, and development and promotion of support structures. Additionally, the Australian Psychological Society was funded to develop online training for mental health professionals who required up-skilling to meet the necessary skills and competencies to deliver the CMHS.
This is the first in-depth study of the CMHS and aims to determine (1) whether there has been an increase in services provided to children via ATAPS (from July 2003 to June 2013) since the introduction of the CMHS (in July 2010), (2) which Medicare Local regional factors are associated with differential uptake of the CMHS, (3) the socio-demographic characteristics of children accessing the CMHS and (4) the nature of the treatment delivered within the CMHS.
Method
Ethical clearance for the study was provided by the University of Melbourne’s Human Ethics Committee (Ethics ID 1136812.2).
Data sources
Minimum dataset
We extracted the following data from a purpose-designed minimum dataset: the number of referrals and sessions delivered to children aged 0–11 years (via the CMHS and ATAPS overall) and the referral and treatment characteristics for those referred to the CMHS. The minimum dataset captures de-identified, consumer-level and session-level information, which is collected by providers and entered by Medicare Local staff or providers as required by Medicare Locals’ funding agreement with the Department of Health. Data for the period from 1 July 2003 to 30 June 2013 were downloaded on 28 October 2013.
Medicare local-level population data
Medicare Locals were established in three tranches: 19 in Tranche 1 from 1 July 2011, 18 in Tranche 2 from 1 January 2012 and 24 in Tranche 3 from 1 July 2012. The Department of Health provided us with 2009 Australian Bureau of Statistics Estimated Resident Populations for each Medicare Local (including total population and population aged 0–11 years), based on 2006 Australian Census data. The data were disaggregated by the Socio-Economic Indexes for Areas (SEIFA) Index for Relative Socio-Economic Disadvantage (IRSED, in quintiles) (Australian Bureau of Statistics, 2008) and the Australian Standard Geographical Classification Remoteness Area (ASGC-RA) classifications (major cities, inner regional, outer regional, remote and very remote) (Australian Bureau of Statistics, 2013), also derived from the 2006 census data. Together with the tranche of each Medicare Local, these data were used to explore factors that might contribute to levels of service delivery by Medicare Locals.
Data analyses
Descriptive analyses
Using SPSS Version 21, simple frequencies and percentages were calculated from the minimum dataset data to report on trends in uptake of the CMHS specifically and on uptake of other ATAPS initiatives by children, socio-demographic and clinical characteristics of consumers of the CMHS and the types of services delivered within the CMHS.
Regression analysis
We performed standard multiple regression analysis to identify the factors associated with differential service reach to children by Medicare Locals via the CMHS. Our dependent variable was defined as the number of unique children referred to the CMHS (noting that an individual child could have multiple referrals) divided by the total number of children in the population per year in each Medicare Local. We express this as a rate per 100 per year.
We used the Medicare Local as the unit of analysis, meaning that all of our predictor variables were measured at the Medicare Local-level. Our independent (predictor) variables were the proportion of children in the population in the two most disadvantaged quintiles in each Medicare Local; the proportion of children residing in outer regional, remote and very remote locations in each Medicare Local; the referral rate for consumers aged 12+ years; and the tranche in which each Medicare Local was funded. The referral rate for consumers aged 12+ years was defined as the number of people referred to ATAPS aged 12+ years divided by the total number of people in the population aged 12+ years per year in each Medicare Local (expressed as a rate per 100 per year). These predictors were considered relevant as the rate of child referrals could be influenced by socio-economic status, geographic location, the overall rate of referrals to a given Medicare Local and duration since establishment of each Medicare Local.
Results
Uptake of ATAPS by children
Figure 1 shows the number of referrals for children made to the CMHS and all other ATAPS initiatives between July 2003 and June 2013, by financial year. Overall, 18,631 referrals for children were received via all ATAPS initiatives during this 10-year period, more than half (n = 9586 or 51.5%) of which were received via the CMHS in its first 3 years of operation. Since its introduction, the proportion of children referred to the CMHS as compared with other initiatives has steadily increased from 46.5% in 2010–2011 to 84.3% in 2012–2013. Moreover, since the CMHS was introduced, the overall number of children referred to ATAPS in general almost tripled, from 2295 in 2010–2011 to 6797 in 2012–2013. Correspondingly, the proportion of referrals for children to all ATAPS initiatives (4.8% overall, not shown) steadily increased from 0.9% in 2003–2004 to 3.7% in 2009–2010 (prior to the introduction of the CMHS) and 9.7% in 2012–2013.
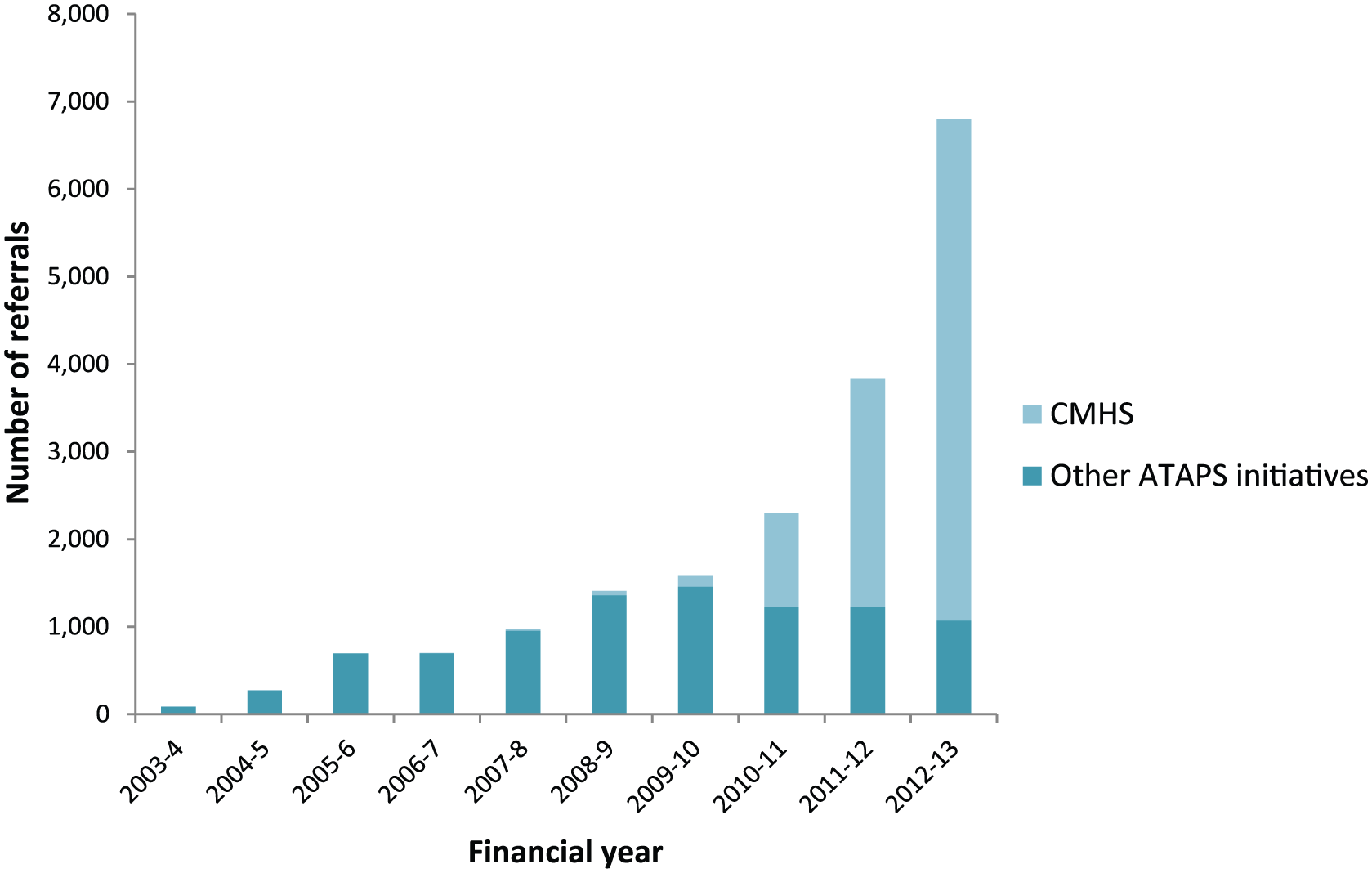
Number of referrals for children to ATAPS initiatives (July 2003 to June 2013), by financial year.
Overall, 15,018 referrals (80.6%) for children to all ATAPS initiatives and 7850 referrals (81.9%) for children to the CMHS resulted in one or more sessions scheduled by a mental health professional.
Overall, 75,178 sessions were offered to children in the 10-year analysis period, 51.1% (n = 38,420) of which were offered via the CMHS in its first 3 years of operation. In total, 4408 sessions (5.9%) offered to children were unattended, 2566 of which were unattended in the CMHS. The average number of sessions per referral offered via the CMHS was 5.4 (including unattended sessions) and 4.9 (attended sessions only). Consistent with the referral pattern, since its introduction, the proportion of ATAPS sessions delivered to children via the CMHS steadily increased from 41.4% in 2010–2011 to 81.9% in 2012–2013. Furthermore, since the introduction of the CMHS, the overall number of sessions delivered to children more than tripled from 8773 in 2010–2011 to 28,954 in 2012–2013. Overall, sessions delivered to children comprised 4.7% of all sessions delivered via any ATAPS initiative in the 10-year analysis period; this proportion steadily increased from 0.6% in 2003–2004 to 3.6% in 2009–2010 (prior to the introduction of the CMHS) and 8.9% in 2012–2013.
Predictors of referrals to the CMHS
Table 1 shows the correlations between the independent variables and rate of children referred to the CMHS as a proportion of the population of children in each Medicare Local (the dependent variable) and the regression coefficients (B) for the independent (predictor) variables. As shown in Table 1, the combination of all four predictor variables in the regression equation accounted for a significant percentage of variance (19%) in the rate of referral of children to the CMHS, R = 0.44, F(4, 56) = 3.29, p = 0.02. However, only the rate of ATAPS referrals for consumers aged 12+ years made a significant independent contribution to the prediction of the rate of referral of children to the CMHS. These findings indicate that the rate at which children are referred to the CMHS is associated with the rate of referrals aged 12+ years to ATAPS; for every 1% increase in the rate of referrals aged 12+ years to ATAPS in a Medicare Local, the rate of children referred to the CMHS increased by 0.06%.
Simple correlations between predictor variables and rate of children referred to the CMHS, and regression coefficients (B).
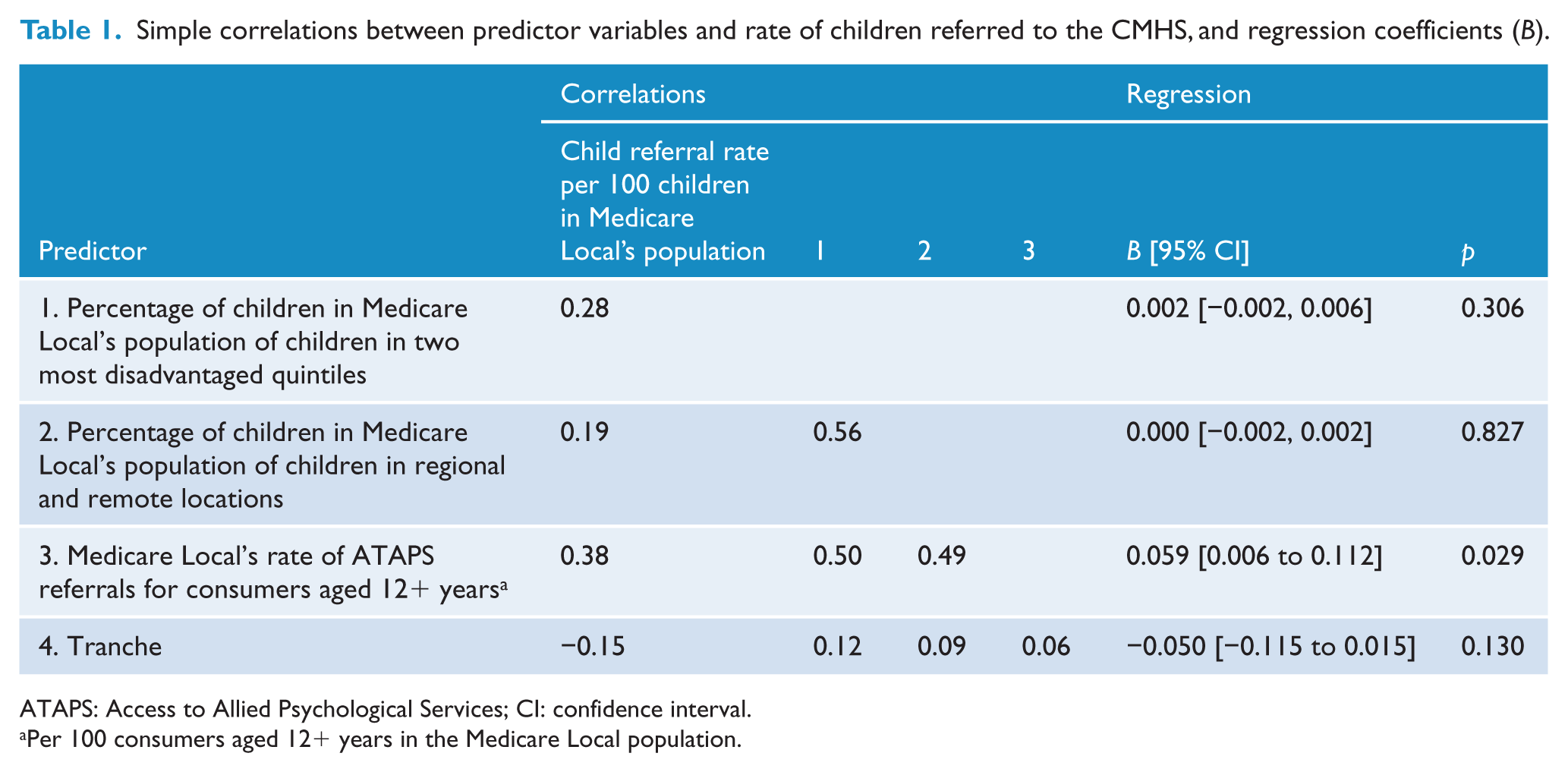
ATAPS: Access to Allied Psychological Services; CI: confidence interval.
Per 100 consumers aged 12+ years in the Medicare Local population.
Demographic and clinical characteristics of CMHS consumers
Table 2 summarises the key characteristics of the 9586 referrals (representing 9090 individuals) to the CMHS, and where available comparable percentage breakdowns for all Australian children using 2006 Census data (Australian Bureau of Statistics, 2007) to be consistent with the data source used for Medicare Local characteristics. Proportionally, the CMHS seems to at least marginally target difficult-to-reach sub-populations of children, such as males, Indigenous people and those residing in regional locations; however, children residing in remote areas appear to be under-serviced, and the level of access by children from Culturally and Linguistically Diverse backgrounds is unclear given that data related to language spoken at home were missing for 13% of CMHS consumers. The mean age of children referred to the CMHS was 9.5 years. A small proportion of referrals to the CMHS (6.8%) appears to be for children aged over 15 years, although this could reflect errors in data entry. Of all referrals for children to the CMHS, over 38% were aged 5–9 years, slightly more were male than female (52.4% vs 46.4%), 4.6% were Aboriginal and/or Torres Strait Islanders, 86.2% spoke English at home and 60% were reported to be from a family with a low income (based on the referrer’s judgement). Referred children mainly resided in major cities (56.2%), or regional locations (38.1%).
Demographic and clinical characteristics of children referred to the CMHS (and all Australian children), and interventions delivered.
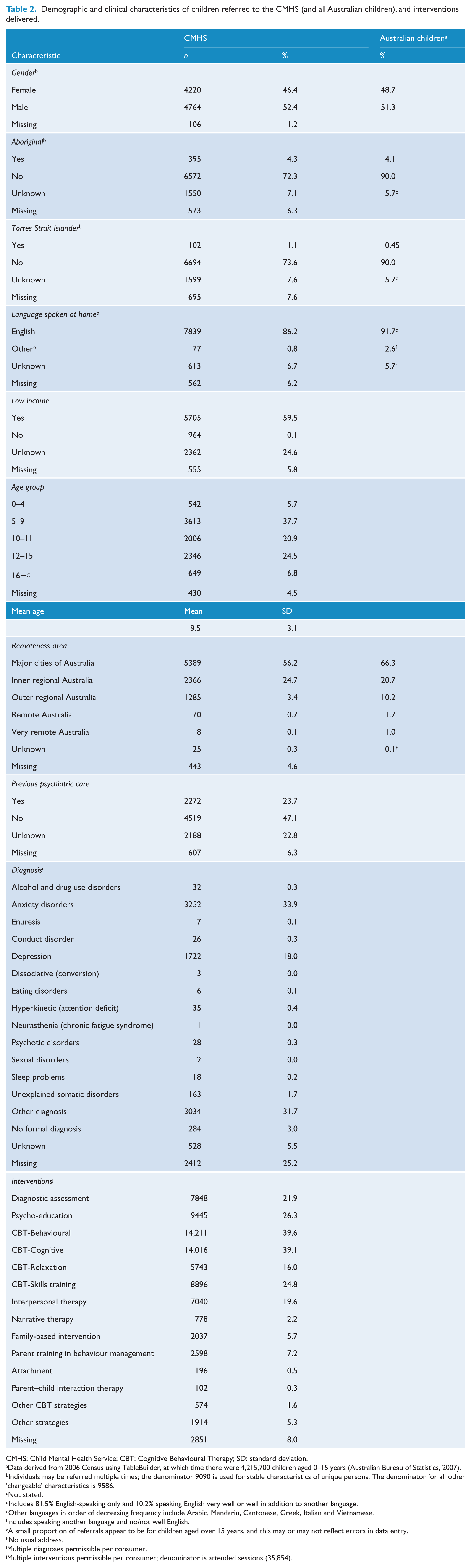
CMHS: Child Mental Health Service; CBT: Cognitive Behavioural Therapy; SD: standard deviation.
Data derived from 2006 Census using TableBuilder, at which time there were 4,215,700 children aged 0–15 years (Australian Bureau of Statistics, 2007).
Individuals may be referred multiple times; the denominator 9090 is used for stable characteristics of unique persons. The denominator for all other ‘changeable’ characteristics is 9586.
Not stated.
Includes 81.5% English-speaking only and 10.2% speaking English very well or well in addition to another language.
Other languages in order of decreasing frequency include Arabic, Mandarin, Cantonese, Greek, Italian and Vietnamese.
Includes speaking another language and no/not well English.
A small proportion of referrals appear to be for children aged over 15 years, and this may or may not reflect errors in data entry.
No usual address.
Multiple diagnoses permissible per consumer.
Multiple interventions permissible per consumer; denominator is attended sessions (35,854).
The most commonly reported diagnoses were anxiety disorders (33.9%), depression (18.0%) and ‘other’ diagnoses (31.7%). The high proportion of ‘other’ diagnoses is explained by the relatively recent introduction of child-specific diagnoses (i.e. enuresis, conduct disorder, dissociative disorder, eating disorders, hyperkinetic disorder, neurasthenia, sexual disorders and sleep problems) to the minimum dataset in May 2013. Prior to this, the diagnosis of children with these disorders would have been classified as ‘other’ diagnosis in the minimum dataset. In all, 3% of children were classified as not having a formal diagnosis, which is consistent with the CMHS Operational Guidelines deeming children who are ‘at risk’ of developing a mental disorder as eligible for the service (Australian Government Department of Health and Ageing, 2012b). Of all children referred to the CMHS, close to half had not previously accessed psychiatric care (47.1%).
CMHS treatment characteristics
The majority of sessions (n = 35,854 or 93.3%) scheduled via the CMHS were attended by consumers or their families. These sessions were delivered to either the child alone (37.8%), one or more parents and/or family members without the child present (3.0%), or individuals (either child or parent or other family member; 35.0%). Around 16% of sessions were delivered with both the child and one or more parents or family members present. Finally, 4.7% of sessions were delivered in a group format, meaning the child and/or parents or family members received psychological therapy along with a group of other children and/or parents or family members. Information about who attended the session was missing for 3.9% of sessions. Most sessions were of 46–60 minutes duration (88.4%), 8.6% were over 60 minutes and 2.2% were less than 46 minutes duration. The vast majority of attended sessions (93.5%) were delivered face to face, with 0.7% of sessions delivered via the telephone. Web-based and videoconferencing sessions were very rare (n = 28). Only 5.9% or 2118 of 35,854 sessions incurred a co-payment over the life of the CMHS. The mean co-payment amount (for sessions incurring a co-payment) across all years was AUD21.97 (standard deviation [SD] = AUD24.28). The mean cost per session (for all sessions delivered) amounts to AUD2.86 (SD = AUD11.47).
Table 2 shows the intervention types delivered in CMHS sessions. The most common interventions were CBT-behavioural (39.6%) and CBT-cognitive (39.1%) interventions, accounting for 14,211 and 14,016 sessions, respectively. This was followed by psycho-education (26.3%), CBT-skills training (24.8%), diagnostic assessment (21.9%) and interpersonal therapy (19.6%). Around 56% (or 4419 of 7850) of referrals who took up the service received sessions that were classified as involving diagnostic assessment (not shown). Of the 4419 CMHS referrals (or 7848 CMHS sessions) involving diagnostic assessment, the majority received one (60.3%), two (23.0%) or three (8.3%) separate assessment sessions.
Discussion
This study examined mental health service delivery to children via the CMHS. Our first aim was to determine whether there had been an increase in services provided to children via ATAPS since the introduction of the CMHS. We have shown that there was a steady increase in the number of children (and their corresponding sessions) over the life of ATAPS, which became more pronounced after the introduction of the CMHS, with the overall number of children referred to ATAPS nearly tripling from 2295 in 2010–2011 to 6797 in 2012–2013. Although it is unlikely that this level of service use would have existed outside of ATAPS, it is possible that a minority of families (those less socio-economically disadvantaged) may have purchased similar services prior to its introduction. Furthermore, although uptake of ATAPS by children/families is substantial, it should be contextualised in terms of other available mental health care pathways available in Australia – specialist mental health services and ambulatory or residential mental health-related care provided by general health services. For example, Medicare-subsidised mental health–related services (provided by psychologists and other allied health professionals) were received by over 104,000 children aged 14 years and under in 2012–2013 (Australian Institute of Health and Welfare, 2014). Despite its relatively smaller reach, because of its unique service provision characteristics, the CMHS is complementary in that it has the potential to reach consumers with a different profile.
Our second aim was to explore Medicare Local regional factors associated with differential uptake of the CMHS. Of the factors examined in relation to their impact on uptake by children, only the rate of referrals aged 12+ years was significantly associated with levels of service delivery to children. This finding could suggest that in regions where referrers are cognisant of and referring consumers to ATAPS, they are likely to refer consumers irrespective of their age. This effect may have been related to the extent of Medicare Locals’ ‘presence’ in the community, promotion of ATAPS and its CMHS, partnerships with health and other stakeholder agencies, and other factors impacting on their overall performance within the health care landscape. The fact that socio-economic position, geographic spread and date of establishment of Medicare Locals were not significantly associated with levels of service delivery to children could suggest that, like the overall ATAPS programme (Bassilios et al., 2010), the CMHS is providing relatively equal access to services, which is at least in part attributable to the service being generally available for free. By contrast, although Australia’s larger scale Medicare-subsidised Better Access programme has a far greater reach, around three-quarters of its total consumers are from major cities or other major metropolitan centres and socio-economically disadvantaged people are less likely than socio-economically advantaged people to utilise Better Access (Harris et al., 2010).
The rate of uptake of services (acceptance of referral) by children and their families was very similar to the overall uptake rate of ATAPS by consumers of all ages (81% vs 79% referrals resulting in sessions) (Bassilios et al., 2013) and superior to that observed in other studies. For example, one study of 363 patients reported that 48% of people referred to the UK Improving Access to Psychological Therapy (IAPT) programme did not take up the service, despite being referred by their GP (Di Bona et al., 2014). Potential reasons for not taking up the CMHS include communication between GPs and parents, parent perception that CBT treatment is either not needed or will not be useful (Morgan et al., 2014), stigma associated with mental health problems and receiving treatment (Clement et al., 2014), access barriers (travel, cost, waiting time for services), family discord or crises (Smith et al., 2013) and actual or hoped natural resolution of symptoms.
Our third and fourth aims were to describe the socio-demographic characteristics of children accessing the CMHS and the nature of the treatment delivered, respectively. Some consumer and service characteristics are noteworthy. For example, slightly more males than females were referred (52% vs 46%), which is desirable given that the prevalence of mental disorders is slightly higher in boys than girls (Sawyer et al., 2000). The fact that Indigenous children accounted for 4.6% of referrals is promising given that 4.2% of Australia’s children and young people are Indigenous (Australian Bureau of Statistics, 2011). The majority of children/families were considered to receive a low income, which is consistent with the aim of the overall ATAPS programme of targeting people who are hard to reach.
The CMHS flexibility for parents to attend sessions with or without their children is favoured by stakeholders in terms of the therapeutic benefit conferred to the child and family (Bassilios et al., 2014). This valued option is not available via other ATAPS initiatives, nor via Better Access (Pirkis et al., 2011). CBT-skills training and diagnostic assessment were more commonly delivered in the CMHS than in overall ATAPS (25% vs 18% and 22% vs 16%, respectively). Variations in the interventions delivered via the CMHS might be attributable to some of the flexibilities of the CMHS permitted by the guidelines, such as the allowance of up to three sessions per referral to be used for assessment and the possibility of parents attending sessions with or without the child. For example, the latter might account for the elevated use of CBT-skills training within the CMHS. However, it should be noted that the fidelity of interventions delivered via ATAPS is not currently assessed.
Limitations
Findings should be interpreted in the context of several limitations. Data from the minimum dataset are prone to missing data in some non-mandatory variables, the addition of new data fields to reflect changes to programme guidelines and actual practice, lags in data entry with some Medicare Locals or providers not entering session data until all sessions for a given consumer are complete. The average number of sessions per consumer may be underestimated, as Medicare Locals differ in their ability to identify re-referrals for the same consumer which means they may inadvertently assign a given consumer both a new patient identification number and referral number after the initial six sessions. The population characteristics data used in the regression analyses were limited in type and number, and may have masked heterogeneity within the Medicare Local areas. Furthermore, these data did not take into account the prevalence of mental disorders in children in the population or the availability and utilisation of other (non-ATAPS) mental health services, in each Medicare Local region, the data for which were not available at the time of our analyses. Therefore, the extent to which the CMHS is meeting demand for children’s mental health services could not be determined. Although all Medicare Locals were implementing the CMHS at the time of our analysis, they were in varied stages of implementation, which was not included as a predictor. Future research could investigate other factors potentially impacting on access to primary care psychological treatment in the new Primary Health Network regions with a view to developing strategies to improve reach to consumers of all ages.
Finally, sufficient outcome data for statistical analysis were not yet available, which may be attributable to factors ranging from clinician willingness to administer and report outcome data (Cesare, 2013) to consumer dropout either due to symptom improvement or disengagement from therapy. Improved recording of outcome measure scores and/or reasons for termination as standard would assist in better understanding the outcomes of the CMHS. Strategies to improve the proportion of outcome data could include more regular monitoring of outcomes (Wolpert et al., 2012) than at the first, sixth and/or final session and promoting the clinical utility (Cesare, 2013) of outcome measurement to providers (e.g. informing clinical work, monitoring programmes, modelling data to produce intervention norms) (Wolpert et al., 2012).
Conclusion
The CMHS was successful in increasing services provided within the ATAPS programme for children with emotional and behavioural issues and their families, and led to rapid uptake. This finding suggests that the CMHS is potentially filling a service gap in the area of prevention and early intervention for children who are unable to access other and larger scale mental health services. There are indications that levels of service delivery to children are unrelated to socio-economic position, residence in regional and remote locations and date of establishment of Medicare Locals. It will be interesting to see what impact the imminent changes in Australia’s primary mental health care landscape have on service reach to children. Our findings are policy-relevant for other developed countries with a similar primary mental health care system that are considering means of improving service access by children. Future research could examine outcome data for children receiving primary mental health care, including reasons for termination, in order to determine the impact on symptoms and functioning.
Footnotes
Acknowledgements
Strategic Data Pty Ltd developed and maintains the minimum dataset from which the data for this study were extracted. An early version of this paper was presented at the 49th Australian Psychological Society Conference in Hobart, Australia, on 30 September 2014.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported through funding from the Australian Government Department of Health.