
Abstract
With numerous epidemiological studies finding that moderate alcohol consumption is associated with a reduced risk of dementia in late life [1], alcohol-related dementia has had limited attention in recent years. It has long been known that excessive alcohol consumption can cause severe and sometimes permanent cognitive deficits, including alcohol-related dementia, withdrawal syndromes and frontal lobe syndrome, as well as Wernicke's encephalopathy and Korsakoff (amnesic) syndrome through associated thiamine deficiency [2]. Significant clinical and neuropathological overlap between these disorders has been reported [3].
Because alcohol abuse is associated with a large range of physical and mental comorbidities, general hospital admission is common in this population [4]. Alcohol-related cognitive disturbances often become apparent to hospital clinicians during withdrawal in the first few days of admission or due to persistent confusion following recovery from the acute physical disorder that precipitated admission. In a study of early-onset dementia, a high proportion of subjects identified with alcohol-related dementia were diagnosed during a general hospital admission rather than through a memory clinic – a different pattern from that found in Alzheimer's disease, fronto-temporal dementia and vascular dementia [5]. Hence the general hospital is likely to be a setting in which alcohol-related cognitive disorders are identified and interventions planned [6].
The Hospital Dementia Services Project (HDS) is an innovative study that explores at the patient level how hospital experiences and outcomes vary for people with and without dementia, and at the system level how hospital-based aged care and dementia care influence outcomes for people with dementia. The study focuses on people aged 50 and over admitted to a public hospital in the state of New South Wales (NSW) (total population 6.9 million), Australia in 2006/7. The age of 50 was chosen as the age cut-off because there are relatively few cases of dementia under this age. In a previous paper from this study, we demonstrated that alcohol-related dementia (ARD) was age-related, on its own accounting for just over 20% of diagnosed cases of dementia under the age of 65 and less than 1% of cases aged 65 years and over [7].
Although the focus of this paper is on ARD, due to the previously mentioned overlap between alcohol-related cognitive disorders, we will also examine Wernicke's encephalopathy and amnesic syndrome due to alcohol. The aims of this paper are to document the prevalence of alcohol related dementia (ARD), Wernicke's encephalopathy and amnesic syndrome due to alcohol; to describe the principal reasons for admission, medical comorbidities, interventions and outcomes recorded for patients with ARD; and to compare ARD patients on these variables with other dementia patients. The analysis includes stays in both public and private hospitals for these people.
Methods
For this study, data were extracted by the NSW Department of Health from the NSW Admitted Patient Care Database for hospital episodes in public and private NSW hospitals between 1 July 2005 and 30 June 2007. The Admitted Patient Care Database records new episodes for every within-hospital change in care type and each transfer between hospitals [8]. A unique patient identifier, derived by the Centre for Health Record Linkage (or CHeReL), was added to the extract. This permitted all hospital episodes belonging to the same patient to be combined into a single completed hospital stay (i.e. from initial admission to final discharge from hospital, allowing for movement both within and between hospitals). It also allowed the identification of readmissions by individuals. Transfers and readmissions for individual patients were identified using episode start and end dates and reported mode of episode discharge. Previous research has relied on hospital episodes and has been unable to accurately portray the individual patient journey through the system from admission to discharge. This linking of patients' data is a major advance on earlier analyses [8,9].
Combining the patient-level hospital episode data, we identified 253 000 individuals aged at least 50 years on 1 July 2006 who had at least one multi-day stay ending between 1 July 2006 and 30 June 2007 in a public hospital in NSW (including seven public psychiatric hospitals). Between them, these people had 409 000 multi-day stays and 252 000 single day stays ending in that year across 222 public hospitals and 167 private hospitals.
Up to 55 diagnoses could potentially be recorded per episode of care. Diagnoses were coded using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) [10]. The principal diagnosis was defined as the diagnosis chiefly responsible for occasioning the hospitalization episode. Diagnoses are recorded by chapters from A to Z that correspond to a mix of organ systems, types of diseases and injuries, and miscellaneous other reasons for a health encounter.
The group of interest was patients for whom alcohol-related dementia was recorded on at least one hospital stay from July 2005 to June 2007 as contributing significantly to the cost of hospital care, the criterion used by hospital medical records department coders using standardized national coding criteria. This meant that there were admissions in which dementia was not a recorded diagnosis.
Where alcohol-related dementia was recorded on one admission and another type of dementia on the same or another hospital admission, we categorized the patient as having ‘alcohol-related dementia with mixed diagnoses’.
We also investigated for the presence of comorbid delirium, which in some cases was captured with the ICD-10-AM category ‘dementia with delirium’ and in other cases was captured as a separate diagnosis comorbid with a dementia diagnosis. The presence of other ‘mental and behavioural disorders due to use of alcohol’ (F10 in ICD-10-AM) and the subcategories (acute intoxication, harmful use, dependence syndrome, withdrawal state, withdrawal state with delirium, psychotic disorder, amnesic syndrome, residual and other late-onset psychotic disorder, other mental and behavioural disorders, unspecified mental and behavioural disorder) were determined.
Medical comorbidities were examined by counting the number of ICD-10-AM chapters recorded for the admission. We also examined other specific comorbidities associated with hospital admission including hip (femur) fractures, head injuries, lower respiratory tract infections, urinary tract infections (UTI), stroke/ transient ischaemic attacks (TIAs), subdural haematoma, Wernicke's encephalopathy, epilepsy, and septicaemia.
Procedures that were undertaken during each hospital admission were grouped into the following broad ICD10-AM categories: cardiovascular system; digestive system; musculoskeletal system; non-invasive, cognitive and other interventions; allied health; and imaging. Some specific subcategories of non-invasive procedures were examined: alcohol detoxification, electroencephalogram, neuropsychology, transfusion of blood and gamma globulin, psychosocial therapies and computerized tomography.
The following outcomes of hospitalization were examined: length of stay (LOS), mortality, discharge destination, and readmission.
Institutional ethics committee approval was obtained from the Australian Institute of Health and Welfare Ethics Committee, the NSW Population and Health Services Research Ethics Committee, the University of NSW and University of Canberra Human Research Ethics Committees, and 19 site-specific approvals that together covered all of the public hospitals in NSW.
Results
Overall, 20 793 patients aged 50 and over with a dementia diagnosis (8.2% of all HDS patients) had an admission lasting at least one night that ended between 1 July 2006 and 30 June 2007 (see Table 1). Among these patients were 268 patients with an alcohol-related dementia (ARD) diagnosis and a further 32 patients with ARD and another dementia diagnosis (ARD with mixed diagnosis). These patients had 882 multi-day stays in this period. All 300 patients with an ARD diagnosis represented 1.4% of the dementia patients and 3% of the patients diagnosed with an alcohol-related mental disorder (n = 9303). In the remainder of this paper patients with ARD or with ARD with mixed diagnosis are jointly referred to as ‘ARD patients’ and any differences between the two groups are noted in the text.
Patients aged 50 and over admitted to NSW Public Hospitals in 2006/7 with alcohol-related dementia, amnesic syndrome due to alcohol, Wernicke's encephalopathy and other dementias (N = 252719)
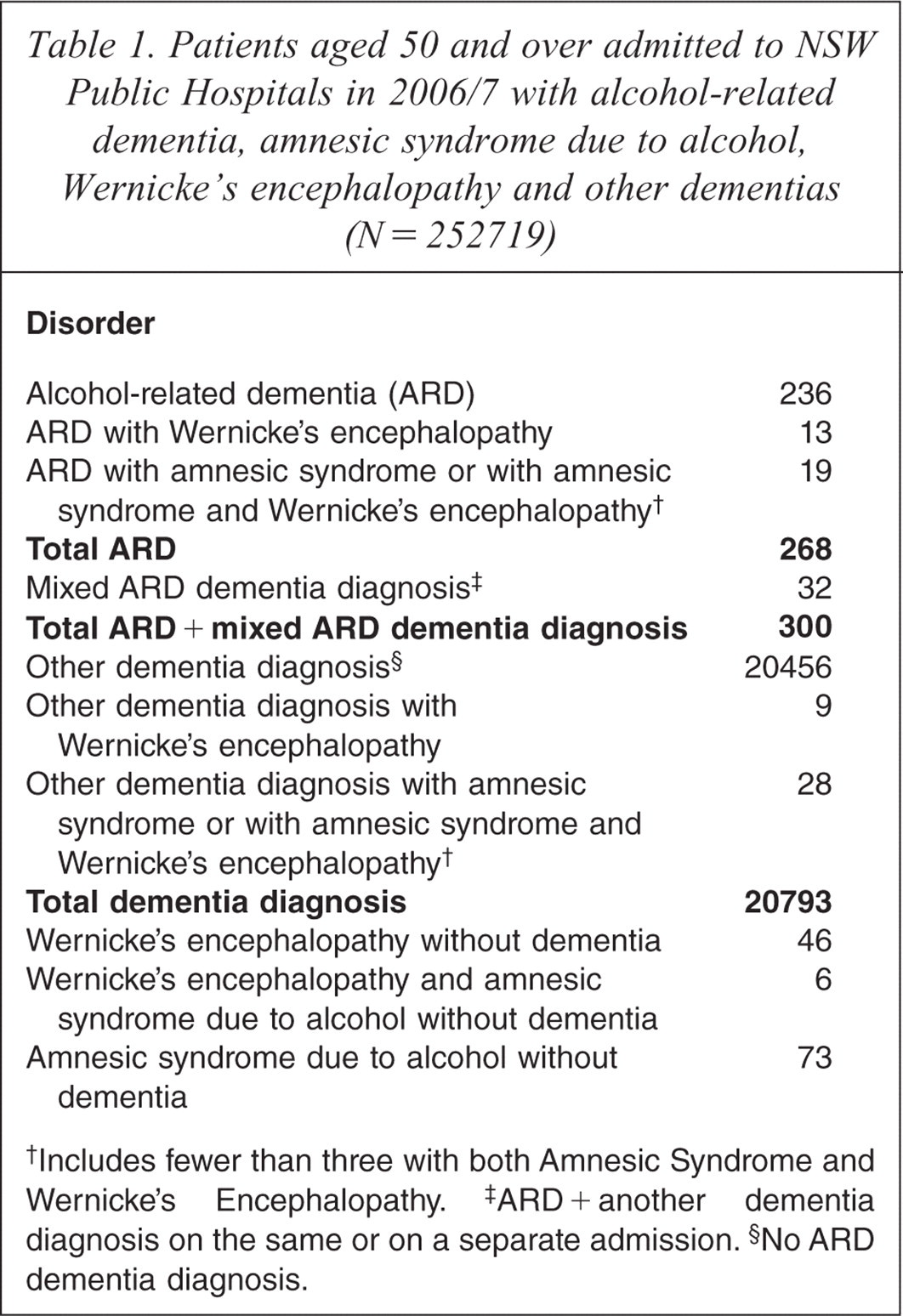
Includes fewer than three with both Amnesic Syndrome and Wernicke's Encephalopathy.
ARD + another dementia diagnosis on the same or on a separate admission.
No ARD dementia diagnosis.
The majority of the ARD patients (n = 246, 82%) were male. Overall, the mean age of the ARD patients was 65 years (median = 63.9, standard deviation 9.3 years, minimum 50.4, maximum 86.6). Patients with ‘ARD with mixed diagnosis’ (mean = 71.3 years, median = 74.0, standard deviation 8.8, minimum 53.2, maximum 84.4) were significantly older than patients only diagnosed with ARD.
Amnesic syndrome due to alcohol was diagnosed in 126 patients and in 47 of these there was a comorbid dementia diagnosis including 19 with ARD. Wernicke's encephalopathy was diagnosed in 77 patients and in 25 of these there was a comorbid dementia diagnosis including 15 with ARD. Six patients without dementia were diagnosed with amnesic syndrome due to alcohol comorbid with Wernicke's encephalopathy. Only six patients with Wernicke's encephalopathy did not have an alcohol-related mental disorder diagnosed. In total, there were 462 patients (0.2% of all patients) with ARD, Wernicke's encephalopathy associated with alcohol, or amnesic syndrome due to alcohol, although there were overlaps of the diagnostic groups with some patients attracting multiple diagnoses (see Table 1).
Principal reasons for admission for ARD patients
Dementia was the principal diagnosis in only 51 (6%) multi-day stays, and was reported as a diagnosis affecting the complexity or cost of care in 308 (35%) of stays (see Table 2). A mental or behavioural disorder was the principal reason for admission in 223 (25%) stays and was recorded in 678 (77%) stays. Many of these disorders were alcohol related, with an alcohol-related mental disorder reported for 621 (70%) multi-day hospital stays; dependence syndrome (n = 455, 52%) was by far the most frequently recorded type of alcohol-related mental disorder. Acute intoxication was reported in 120 patients (14%) and psychotic disorder due to alcohol in 91 patients (10%); both were more likely to be recorded in patients with ARD with mixed diagnoses (acute intoxication, chi square = 8.33, p < 0.01; psychotic disorder due to alcohol, chi square = 9.48, p < 0.01). However, alcohol-related mental disorders were the principal diagnosis in just under 18% of stays with dependence (n = 60, 7%) and acute intoxication (n = 56, 6%) being most frequently reported. Wernicke's encephalopathy was recorded in 22 (2.5%) stays and delirium was recorded in 3.4% of stays (see Table 2).
Principal and comorbid diagnoses for multi-day hospital stays of patients with alcohol-related dementia in NSW, 2006/7 (N = 881)
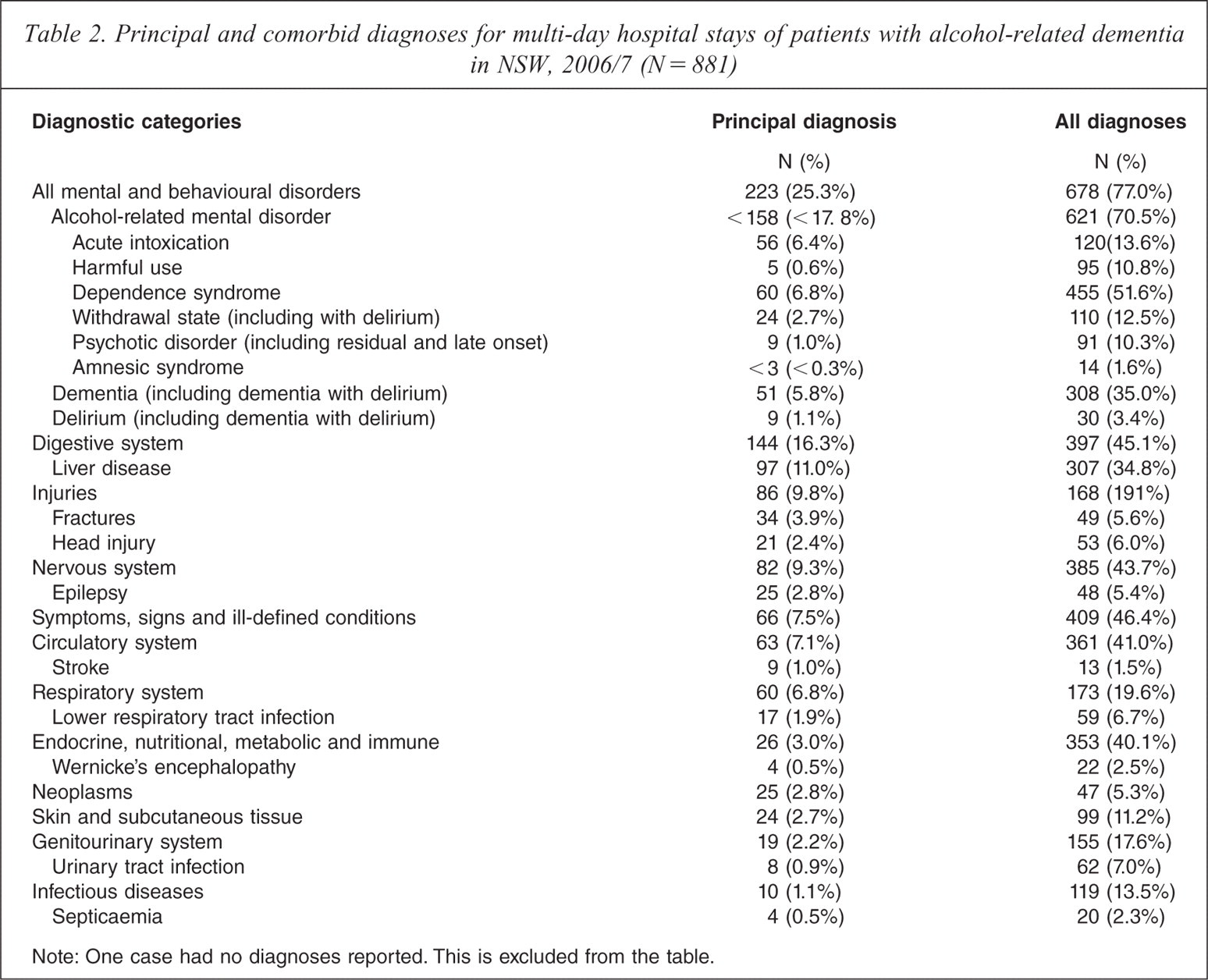
Note: One case had no diagnoses reported. This is excluded from the table.
Medical comorbidity for ARD patients
Medical comorbidity was common in the multi-day stays (mean of 4.8 ICD-10-AM chapters, median = 5, range = 1–13), with 13% of admissions having eight or more comorbidities. Liver disease was both a prominent principal reason for admission (n = 97, 12%) and often recorded as an additional diagnosis (n = 307, 35%). Other diagnoses frequently recorded as additional diagnoses included UTIs (7%), lower respiratory tract infections (7%), head injuries (6%) and epilepsy (5%). Endocrine disorders (chi square = 6.95, p < 0.01, Liver disease (chi square = 5.65, p < 0.05) and epilepsy (chi square = 4.75, p < 0.05) were less common in ARD with mixed diagnoses; while UTIs (chi square = 7.01, p < 0.01) and nervous system disorders (chi square = 13.62, p < 0.001) were more common (see Table 2).
Procedures for ARD patients
Procedures were recorded in 685 (78%) admissions. Generalized allied health interventions were the most frequently recorded procedure, occurring in 500 (57%) admissions and being the principal procedure in 192 (22%). Imaging was the second most common procedure; brain computed tomography was the most frequent of this type of investigation (n = 205, 23%) and was the principal investigation in 162 admissions (18%). Of note, formal alcohol detoxification was recorded in only 28 (3.2%) admissions, electroencephalography in only three, and no admissions included neuropsychological assessment. Transfusions (chi square = 6.70, p < 0.01) and digestive system procedures (chi square = 5.24, p < 0.05) were significantly less likely to occur in patients with ARD with mixed diagnoses, and allied health services were significantly more likely to be involved (chi square = 4.63, p < 0.05) (see Table 3).
Procedures for multi-day hospital stays of patients with alcohol-related dementia in NSW, 2006/7
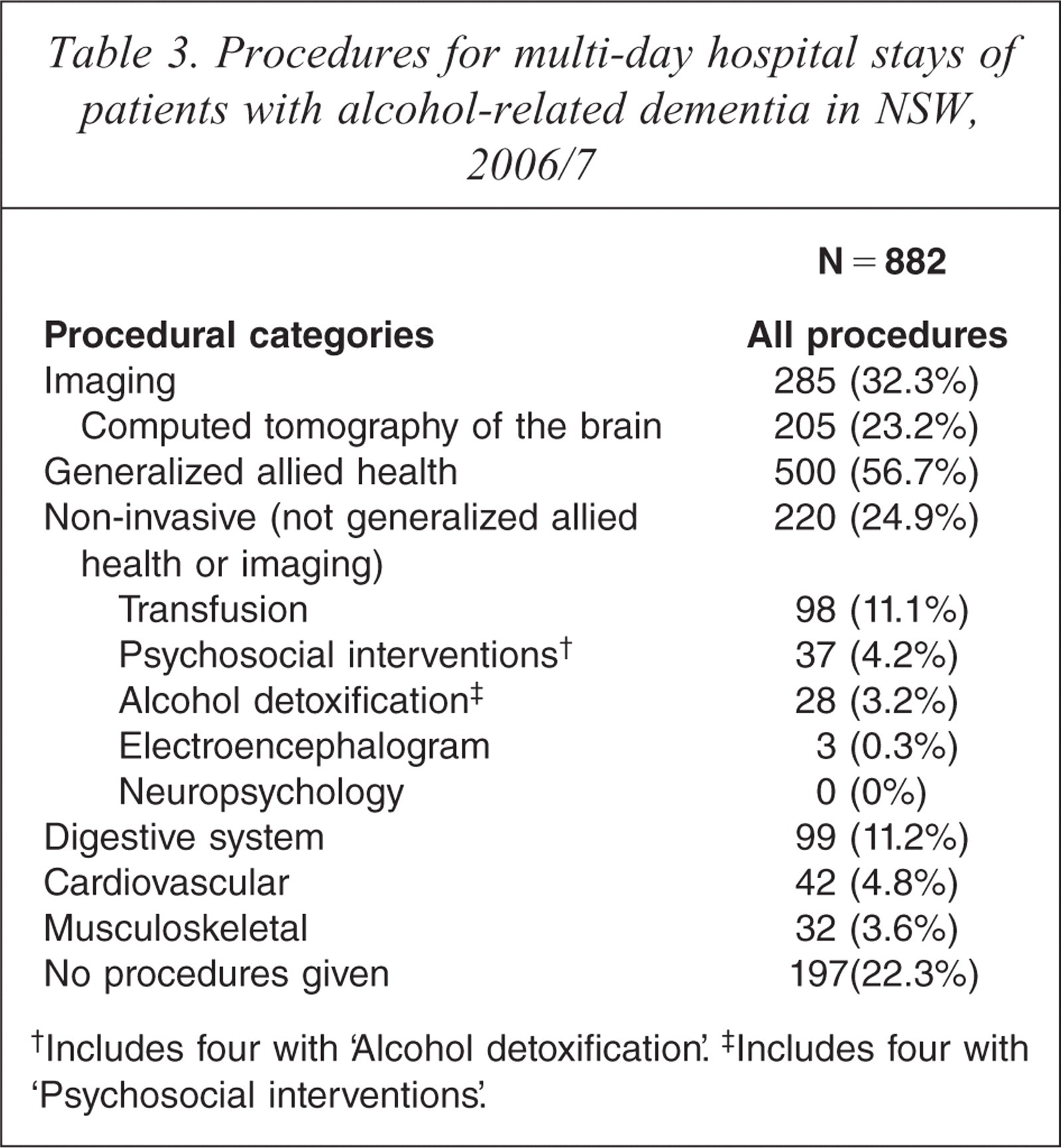
Includes four with ‘Alcohol detoxification’.
Includes four with ‘Psychosocial interventions’.
Outcomes for ARD patients
For the multi-day stays, the mean LOS was 15.0 days (median = 6). Reported discharge outcomes included transfer to nursing home for 7% of stays (n = 59), mortality of 5% (n = 45), discharge at own risk 3.7% (n = 33), transfer to other accommodation 2.8% (n = 25), with the majority (80%, n = 707) returning to their usual residence (which could be their nursing home).
For cases where there was a readmission, the one day readmission rate varied little with age and was similar to that for all dementia patients and patients without dementia: 11% compared with between 10% and 12% for patients aged under 85 both with and without dementia. However, 64% of discharges were followed by readmission within 13 weeks. This was largely (but not solely) an age effect: at 68% the 3-month readmission rate for ARD patients aged under 65 was significantly higher than that for those aged 65 to 74 (58%; chi square 5.22, p < 0.05). It was also high when compared with stays for all dementia patients aged less than 65 (55%), and higher again than the 29% for non-dementia patients aged under 65.
ARD patients compared with other dementia patients
We compared patients with ARD with all 20 793 patients with a dementia diagnosis. Those with ARD were younger and more likely to be men than other dementia diagnoses (3.7% of all dementia patients were aged 50–64, with mean age = 82.7 years, 40% male) [7]. For principal diagnoses, ARD patients had relatively high rates of epilepsy and liver disease and low rates of fractured femurs and strokes than other dementia patients.
Young ARD patients compared with young dementia patients (aged 50–64 years)
As more than half of the ARD patients were aged under 65, but only 3.7% of all dementia patients were aged 50–64, we compared young patients with ARD with all 759 patients in the study with dementia aged 50–64. ARD patients aged 50–64 accounted for 22% of the young dementia patients. Those with ARD were more likely to be men than younger patients in general with a dementia diagnosis (62% male). For principal diagnoses, ARD patients had relatively high rates of digestive diseases and lower rates of respiratory conditions, ill-defined conditions, UTIs and nervous system disorders when compared with all young dementia patients [7].
While young ARD patients had a shorter mean LOS than young dementia patients (mean of 14.3 days versus 20.7 days) the median stay was only slightly lower (5 versus 6 days) showing that ARD patients were less likely to have very long stays. Like other dementia patients, LOS for ARD patients tended to be longer than for non-dementia patients (mean = 7.1 days, median = 3 for non-dementia patients aged 50–64). At 3.7%, reported transfer to residential aged care was less than that for young dementia patients (8%) but higher than among non-dementia patients (0.4% for the 50–64 group). Also, ARD and young dementia patients had similar rates of discharge at own risk (3.7% and 2.8%, respectively; not statistically significant at 95% level) – both higher than that for non-dementia patients aged 50–64 years (1.4%). Mortality was not statistically different from that for young dementia patients, or from that for young non-dementia patients (following 3.6%, 4.7% and 2.3% of admissions, respectively). Note, however, mortality was significantly higher among all younger patients with dementia than among those without dementia.
Discussion
To our knowledge, this is the first study to document the prevalence, comorbidities and outcomes of diagnosed alcohol-related cognitive disorders in Australian hospitals. Overall 0.2% of patients discharged from NSW hospitals in 2006/7 were diagnosed with either ARD, amnesic disorder due to alcohol, or Wernicke's encephalopathy, while ARD represented 1.4% of 2006/2007 patients diagnosed with dementia. We have previously estimated that approximately 25% of individuals with dementia in NSW had a multi-day stay in hospital in that period and if that estimate holds true for ARD, which may not be the case, then it would mean that there were approximately 1200 persons with ARD in NSW in 2006/2007 and approximately 3500 Australia-wide [7,11]. As ARD is both preventable and potentially reversible, this represents a considerable public health concern [2,12].
ARD patients have a different profile from other dementia patients; they are younger and more likely to be men [7]. Indeed, ARD represents approximately 20% of the patients diagnosed with dementia in the 50–64 year old age bracket. This profile is not surprising but indicates that, as with other cases of early-onset dementia, there are likely to be considerable psychosocial consequences related to family function, employment and accommodation [13]. In an examination of early-onset dementia in Sydney a number of ARD cases were found to be homeless [5]. These factors undoubtedly contribute to a number of the outcomes noted when compared to people without dementia – the longer LOS, higher transfer rates to residential aged care and high rates of discharge at own risk – as well as the prominent use of allied health, which includes social work.
The overlaps noted between ARD, other dementias, Wernicke's encephalopathy, and amnesic syndrome due to alcohol is not surprising given the debate in the literature about the nosology of alcohol-related cognitive disorders [2]. A review of alcohol-related dementia and the clinical spectrum of Wernicke-Korsakoff syndrome discussed the overlap of the disorders both clinically and in neuropathological findings and provided good rationale for these observations [3]. It should be noted, however, that because this study has linked separate hospital admissions over a period of a year, that it is possible that some individuals initially presenting with an amnesic syndrome or Wernicke's encephalopathy might on a later separate admission be diagnosed with ARD or another type of dementia due to a worsening of cognition. The comparisons of the ARD with mixed diagnosis group with the rest of the ARD patients showed that they tended to be older, were more likely to present in acute alcohol intoxication or psychosis, and were less likely to have liver disease or epilepsy. Perhaps the nature of the acute presentation was initially misleading to clinicians when they made their initial dementia diagnosis.
Approximately a quarter of the admissions of patients with ARD were principally for a mental or behavioural disorder, although dementia itself was the principal reason in only about 6% of cases. In a similar fashion to dementia patients in general, ARD patients are most frequently admitted due to physical health problems, and common reasons for admission included liver disease, injuries (head injuries and fractures), infections (UTIs, lower respiratory, septicaemia) and epilepsy [7]. Perhaps not unexpectedly, about a third of the ARD admissions were diagnosed with liver disease, and this comorbidity distinguished them from other dementia patients.
It is difficult to determine from the data set how well-managed ARD is in the hospital system. The proportion that was assessed by drug and alcohol, geriatric or mental health services is not known and nor is the use of pharmacotherapeutic interventions including thiamine. Fortunately there was a high utilization of allied health services including social work, physiotherapy, occupational therapy and psychology. We also have no information about post-discharge treatment arrangements. Of concern, only 3% of admissions had formal alcohol detoxification and no admissions had a neuropsychological assessment, although in most cases that would be appropriate as this should be deferred until several weeks of abstinence [14]. Australian guidelines for the treatment of alcohol problems have specific sections that outline recommendations for assessment and management of cognitive disorders in this population but lack guidance about what services should be involved [14]. Undoubtedly as with other dual diagnosis populations, ARD patients are likely to benefit from input from a combination of services such as specialist drug and alcohol services and dementia services, but how often this happens is unknown. The development of clinical pathways to facilitate partnerships between services to address these issues would improve clinical care. At present the absence of such partnerships and pathways coupled with the stigma these patients often bear undermines adequate service delivery.
There has not been much interface between research focusing on other types of dementia and that involving ARD. Future research needs to prospectively assess patients identified with alcohol-related cognitive disorders and then include long-term follow up of cognitive and functional outcomes and their predictors using contemporary diagnostic criteria for cognitive impairment and dementia.
There are a number of limitations to this study. The NSW Admitted Patient Care Database is derived from data obtained from numerous clinicians making diagnoses and hence their validity is variable. In particular, the overlap noted between ARD, amnesic syndrome due to alcohol, and Wernicke's encephalopathy may in part reflect the different clinical viewpoints about the nosology of cognitive disorders in this population. The accuracy of coding of diagnoses and data entry by medical record staff is also unknown. There have been no published Australian studies that address this issue. It is likely that dementia is underestimated in this population due to a combination of poor recognition by medical staff, deficiencies in the medical record, and the requirement that to be recorded in the hospital admission data the medical diagnosis has to be deemed to contribute to the cost of the hospital stay. It is also possible that, in this study, patients that had multiple or longer stays were more likely to be identified as having dementia than patients with short or single admissions, and this might exaggerate the effect of dementia. These two factors have opposing effects; however, it is not currently possible to measure their impact on estimates. The age cut-off of 50 years is likely to have missed some patients with ARD as the onset of this disorder can occur at a younger age. Nevertheless, this is the largest ARD in hospital study in Australia.
There are also important strengths to the dataset. The database covers the whole population of admitted multi-day public hospital patients aged 50 years and over in NSW, the most populous state of Australia. In addition, all hospital stays for these people are included (public and private, multi-day and single day) allowing comprehensive analysis of their hospital experience. Further, the data linkage which allows patients to be tracked from initial admission to final discharge from hospital, allowing for movement both within and between hospitals and identification of readmissions is a major advance on earlier analyses.
In conclusion, these data suggest that ARD is responsible for considerable morbidity in the Australian community, particularly among those with early-onset dementia. More investigation of approaches to prevention, identification, assessment and management are required.
Acknowledgements
The authors thank the New South Wales Department of Health for permission to use data from the Admitted Patient Data Collection and for provision of the data extract with patient identifiers derived by the Centre for Health Record Linkage (or CHeReL). We thank the other members of the Hospital Dementia Services project team, Gail Brien, Le Anh Pham Lobb and Charles Hudson, for their work on the project and assistance with this paper and the Australian Institute for Health and Welfare for hosting and supporting the project.