
Abstract
The declining interest in psychiatry as a subspecialty of medicine is an ongoing concern that has prompted many studies in recent years to examine determinants of career choice for medical students and junior doctors [1–8]. Some studies have correlated personality traits with career preferences in an attempt to profile characteristics of medical students that might contribute to career trajectories [9–11]. The majority of these studies sought to identify future psychiatrists, and interpret analyses to encourage those interested and suited to the profession to consider psychiatry as a career option.
One study [12] suggested that psychiatrists are more likely to have ‘open’ and ‘agreeable’ personalities, and are viewed as being imaginative, curious, sympathetic and trusting. Openness refers to attentiveness to one's inner feelings, the possession of intellectual curiosity, and an independence of judgement. Men and women who score high on openness experience deeper and more differentiated emotional states, and feel both happiness and sadness more intensely than others. They are more imaginative, and are receptive to new experiences and change. Conversely, those who score low on openness tend to be conventional in behaviour and conservative in outlook. They prefer the familiar to the novel, and their emotional responses are somewhat blunted, as they do not believe that feeling states are of much importance. Agreeableness refers to those who are fundamentally altruistic, thereby sympathetic to others and eager to help them. Lifestyle factors and perceptions of what a medical career entails are also important, and are perhaps increasing in influencing career choice. However, to what extent each of these determinants plays a role, and more explicitly, how and when they exert an effect, remains unknown.
In terms of medical student personality styles, openness to experience and agreeableness have correlated significantly with positive attitudes towards psychiatry [11]. Positive personal experiences of psychiatry whilst training as a medical student and as an intern, or exposure to psychiatrist leaders, have been held to orientate doctors towards this career choice [11,13,14], though it has been suggested that psychiatry is a last resort career [8]. Interestingly, it has also been suggested that having a scientific background engenders a positive view of psychiatry [5,11].
Aims
In an ever-challenging climate in which there is a dearth of psychiatrists to perform the full range of critical clinical, administrative and academic functions, we sought to characterise medical students most likely to choose psychiatry as a career, and ascertain those aspects of the specialty most likely to attract potential recruits, seeking to both identify factors contributing to its attractiveness, and conversely, potential misperceptions that might contribute to its poor desirability.
Method
Participants and materials
Over three successive years, 580 students in the second year of a six-year undergraduate medical program at the University of New South Wales, Australia were administered a questionnaire based on that developed for a North American study [15]. The questionnaire was administered at the beginning of the first semester as part of an introductory lecture. Participation was voluntary and respondents remained anonymous. Permission to administer the questionnaire was granted by the Dean of the medical school.
The questionnaire collected demographic information (age entering medical school, gender, ethnicity, religious affiliation, size of the community from where the students originated), and data that focused on specialty choice. Specifically explored were:
The degree to which students were considering careers in the specialties of internal medicine, surgery, psychiatry, paediatrics, general practice and obstetrics/gynaecology. The students were asked to indicate the likelihood of choosing a career in each specialty on a five-point rating scale (1 = ‘chosen career’, 2 = ‘strong possibility’, 3 = ‘no strong opinion yet’, 4 = ‘unlikely’, 5 = ‘no way’). The ratings for each specialty were not mutually exclusive and students could, for example, rate ‘strong possibility’ to more than one specialty.
The generic factors students considered important, namely, ‘lifestyle’, ‘prestige’, ‘ability’, ‘financial reward’, ‘interesting/challenging work’ and ‘ability to help people’ were rated using a five-point scale (1 = ‘very important’, 2 = ‘important’, 3 = ‘somewhat important’, 4 = ‘of very little importance’, 5 = ‘not important’).
The degree to which students perceived each specialty as attractive according to ‘financial reward’, ‘lifestyle’, ‘job satisfaction’, ‘interesting subject matter’, ‘intellectually challenging’, ‘prestige within the medical community’, ‘degree to which patients are helped effectively’, ‘degree to which the specialty draws upon aspects of medical training’, ‘rapidly advancing understanding and treatments’, ‘bright and interesting future for the field’, ‘based upon reliable scientific foundation’, ‘enjoyable work’, and ‘association with other physicians in that specialty’. The ratings were also made on a five-point scale (1 = ‘very attractive’, 2 = ‘attractive’, 3 = ‘neutral’, 4 = ‘not attractive’, 5 = ‘extremely unattractive’).
In addition, the questionnaire incorporated the 60-item NEO Five-Factor Inventory (NEO-FFI) [16], which measured each student's scores on the five personality factors of Neuroticism (N), Extraversion (E), Openness (O), Agreeableness (A) and Conscientiousness (C).
Data analysis
The collated data were entered into SPSS Windows Version 16 (Chicago, IL, USA) and analysed in several ways. Scores derived from the NEO-FFI were screened for normality, homoscedasticity and linearity of the residuals, multicollinearity, independence of errors, and univariate and multivariate outliers. Data from any students identified as univariate or multivariate outliers were deleted from subsequent analyses. Parametric tests were performed when the dependent variable consisted of continuous scores (e.g., age, the five personality factors), and non-parametric tests were performed when the dependent variable consisted of categorical scores (e.g., choice of specialty, ratings of importance/attractiveness on individual lifestyle and other factors known to influence choice of medical specialty). Possible associations of age and gender to personality and other variables were explored using a variety of techniques: (i) One-Way Analysis of Variance (ANOVA) was performed to examine differences between men and women on the five personality factors; (ii) the Mann-Whitney U-test was performed to examine differences between men and women according to choice of medical specialty and importance on the six generic factors pertaining to ‘lifestyle’, ‘prestige’, ‘ability’, ‘financial reward’, ‘interesting/challenging work’ and ‘ability to help people’; (iii) One-Way ANOVA was performed to examine any differences in age according to choice of medical specialty and importance on the six generic factors, and any correlations between age and personality scores were explored with the Pearson product-moment correlation coefficient. One-Way Multivariate Analysis of Covariance (MANCOVA) was performed to determine which personality factors were associated with likelihood of choosing a career in each medical specialty. Where required, age and gender were controlled. Finally, Friedman's ANOVA was performed to examine differences in ratings of attractiveness across all medical specialties according to the 13 factors listed in ‘Participants and materials’ above. Where significant results were found, post-hoc contrasts were examined using the Wilcoxon's signed-rank test. Bonferroni corrections were applied to control for multiple comparisons.
Results
Characteristics of the sample
Of the 580 students who completed the questionnaire, seven (1.2%) were identified as univariate and multivariate outliers based on their NEO-FFI scores, and their data were excluded from subsequent analyses, leaving 573 participants. The group comprised 267 men (46.6%) and 304 women (53.1%). Two students (0.3%) did not indicate their gender.
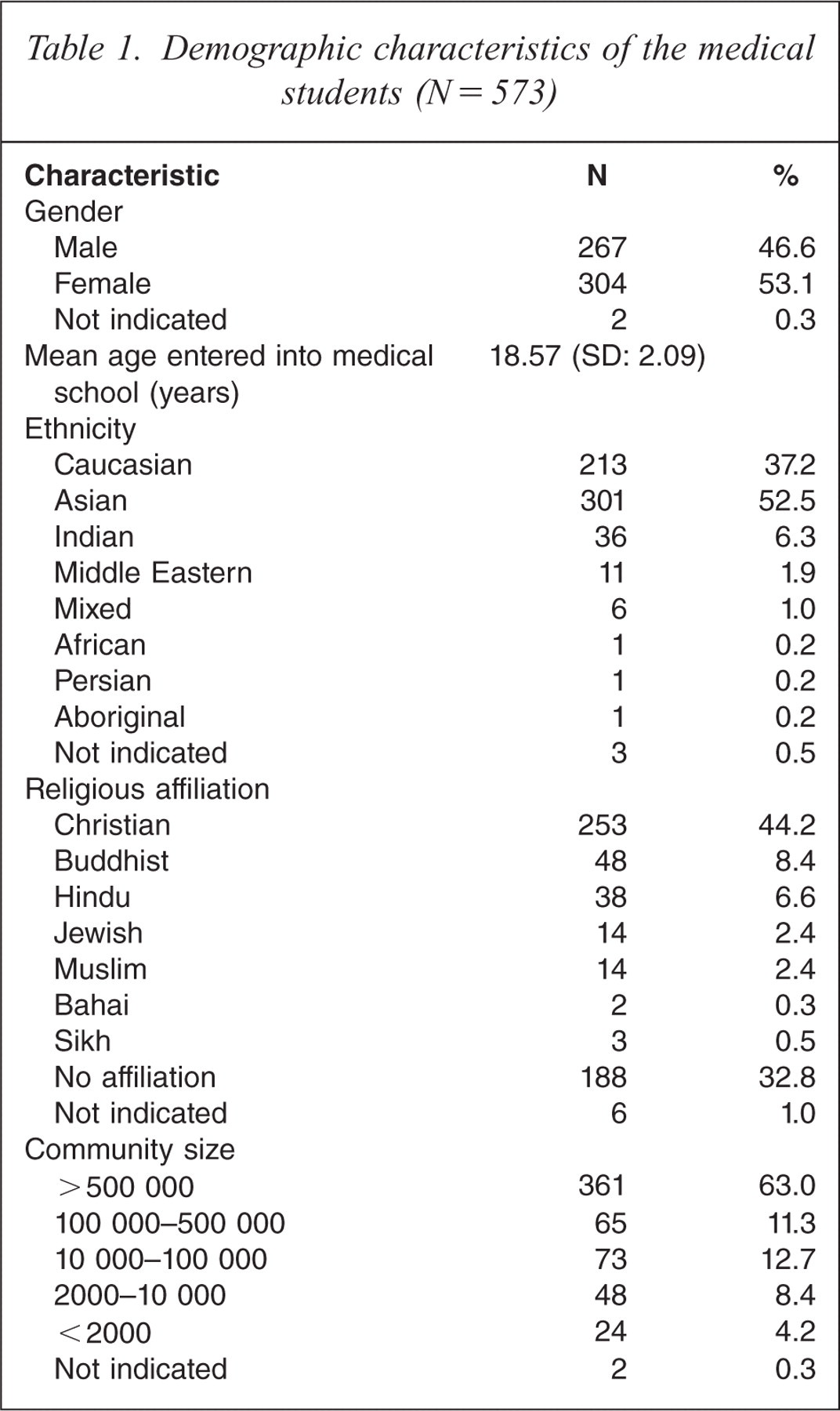
Table 1 details demographic characteristics of the sample. The mean age of entry into medical school was 18.57 years (SD = 2.09), and the proportions of men and women were similar. The majority of students were of Asian and Caucasian background, of Christian or no religious affiliation, and from cities where the population exceeded 500 000.
Demographic characteristics of the medical students (N = 573)
Choice of medical specialty
Figure 1 illustrates the percentages of students indicating their preferences for each of the six specialties. When examining the actual numbers of students who indicated ‘chosen career’ or ‘strong possibility’, the order of preference for the different specialties were internal medicine (n = 290), surgery (n = 281), paediatrics (n = 261), general practice (n = 214), obstetrics/gynaecology (n = 107) and psychiatry (n = 86).
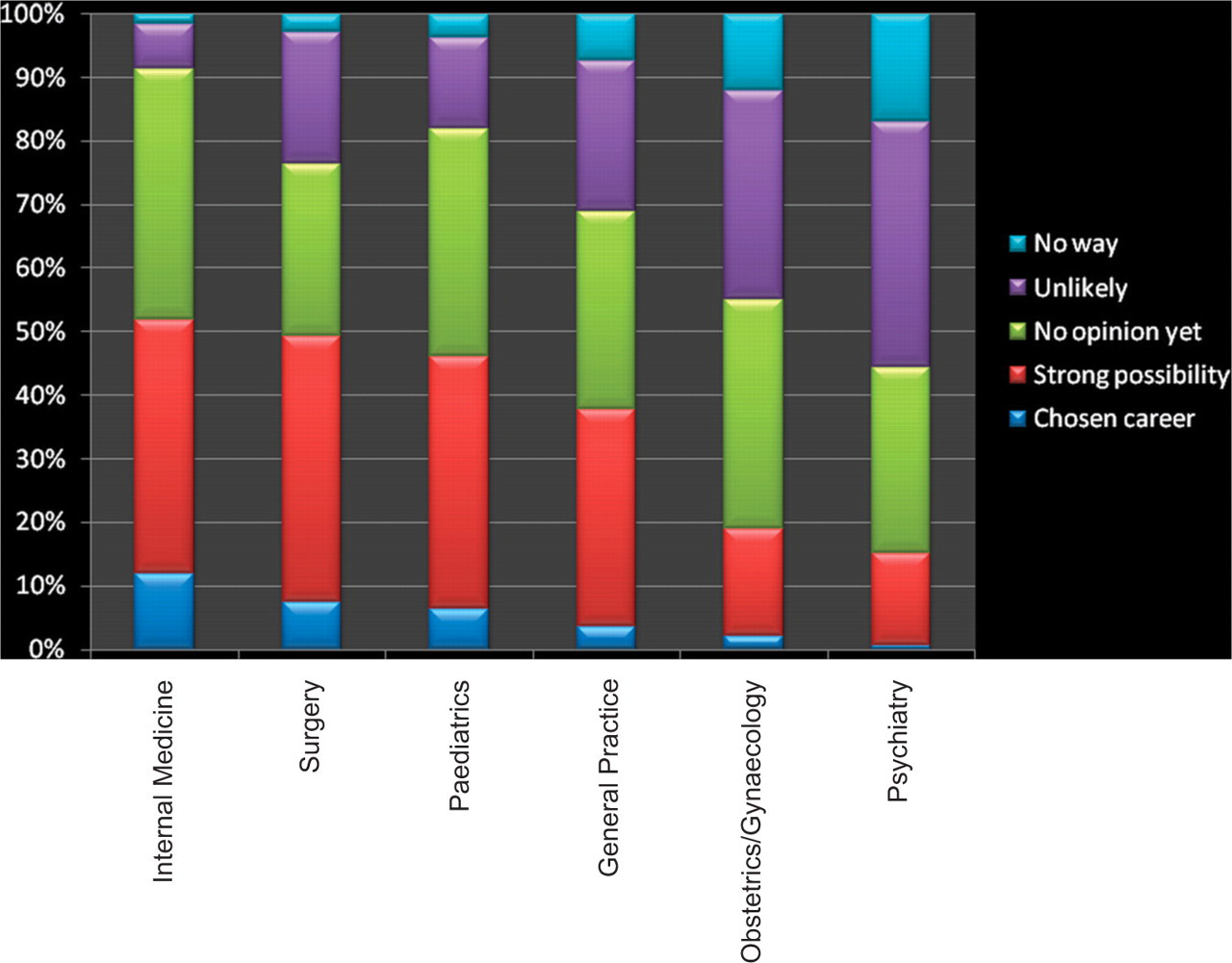
Degree to which first year medical students considered careers in various specialties
Age and gender
Choice of medical specialty
Men rated a career in surgery as significantly more likely than did women (U = 26859.00, p < 0.001, r = −0.31). Women indicated significantly higher preferences than men for a career in obstetrics/gynaecology (U = 28496.5, p < 0.001, r = −0.26), paediatrics (U = 35512.00, p = 0.021, r = −0.10), and general practice (U = 33650.50, p = 0.001, r = −0.14). There were no significant differences between men and women in preference ratings for internal medicine and psychiatry (p > 0.05).
Those who indicated ‘chosen career’ or ‘strong possibility’ for the specialty of obstetrics/gynaecology were significantly older (M = 19.07 years, SD = 2.99) than those who indicated ‘unlikely’ or ‘no way’ (M = 18.45 years, SD = 1.81); [F2,564 = 3.73, p = 0.025]. There were no significant differences in age between those who did or did not indicate a preference for choosing a career in internal medicine, surgery, psychiatry, paediatrics and general practice (p > 0.05).
Personality scores
Women had significantly higher scores than men on the factors of Neuroticism (females: M = 21.53, SD = 7.34); males: M = 19.46, SD = 7.69, F1,570 = 10.79, p = 0.001), Openness (females: M = 30.68, SD = 5.56; males: M = 29.60, SD = 5.74, F1,570 = 5.26, p = 0.02) and Agreeableness (females: M = 33.08, SD = 5.12; males: M = 30.68, SD = 5.47, F1,570 = 29.34, p < 0.001). There were no significant differences between men and women on scores for Extraversion and Conscientiousness (p > 0.05).
There were no significant correlations between age and scores on each of the personality factors (p > 0.05), presumably reflecting the narrow age range of the sample.
Importance on generic factors
Men rated ‘prestige’ (U = 31038.00, p < 0.001, r = −0.20) and ‘financial reward’ (U = 32584.00, p < 0.001, r = −0.17) as significantly more important than did women in directing their choice of specialty. Compared to men, women rated ‘ability to help people’ as significantly more important in choosing a specialty (U = 35088.00, p = 0.002, r = −0.13). There were no significant differences between men and women in ratings of the importance of ‘lifestyle’, ‘ability’ and ‘interesting/challenging work’ in directing future specialty choice, nor were students' rating of the importance of the generic factors affected by age (p > 0.05).
Personality factors and choice of medical specialty
One-Way MANCOVA was performed to examine associations between personality factors and students' anticipated choice of a career in each specialty. The degree of likelihood of making a particular specialty choice was originally rated across five categories, but because of small numbers in some categories, the data were collapsed into three categories and renamed for clarity. ‘
Personality scores relating to each specialty are detailed in Table 2.
Personality scores for each medical specialty stratified by likelihood of choosing a career in that specialty
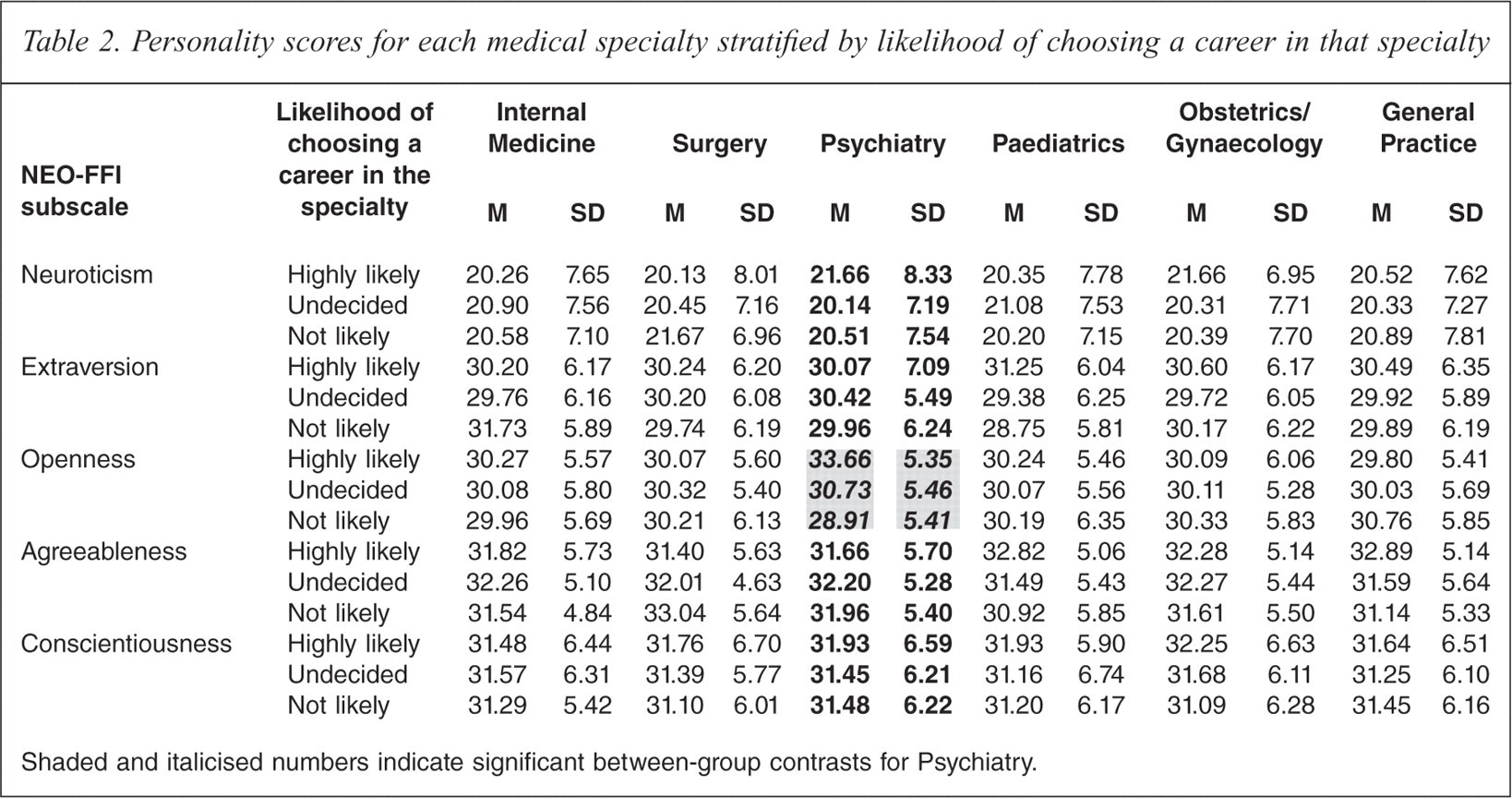
Shaded and italicised numbers indicate significant between-group contrasts for Psychiatry.
Psychiatry
There was an overall significant difference across the five personality factors between those who indicated ‘highly likely’, ‘undecided’ and ‘not likely’ for psychiatry (Wilks λ = 0.90; F10,1118 = 5.83, p < 0.001). Tests of between-subjects effects showed a significant main effect for Openness (F2,563 = 27.35, p < 0.0001). Post-hoc tests showed that those who rated psychiatry ‘highly likely’ had significantly higher Openness scores (M = 33.66, SD = 5.35) than those who indicated ‘undecided’ to psychiatry (M = 30.73, SD = 5.46) (t249 = 4.06, p < 0.0001); and those who indicated ‘undecided’ to psychiatry had significantly higher Openness scores than those who rated psychiatry ‘not likely’ (M = 28.91, SD = 5.41) (t478 = 3.50, p = 0.001). There were no significant main effects for Neuroticism, Extraversion, Agreeableness or Conscientiousness (p > 0.05).
Other specialties
There were no significant differences in scores across the five personality factors between those who indicated ‘highly likely’, ‘undecided’ and ‘not likely’ for internal medicine, surgery, obstetrics/gynaecology and general practice (p > 0.05). In respect of paediatrics, there was an overall significant difference across the five personality factors between those who indicated ‘highly likely, ‘undecided’ and ‘not likely’ (Wilks λ = 0.954; F10,1114 = 2.65, p = 0.003). Tests of between-subjects effects showed a significant main effect for Extraversion (F2,561 = 8.58, p < 0.0001) and Agreeableness (F2,561 = 4.68, p = 0.01). Those who indicated ‘highly likely’ had significantly higher Extraversion scores (M = 31.22, SD = 6.05) than those who indicated ‘undecided’(M = 29.38, SD = 6.25) (t462 = 3.20, p = 0.001) and ‘not likely’ (M = 28.75, SD = 5.81) (t361 = 3.55, p < = 0.0001). Further, those who indicated ‘highly likely’ to paediatrics had significantly higher Agreeableness scores (M = 32.82, SD = 5.06) than those who indicated ‘undecided’ (M = 31.49, SD = 5.43) (t462 = 2.69, p = 0.008) and ‘not likely’ (M = 30.92, SD = 5.85) (t361 = 3.04, p = 0.003).
Ratings of attractiveness of career aspects for all medical specialties
Friedman's ANOVA was performed to determine whether there was an overall significant difference in ratings of attractiveness between the six medical specialties for each career variable. Where significant results were obtained, the Wilcoxon's signed rank test was performed to compare specialties against each other. The critical α level was set at 0.003 to adjust for 15 contrasts per career variable. Results of these multiple contrasts are represented in Figure 2.
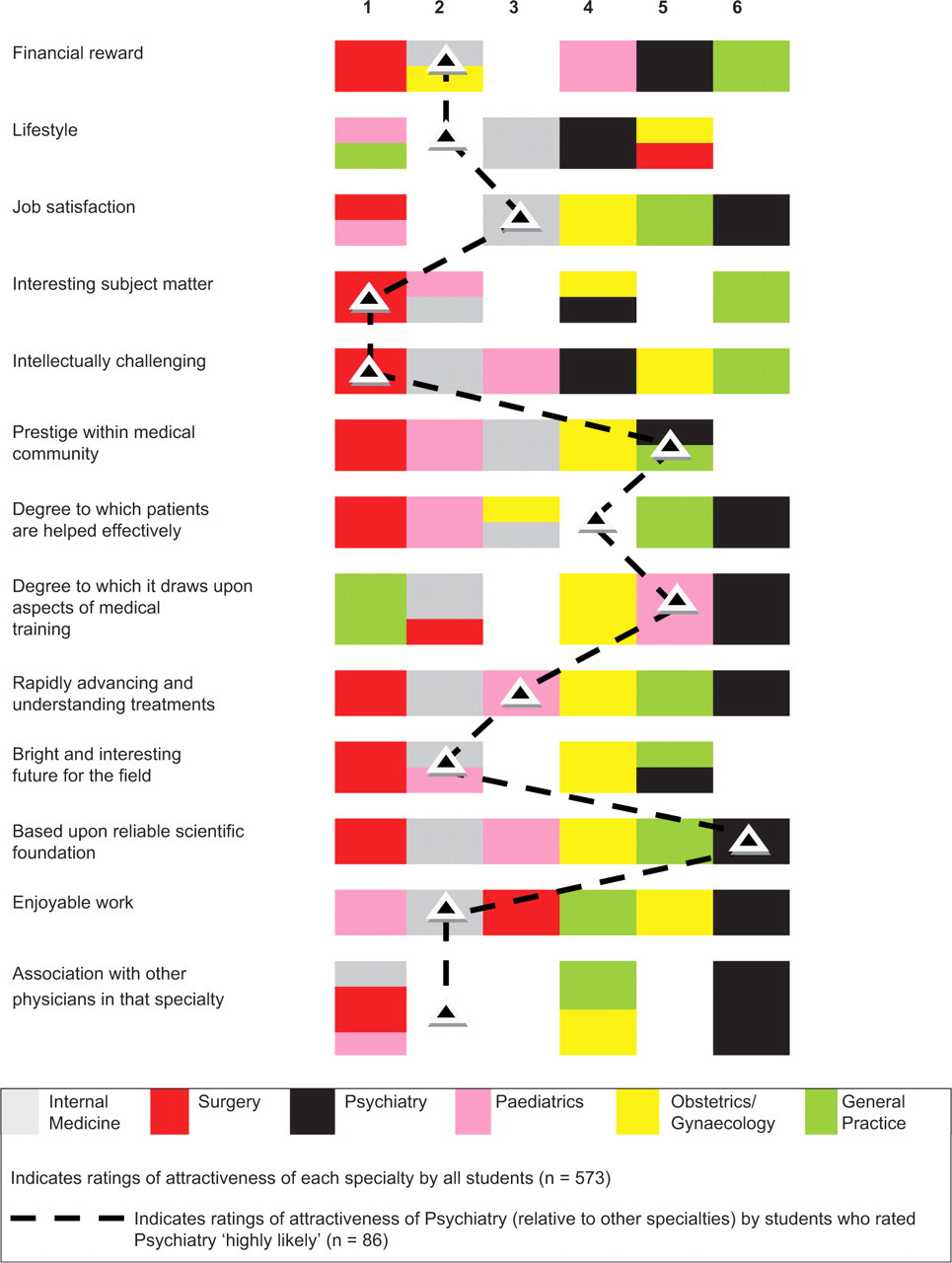
The degree of attractiveness of each medical specialty according to various career variables (1 = most attractive; 6 = least attractive)
The coloured blocks in Figure 2 illustrate how specialties fared against each other based on ratings of attractiveness according to the career variables. These results were based on ratings by all 573 medical students. For example, with respect to ‘financial reward’, surgery was rated most highly (first), followed by internal medicine and obstetrics/gynaecology (equal second), and paediatrics (fourth), with psychiatry ranking fifth, and general practice last.
As shown in Figure 2, surgery was rated most attractive according to the majority of variables (apart from ‘lifestyle’), followed by internal medicine and paediatrics. The least attractive specialties according to the majority of variables were obstetrics/gynaecology (third last), general practice (second last) and psychiatry (last).
In order to determine which career variables may draw students to the field of psychiatry (i.e., the career aspects important and not so important to those interested in this field), the analyses were repeated for those 86 students who indicated ‘highly likely’ to psychiatry. The results for these students are indicated by the dotted black line. Predictably, those interested in psychiatry ranked this specialty more highly on most career variables than did the sample of 573 students as a whole. Of note, psychiatry was ranked by the selected subset of students as most attractive with respect to ‘interesting subject matter’ and ‘intellectually challenging’ (both of which ranked above all other specialties), with relatively high ratings also for ‘financial reward’ (second to surgery and ranked equally to internal medicine, paediatrics and obstetrics/gynaecology), ‘lifestyle’ (second to general practice and ranked equally to paediatrics), ‘bright and interesting future for the field’ (second to surgery and ranked equally to internal medicine and paediatrics), ‘enjoyable work’ (second to paediatrics) and ‘association with other physicians in the specialty’ (second to paediatrics and ranked equally to internal medicine). Variables not rated attractive in the context of psychiatry as a career were ‘prestige within the medical community’, ‘degree to which patients are helped effectively’, ‘degree to which it draws upon aspects of medical training’, and the extent to which it is ‘based upon reliable scientific foundation’.
Discussion
Over the past five decades there has been a decrease internationally in the number of students interested in psychiatry, with a decline from 10% in the 1960s [17] to present-day rates of approximately 2 to 5% [2]. This is of significant concern in light of recent findings from the Australian 2007 National Survey of Mental Health and Wellbeing showing that almost half the population met criteria for a mental disorder at some time in their entire life, with one in five experiencing symptoms in the past 12 months [18]. A preponderance of intensive community-based mental health care being consumed by psychosis patients in particular means that a scarcity of resources is available to other individuals in need [19], and could in part reflect the increasing prevalence of self-management versus formal service use for common mental disorders [20]. Current service inadequacies are not solely a function of government funding, but also reflect the dearth of psychiatrists to perform critical clinical services.
Several studies have shown that students are aware at an early stage in medical school or during residency which specialty they want to pursue [21,22]. However, research examining career choice amongst medical students has established that the number of students considering a career in psychiatry increases after undergraduate teaching and training exposure to the specialty [11,23]. In this context, professional socialisation also impacts upon existing attitudes [24], but to what extent prior personality plays a role in career selection, and the precise nature of the motives that underpin specialty choice remains unknown [25].
In our study, psychiatry appealed to the fewest number of students. However, those who expressed a strong interest had significantly higher Openness scores on the NEO-FFI than those who indicated a lesser likelihood of pursuing the specialty. Consistent with our findings, previous studies have shown that openness to experience fosters more favourable attitudes towards psychiatry [11], and that those choosing psychiatry also have greater neuroticism [26], currently understood as a heightened emotional sensitivity and vulnerability to distress. The latter finding suggests a need to ensure that psychiatry training programs incorporate elements aimed towards promoting the emotional self-care and well-being of trainees.
Our study also revealed that those interested in psychiatry as a career were most influenced by perceptions that the field contains interesting subject matter and is intellectually challenging, and were less influenced by factors such as prestige within the medical community. These findings echo those of previous studies [27,28] in which medical students interested in psychiatry were not particularly concerned about recognition, but instead, considered the specialty as interesting and challenging. Therefore, in addition to individual characteristics such as personality, perceived attributes of a particular career and lifestyle factors are likely to be important in decisions about career specialty [29]. Indeed, when examining the actual contributions of variance to choice of psychiatry, the career variable ‘interesting and challenging subject matter’ accounted for 22.2%, whilst ‘Openness’ accounted for only 5.1%. Other studies have also found that personality traits and vocational interests make only a modest contribution, with the majority of variance remaining, puzzlingly, unaccounted for [30]. It is therefore likely that what students value has multiple determinants.
With respect to other career determinants influencing choice of psychiatry, those in our sample interested in psychiatry viewed the specialty relatively favourably with respect to financial reward and lifestyle, and perceived the field as making advances with respect to understanding and developing new treatments, such that it potentially has a bright and interesting future. Somewhat worrying, however, is the fact that even those interested in the specialty regard it as lacking both scientific foundation and prestige within the medical community views that have been identified previously [28]. Further, students' appraisal is that it does not help patients effectively. In part, this may be because it does not appear to draw upon aspects of medical training. Not surprisingly, these negative views resonate more broadly across all students, irrespective of their level of interest in psychiatry.
These negative views around psychiatry as lacking a scientific foundation, ineffective in helping people, and not holding prestige within the medical community are perhaps equally critical to specialty choice, as are the field's many positive attributes. Therefore, in order to enhance the likelihood of medical students choosing psychiatry as a career, in addition to promoting its attractions, misperceptions about the specialty need to be addressed [31]. Given that a large number of students remain undecided about their future specialty choices at this early stage of medical school, early efforts to correct misperceptions may be important.
Clinical rotations in psychiatry provide an opportune forum in which such misperceptions can be targeted, and in which positive experiences of psychiatry can be fostered through influential role models and mentoring. Research has demonstrated that changes in the likelihood of considering psychiatry as a career significantly increases in a positive direction following a clinical attachment for medical students, and the factors identified as most influential in persuading the students include quality of the teaching, enthusiasm of the clinical teachers, the holistic approach, and the scientific basis of psychiatry that is promoted [14]. The influence of such medical school experiences has been shown to foster similar positive attitudes towards psychiatry as well as various other medical specialties [11,32–34].
The reality is that psychiatry is interesting both theoretically and clinically. Few specialties in medicine afford such personal access to people's lives and perceptions of the world. The mind is by far the most complex and sophisticated ‘component’ of human beings, and understanding disorders of the mind is undoubtedly one of the greatest intellectual challenges facing mankind. Researchers dealing with the concepts of consciousness, self, and neuropsychology are working in fields that are at the frontiers of science, but remarkably these domains of psychiatry are seldom detailed in medical school prospectuses, or if they are mentioned, they are often not linked to psychiatry. As a consequence, it is perhaps understandable why psychiatry as a medical specialty is viewed as lacking prestige and a scientific foundation. Granted, in practice there is much to do, and almost all treatments in psychiatry remain largely symptomatic remedies as opposed to cures. However, the majority of patients managed by psychiatrists benefit significantly. This message is perhaps lost during medical training, and is insufficiently emphasised.
Limitations
In our sample, personality factors did not appear to be significantly associated with choice of medical specialty, except in the case of psychiatry, as discussed, and paediatrics, where those favouring the specialty had higher Extraversion and Agreeableness scores. One reason for the lack of association between personality and a number of the specialties may be the presence of confounding factors such as age and gender. For example, prior to the control of any confounds, a preference for surgery was associated with lower Neuroticism and Agreeableness scores. However, there was also a significant bias towards men expressing a preference for surgery, and once gender was controlled, any associations between personality factors and surgery disappeared. Similarly, a preference for general practice was associated with higher Agreeableness scores. However, there was a significant bias towards women expressing a preference for this specialty, and after gender was controlled, any associations between personality factors and general practice disappeared.
The current group under study were also young, and likely to have entered medical school soon after finishing high school. This may have resulted in a more homogeneous group than might be expected in a post-graduate medical course, and it would be of interest to replicate the current study in such a group. Finally, it has been argued that in relatively homogeneous groups, it may be necessary to study personality at the facet, or trait level, such as with use of the 240-item NEO-FFI, in order to identify differences. The NEO facet scales are independent subsets of items and thus provide additional explanatory variance [35].
Conclusions
The aims of this study were to characterise the personality profiles of those medical students who identified themselves as most likely to choose psychiatry as a career, to determine aspects of the specialty that attract potential recruits, and to pinpoint misperceptions that may dissuade students from pursuing it as a career. This study found that openness to experience was strongly associated with favouring psychiatry as a specialty choice; however, positive perceptions regarding its interesting and intellectually challenging subject matter was its most attractive attribute, and contributed a greater proportion to the variance than personality factors. These positive aspects of psychiatry that also extend to lifestyle and enjoyment were offset by misgivings regarding its putative scientific basis and mainstream role in medical training and lack of associated prestige. This is in keeping with the perceptions and stereotypes attributed to psychiatry, and correspond intuitively to the findings of previous reports [9,11,28]. There is growing concern that the psychiatric profession is failing to attract sufficient numbers of high-quality recruits [36], and therefore, if the decline of interest in the specialty is to be reversed, psychiatry needs to be better promoted using a two-pronged approach that not only highlights its many positive benefits and attributes, but also directly addresses the incorrect and biased views as to its scientific basis and professionalism. Clinical attachments that foster positive experiences and perceptions of psychiatry through influential role models and mentoring offer one means by which negative views can be corrected. Medical schools need to be mindful of any other opportunities that can be provided, as psychiatry does offer the lifestyle that many budding medical practitioners desire, and as a career both clinically and in research, it provides considerable intellectual stimulation. It is important therefore that we promote psychiatry throughout medical training and internships, and this is perhaps a role that some of our professional bodies could expand upon. If these positive messages can be conveyed, then perhaps more students can be persuaded to pick psychiatry.