
Abstract
Objectives
We aimed to assess the degree of stigmatizing attitudes and psychological distress amongst Australian medical students in order to better understand factors that may impact help-seeking behaviours of students. We hypothesize that sociodemographic factors will not significantly predict stigmatizing attitudes, and increasing levels of psychological distress will be associated with increasing stigma.
Methods
A cross-sectional online survey was distributed to medical students at Western Australian universities and members of the Australian Medical Students’ Association. Stigma was scored using the Mental Illness Clinicians’ Attitudes (MICA-2) scale. Psychological distress was assessed using the Hospital Anxiety and Depression Scale (HADS). Participants provided information about gender, age, spirituality, financial hardship, treatment for mental illness, and experience in psychiatry.
Results
There were 598 responses. The mean (Standard Deviation) MICA-2 score was 36.8 (7.5) out of a maximum of 96, and the mean (SD) HADS depression score was 4.7 (3.7). The mean (SD) HADS anxiety score was 9.3 (4.4). Past or current treatment for a mental illness was associated with lower MICA-2 scores. There was no association between MICA-2 and HADS scores, or sociodemographic factors.
Conclusions
Our results demonstrate relatively low MICA-2 scores and high HADS-A scores overall, with no association between HADS scores and stigma.
Stigma towards mental illnesses may be described as negative feelings or avoidance of a person based on their mental health status. 1 The conceptualization of stigma dates back to 1895, with Émile Durkheim’s characterization of stigma as a social phenomenon. 2 This was furthered by Corrigan’s four-stage model of self-stigma: perception of public stigma, natural agreement with public stigma, internalization of public stigma, and harm to self as a result of internal discordance between stigmatizing attitudes and the presence of the stigmatized trait. 3 This suggests that the formation of a stigmatizing attitude is unrelated to the presence of the stigmatized trait in an individual, which may explain why people with mental illnesses may still discriminate against other people with mental illnesses.
In 2013, an Australian study found high levels of stigma towards those with depression among medical students. 4 Stigma may also complicate help-seeking and exacerbate psychological distress,5,6 which is more prevalent in doctors and medical students than the general population. 7 Notably, a 2018 national Australian study found that up to 47.4% of medical students experienced subjective psychological distress. 8 Furthermore, moderate to high levels of stigma amongst medical students have been reported across national and international research.9–11 Investigating these issues, including stigma, is crucial as poor mental health has been associated with poorer academic performance, 12 lower levels of professionalism, 4 and increased medical errors. 13
This study was completed on behalf of the Australian Medical Student Association (AMSA), which is the peak representative body for medical students in Australia aiming to connect, inform, and advocate for the emerging medical workforce. Membership is voluntary. In 2021, AMSA’s national advocacy priority was to improve medical student mental health and well-being, including research into factors that influence poor mental health and attitudes to mental illness. Therefore, the primary aim of this study was to investigate the extent to which medical students display psychological distress and stigma towards mental illnesses as compared with the published literature.9–11 Secondary aims were to assess the association among stigma, sociodemographic, and psychological factors. We hypothesize that medical students will display varying levels of stigma, and sociodemographic factors will not significantly predict stigma levels. Due to the combination of internal discordance and reluctance to seek help, a secondary hypothesis is that increasing levels of psychological distress will be associated with increasing stigma.
Methods
Study design, ethics, participants, and procedure
A cross-sectional quantitative online survey was performed. Ethical approval for this study was obtained from [anonymized for peer-review]. Participation was voluntary, and informed consent was obtained prior to survey commencement. No identifiable data were collected. All students were enrolled in a medical degree at the University of Western Australia (UWA), Curtin University, and the University of Notre Dame Fremantle (n = 1602) or were registered members of AMSA (n = 3937 after excluding WA members). Invitations were distributed via an investigator-blind email. Three invitations 2 weeks apart were sent between July and September 2022.
Survey instrument
Stigma was assessed using the 16-item Mental Illness: Clinicians Attitudes-2 (MICA-2) scale, which has been validated among medical students with good internal consistency (Cronbach’s alpha: 0.79). 14 Possible scores range from 16 to 96. Higher scores indicate increasing stigma.
Psychological distress was assessed using the Hospital Anxiety and Depression Scale (HADS), a 14-item scale identifying anxiety/depressive symptoms. 15 Mean Cronbach’s Alphas of 0.83 and 0.82 for HADS-A and HADS-D, respectively, have been reported. 16 The efficacy of HADS has been reported as 0.73 and 0.91 for HADS-A and HADS-D, respectively. 17
Sociodemographic data including age, gender, year level, domestic versus international status, and previous psychiatry clinical placement experience were collected. Participants were asked if they had ever been treated for a mental illness, whether they considered religion/spirituality to be an important part of their life, their current living situation, and level of financial stress.
A copy of the questionnaire is provided in Appendix 1.
Statistical analysis
Data was managed and analyzed using SPSS v21 and GraphPad v8.0.0.18,19 MICA-2 scores were grouped into quartiles for analyses. The Chi-square test was used to compare the number of respondents in each quartile, the Kruskal–Wallis test compared MICA-2 scores between categorical groups, and the unpaired t test with Welch’s correction compared scores between dichotomous groups. WA and AMSA cohorts were compared using the same method. Volunteer bias was assessed using Continuum of Resistance Model. 20 Responses were divided into three groups as being from the first, second, or third email wave and compared using 1-way ANOVA for continuous variables and Chi-square test for dichotomous variables. Alpha was set at 5%, and all statistical tests were two-tailed.
Results
Participant demographics
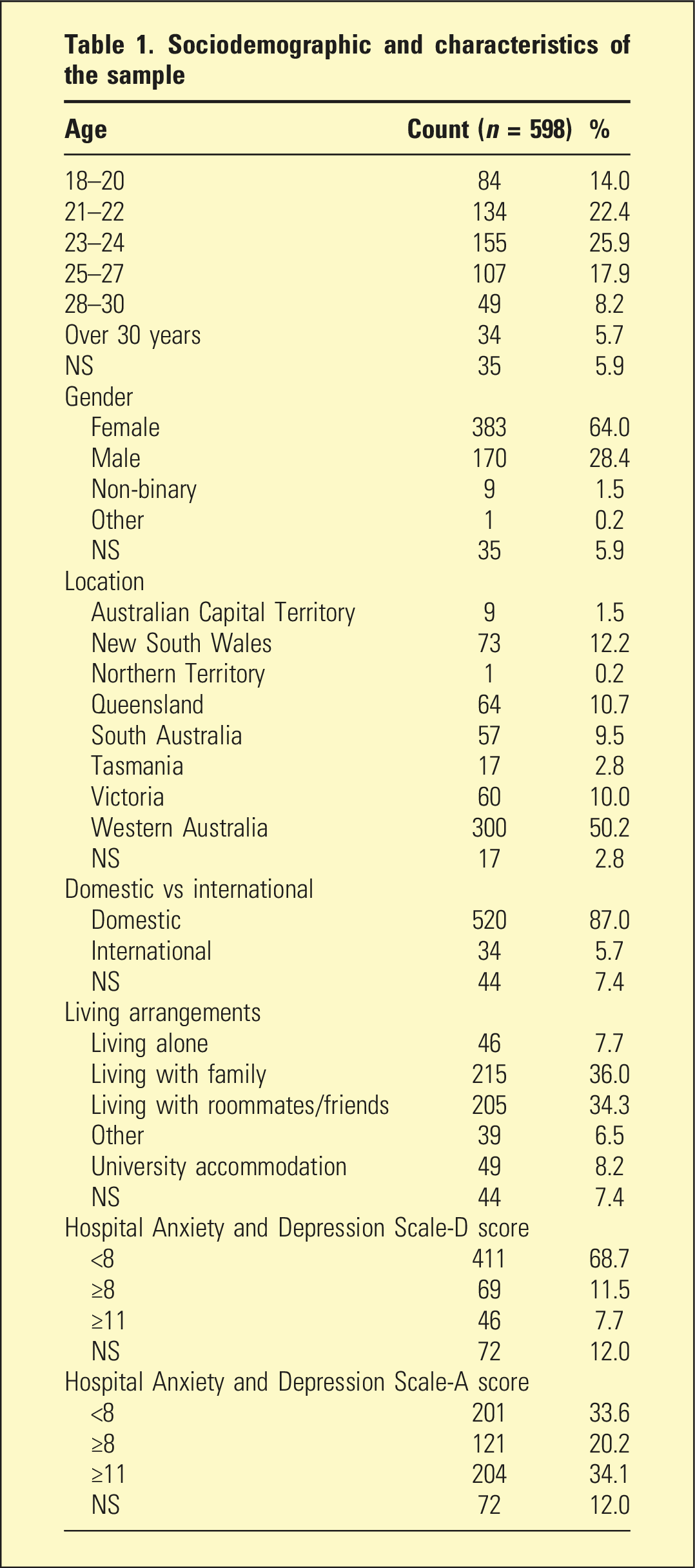
A total of 598 participants completed the survey, corresponding to a response fraction of 10.5% (Figure 1), with 318 recruited from AMSA’s mailing list and 280 from WA medical schools. Most participants were domestic students (n = 520, 87.0%), female (n = 383, 64.0%), aged 23–24 years (n = 155;25.9%), and living with family (n = 215, 36.0%) (Table 1). Flow chart of survey responses. Sociodemographic and characteristics of the sample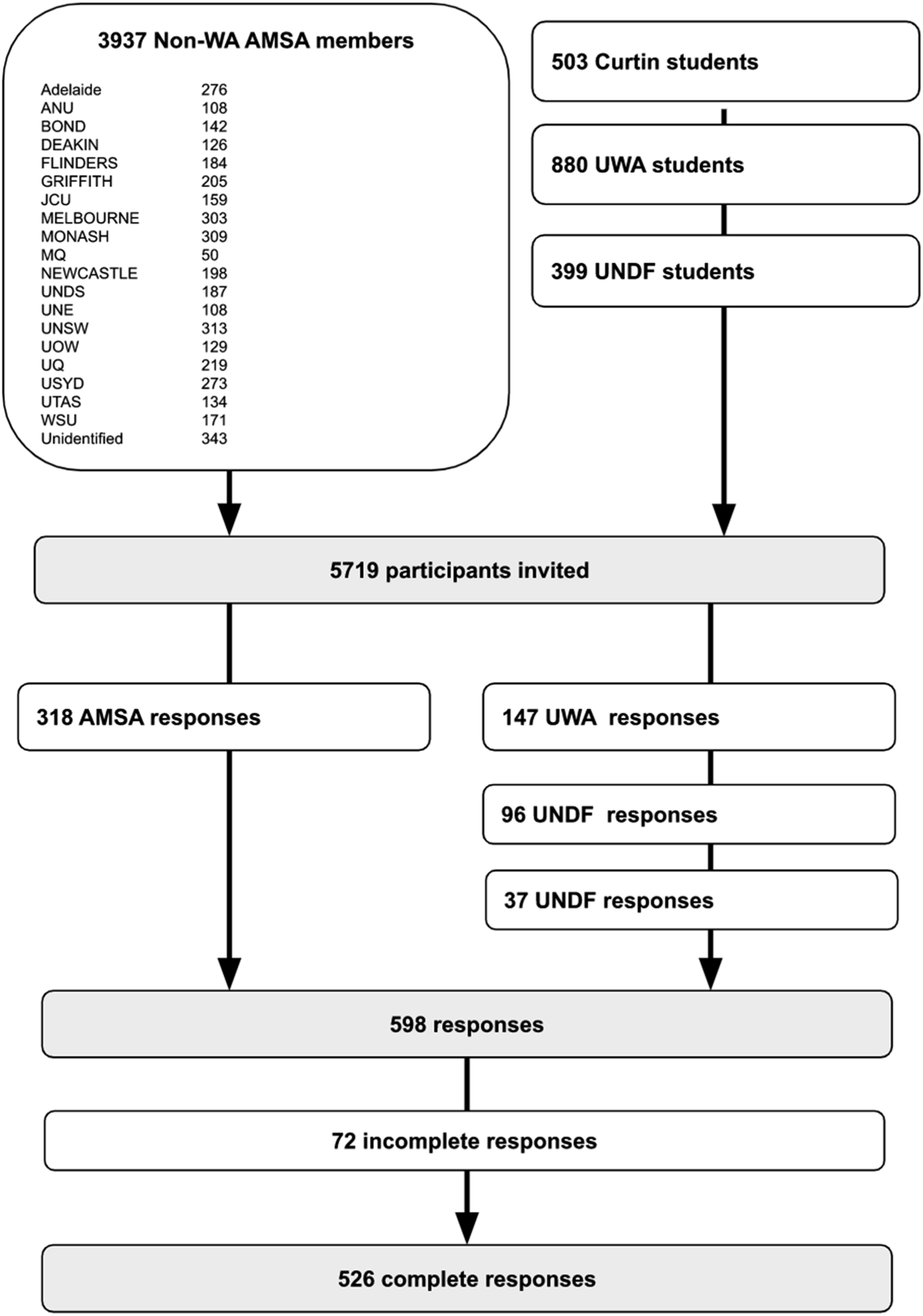
Participant non-response bias analysis a
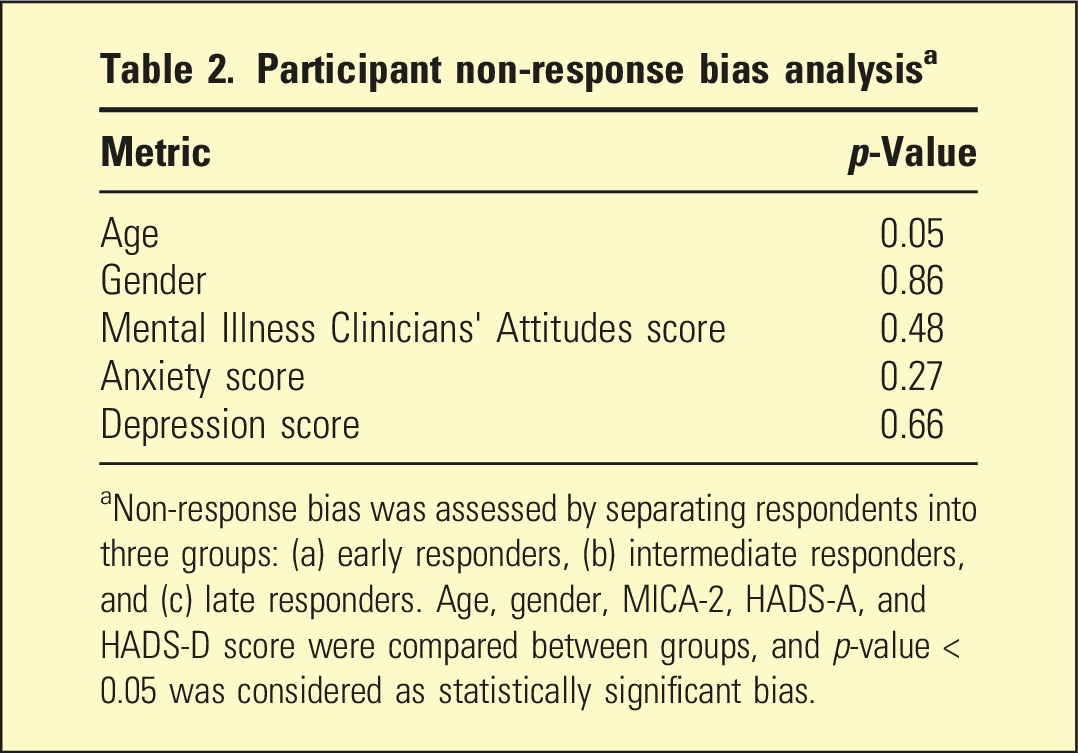
aNon-response bias was assessed by separating respondents into three groups: (a) early responders, (b) intermediate responders, and (c) late responders. Age, gender, MICA-2, HADS-A, and HADS-D score were compared between groups, and p-value < 0.05 was considered as statistically significant bias.
The WA cohort had a higher proportion of male respondents (36.3 vs 24.9%; p = 0.03). There was no statistically significant difference between WA and AMSA cohorts regarding HADS-A, HADS-D, MICA-2 score, previous psychiatry clerkship, domestic/international status, financial stress, and past/current psychological treatment.
Study measures
Sociodemographic measures and their association with stigmas a
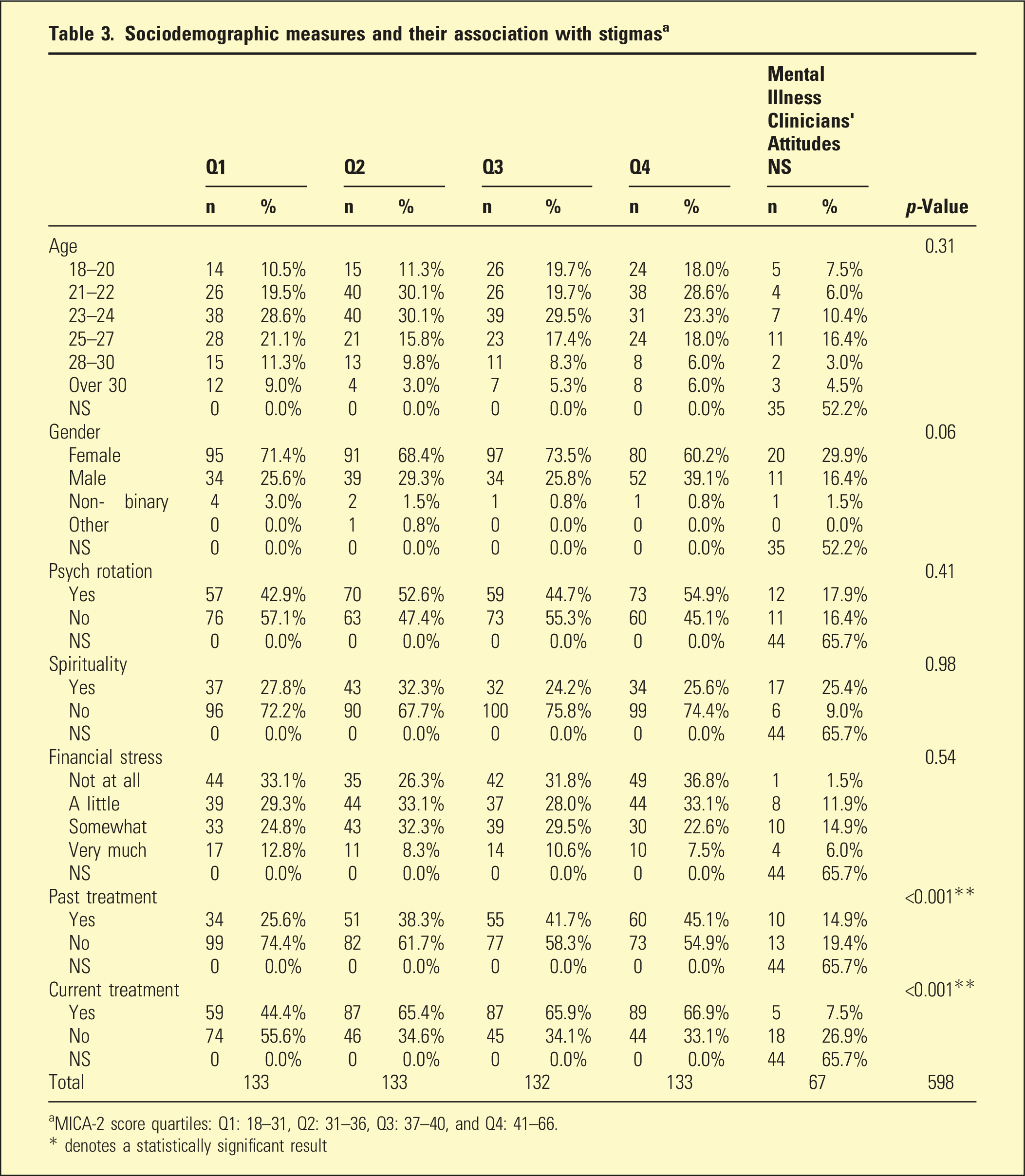
aMICA-2 score quartiles: Q1: 18–31, Q2: 31–36, Q3: 37–40, and Q4: 41–66.
* denotes a statistically significant result
Correlation among MICA-2 score, HADS-D score, HADS-A score, and sociodemographic factors
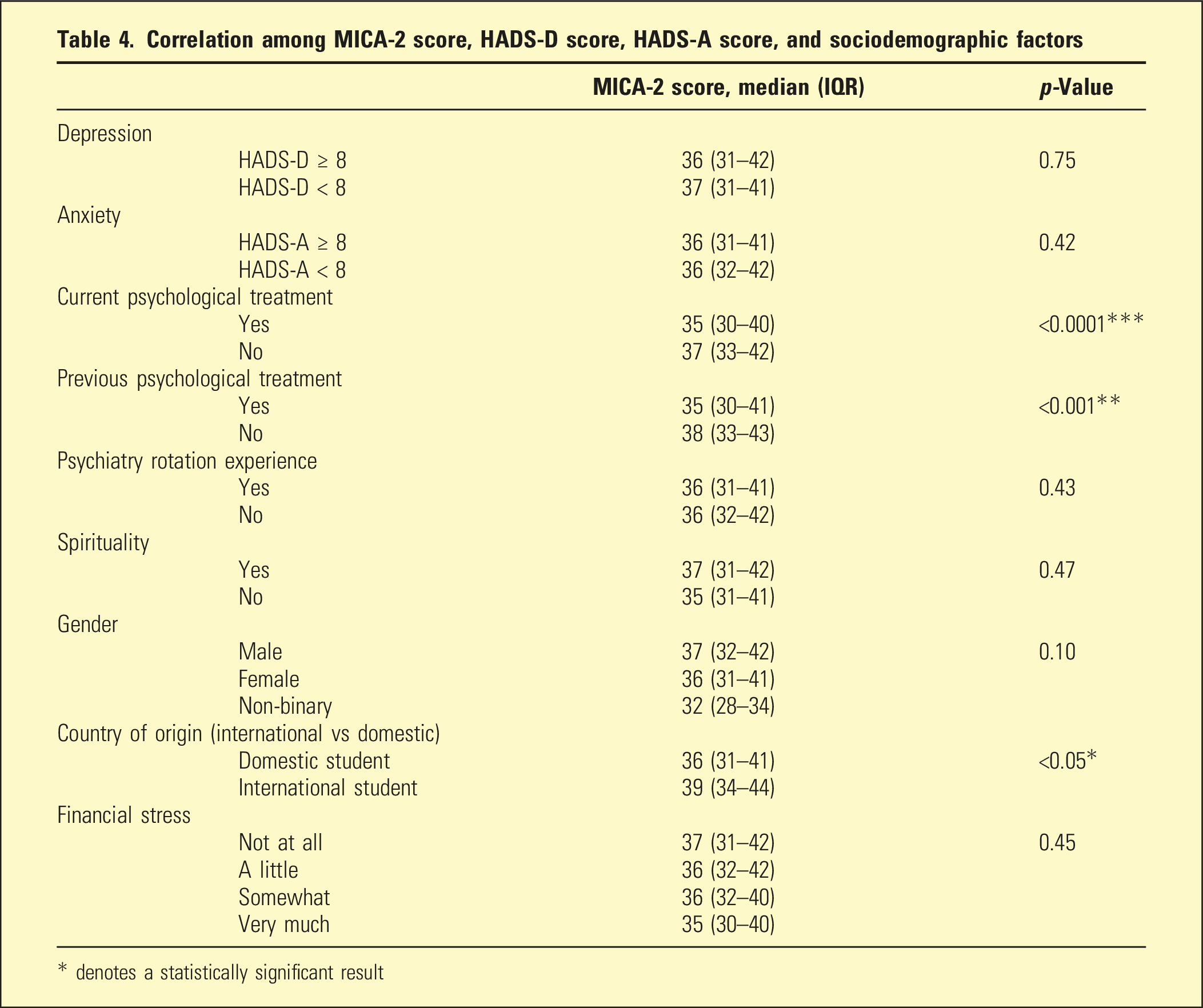
* denotes a statistically significant result
Discussion
Based on our review of the literature on MEDLINE from 2010 to present, this is the first Australian study using a validated instrument to assess stigma towards mental illness amongst medical students. The mean MICA-2 score was 36.77, the mean HADS-A score was 9.30 (SD: 4.40), and the mean HADS-D was 4.67 (SD: 3.70). Consistent with the primary hypothesis, we found no significant association between MICA-2 scores and sociodemographic factors. We found that students who reported current or past psychological treatment had lower MICA-2 scores than those who did not. However, contrary to the secondary hypothesis, HADS scores were not associated with MICA-2 scores.
MICA-2 scores were normally distributed. The mean MICA-2 score of 37 in our study is lower than the neutral score of 48 and lower than those found in surveys of medical students at UWA (43.5), medical students in Chile and Spain (40.17), and across a worldwide study of medical students in 65 countries (40.5).9–11 Contrary to the UWA study, we found no significant difference between MICA-2 scores of participants who had completed a psychiatry clinical rotation. 11 These differences may be attributable to the uptake of mental health programs such as Mental Health First Aid (MHFA), 21 which UWA introduced for preclinical students in 2016, and ∼8000 medical students were trained in MHFA between 2020 and 2022 under Australian government agreements. 22 Exposure prior to a psychiatry rotation may account for the lack of decrease in MICA-2 score after a psychiatry clinical rotation, and this may also account for the lower MICA-2 scores overall.
We found no significant association between MICA-2 scores and clinically significant symptoms of depression or anxiety (p = 0.75 and p = 0.42, respectively). 3 Therefore, the model of stigma has limited explanatory effect regarding psychological distress in medical students. Most participants (n = 325;54.3%) had HADS-A scores ≥ 8, indicating clinically significant symptoms, and 34.1% had scores ≥ 11 suggesting an anxiety disorder. This is higher than findings from the 2013 BeyondBlue study, which found that 7.5% of participants self-reported an anxiety disorder. 7 There were 115 participants (19.23%) with HADS-D scores ≥8 and 7.7% with scores ≥ 11, which is comparable to the BeyondBlue finding that 8.1% of participants self-reported a depression diagnosis. 7
Participants who endorsed previous or current treatment for a psychological condition had lower stigma scores than their counterparts (35 vs 38, p < 0.001, and 35 vs 37; p < 0.0001, respectively). However, this is unlikely to be clinically significant, as it represents a small reduction in stigma scores that were already low. It is possible that participants who sought psychological treatment may have had inherently lower levels of stigma, as stigma may be a reason for insufficient help-seeking.
Consistent with findings from a 2019 study, 23 we found that international students had significantly higher MICA-2 scores. However, international students were underrepresented when compared to national enrolment data. 24 Therefore, our results are not conclusive, and further research is required to elucidate the factors that underpin these attitudes. Finally, we found no association between MICA-2 scores and self-reported religiosity. The link between religiosity and stigma is not well established, and existing literature yields inconclusive results. 25
Limitations
A major limitation of our study is that our data are derived from a volunteer sample rather than a random representative sample. Methodological limitations include using email recruitment, and despite the findings of the Continuum of Resistance model, the presence of participation bias cannot be excluded. Whilst we intended to survey to all Australian medical students, following consultations with various medical faculties, the need for multi-institutional ethical approval and faculty-specific requirements for censorship of survey content were identified, and several medical schools declined participation. Consequently, a smaller sample of 5539 students was utilized. Therefore, although our results may be indicative, they are not necessarily generalizable to the entire population of Australian medical students due to the uncertain representativeness of the sample, especially regarding gender distribution and international students. International students were under-represented and female students were over-represented. These gender differences can be interpreted as reflecting gender-specific expectations leading to greater representation of women in online research. 26 Subgroup analysis between the WA and AMSA cohorts found statistically significant differences in gender distribution. The implications of this remain unclear, and there was no significant difference in other variables. Finally, the 10.5% response fraction is low, but in keeping with comparable studies,27–30 limiting our ability to generalize these results with confidence.
Conclusion
Our findings should be considered together with AMSA’s Mental Health and Wellbeing policy, and further research can provide the foundation for the implementation of mental health interventions in medical schools across Australia. These include access to an external mental health clinician, leave of absence, and academic consideration policies. The effectiveness of such interventions is yet to be tested.
Supplemental Material
Supplemental Material - Stigmatizing attitudes towards mental illness: A cross-sectional survey of Australian medical students
Supplemental material for Stigmatizing attitudes towards mental illness: A cross-sectional survey of Australian medical students by Annora Kumar, Zhao Feng Liu, Jessica Han, Sasha Patil, Lucy Tang, Paul McGurgan and Osvaldo P Almeida in Australasian Psychiatry
Footnotes
Acknowledgements
The authors thank the medical faculties at The University of Notre Dame, Curtin University, and the University of Western Australia, as well as the Curtin Association of Medical Students and Western Australian Medical Students Society for their help with the dissemination of this survey.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.