
Abstract
Keywords
A single re-experiencing symptom is required for the diagnosis of post-traumatic stress disorder (PTSD) in DSM-IV [1] and the proposed diagnosis in DSM-V [2]. With post-traumatic dreams the second most common re-experiencing symptom behind daytime intrusions [3], diagnosis may well rest on the accurate assessment of post-traumatic dreams. There is currently no consensus on the parameters of the DSM-IV B2 diagnostic criterion [4] or clarity in the differentiation between the post-traumatic dreams of PTSD and the highly prevalent post-traumatic dreams of people exposed to trauma who do not develop PTSD [5]. Furthermore, dreams are conceptualised differently across fields; an intrusive symptom in the PTSD field [6–8] and an adaptive emotional processing mechanism in the dreaming field [9,10]. Comparisons of the extent to which they are distinct or related phenomena have been hindered by different research methodologies and foci of enquiry across the two fields [4].
In a recent review of existing research into PTSD dreams, Phelps et al. [4] note that the ‘hallmark’ post-traumatic nightmare of PTSD is often described as a repetitive replay of the traumatic event, complete with accompanying cognitive, affective, physiological and behavioural responses [11–13]. They note that this phenomenology is recognised alongside a broader range of dreams that are understood by the dreamer to symbolise, or be related to, the traumatic event while varying in the extent to which the actual event is replayed [14–16]. The goal of this study was to explore the dreams in a population with an established diagnosis of PTSD in order to contribute to greater understanding of the phenomenology. Both the DSM-IV (‘recurrent distressing dreams of the event’) and proposed DSM-V criteria (‘recurrent distressing dreams in which the content and/or affect of the dream is related to the event(s)’) require recurrent, distressing dreams of, or related to, the trauma. This study aimed to address the following key questions:
To meet the ‘recurrent’ requirement, does dream content have to remain unchanged over time or do constantly changing distressing dreams of the event qualify? A key difference between the repetitive dreams of PTSD and those that resolve over time may lie in the ‘stuckness’ of their content and/or affect. Hartmann [9] describes the typical evolving pattern of content and affect as the traumatic experience is processed. This evolution may discriminate between PTSD dreams that remain stuck in repetition and normal dreams that resolve. This study investigated whether the B2 criterion dreams in participants with PTSD had changed or remained the same over time.
To meet the ‘distressing’ requirement, do dreams have to be so distressing that they lead to immediate awakening, as is required to meet DSM-IV [1] and proposed DSM-V [2] diagnostic criterion for nightmare disorder, or do less distressing dreams that are only remembered upon awakening in the morning qualify? Hartmann [9] has proposed that broader connections in the mind (between people, memories, experiences) are made during dreaming and this facilitates the integration of new material following trauma, and hence, emotional processing. Post-traumatic dreams that cause sufficient distress to lead to immediate awakening, and thereby bypass the opportunity for emotional processing during sleep, may be specific to PTSD. This is consistent with the notion of competing psychological processes in which traumatic memory is brought to mind in order to ‘work through’ the experience and then avoided (e.g. when the person awakens) when the memory becomes overwhelming [17]. This study investigated whether the B2 criterion dreams of study participants were associated with immediate awakening, or were only remembered in the morning.
With rard to the content and/or affect being related to the event, do one or both of these features have to relate to the person's experience at the time of the trauma, or does content or affect that reflects subsequent understandings or emotional processing of the event qualify? This question goes to the core of the conceptualization of the post-traumatic dream as an intrusive symptom arising from the encapsulated memory of the trauma [7] and the extent to which the traumatic experience needs to be replayed in the dream to meet the diagnostic criterion. With regard to content, a critical empirical question is whether dreams in which the content differs from waking memory of the traumatic event are associated with less severe PTSD than replay dreams? This would support a continuum of post-trauma dream phenomenology, rather than a categorical distinction between PTSD and non-PTSD dreams [9,18]. A related question is whether there are key differences in affect associated with dream types (replay and non-replay) that may reflect varying degrees of emotional processing. In this study, dream affect was compared with the emotions experienced at the time of the traumatic event. Dreams in which the original affect remains stuck, even when original content differs, may differentiate PTSD from non-PTSD dreams. We hypothesized that dream affect would be the same as that experienced at the time of the trauma, reflecting unsuccessful emotional processing of the event.
In addition to these three elements of the proposed diagnostic criterion, there may be key differences in the phenomenology of PTSD and non-PTSD dreams following trauma, for example in their sensory or somatic features [4]. This study investigated the phenomenology of PTSD dreams using features reported in daytime intrusions [19–21] to establish a basis for comparison with normal dreams following trauma in future research.
Method
Participants
The sample comprised forty veterans recruited from veterans' mental health services where they were undergoing routine maintenance treatment for their PTSD or comorbid mental health problems. Information about the study was provided to treating clinicians who were asked to invite appropriate patients to consider participation. Veterans willing to participate were contacted by the first author. After complete description of the study to the participants, written informed consent was obtained. One participant declined to participate being unwilling to describe his post-traumatic dreams. Of these participants 85% were taking anti-depressant medications, most commonly SSRIs. In one third of cases, antidepressant medication was augmented with an atypical antipsychotic. Inclusion criteria included exposure to a traumatic event (as defined by DSM-IV PTSD Criterion A) in the context of military service, a clinical diagnosis of PTSD and self-report of trauma-related dreams. Participants were excluded if they had no memory of the traumatic event, had sustained a moderate to severe head injury, or were currently suicidal or psychotic. Approval for this study was obtained from the Institutional Ethics Committees of the organizations involved.
Measures
PTSD was assessed using the Clinician Administered PTSD Scale (CAPS) [22,23]. Comorbid mental health problems were assessed with widely used and validated measures in PTSD research: the World Health Organization's Alcohol Use Disorders Identification Test (AUDIT) [24]; the Beck Depression Inventory (BDI-II) [25]; and the Beck Anxiety Inventory (BAI) [26]. Sleep quality was assessed by the Pittsburgh Sleep Quality Index (PSQI) [27] and the Pittsburgh Sleep Quality Index Addendum for PTSD (PSQI-A) [28].
As part of a structured interview, participants were asked to describe their experience of post-traumatic dreams since the trauma, with particular emphasis on changes in frequency, associated distress and extent of trauma replay over time. To investigate the phenomenological features of post-traumatic dreams, participants were asked to select one current trauma-related dream on which their endorsement of CAPS item B2 was based. Participants with more than one recurrent dream in the past month were asked to select the most distressing dream. This is consistent with Ehlers and colleagues' [20,29] phenomenological investigation of daytime PTSD intrusions. Participants with minor variations within a recurring dream were asked to select the most typical dream. Concern about the limited reliability of dream content based on a single dream report [30,31] was mitigated by the repetitive nature of the dreams under investigation in this study.
In the absence of an established measure of nightmare phenomenology, the phenomenological questions were derived from previous research into post-traumatic dreams [32, Mellman T: personal communication] and daytime intrusions [20,29,33,34]. Participants were asked to rate features of their dreams on a 5-point Likert scale (0 = not at all; 1 = a little bit; 2 = moderately; 3 = quite a bit; 4 = extremely). In light of the potential for dream affect to evolve [9], participants were asked to identify the dominant emotions associated with their dream and with the original trauma. Table 1 shows the questions on dream phenomenology and associated affect.
Questions on the phenomenological features and associated affect of dreams
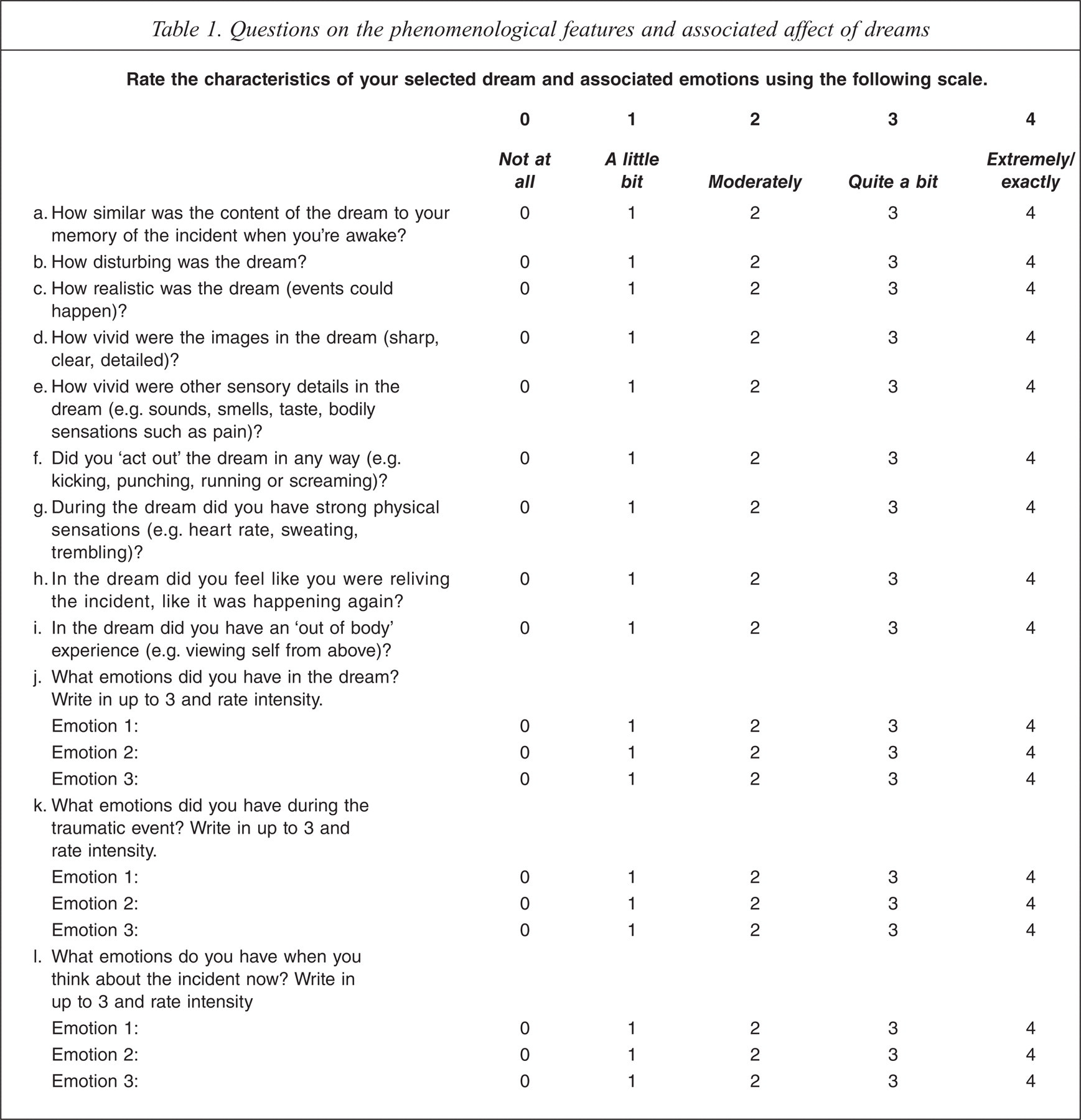
The scope of enquiry into the selected dream included:
Dream content: participants were asked to narrate the events of the dream and to say how the dream differed from their memory of the actual traumatic experience. Dreams that did not differ were categorized as replay, dreams that were completely different as non-replay, and dreams that combined actual traumatic experience with events that did not actually occur were categorized as mixed replay/non-replay. No attempt was made to verify participant's memory of traumatic events against the actual event, as our interest lay in the relationship between waking memory and night time re-experiencing of the event. Participants were also asked whether the dream represented the full replay of the event, events leading up to it, only the worst aspects, or worst fears of what might have happened.
Associated affect: participants were asked to nominate the dominant emotion(s) experienced (i) during the dream, (ii) at the time of the traumatic event, and (iii) in the current waking recollection of the event.
Other phenomenological features: participants were asked to rate their dream on dimensions of how disturbing, vividness of images, vividness of other sensory details, associated behavioural re-enactment, physical sensations, ‘out of body’ experiences and dream modality (thought-like or sensory experience).
To gather evidence for the parameters of ‘distress’ and ‘recurrent’, participants were asked about the impact of dreams on sleep: immediate awakening or only remembered on awakening in the morning, as well as whether the selected dream had recurred unchanged over time.
Distress associated with dreams was further assessed using the Nightmare Distress Questionnaire (NDQ) [35]. This 13-item questionnaire is designed to measure anxiety, avoidance, realism and importance associated with nightmares, as well as their impact on sleep and general well-being. Items are scored on a 5-point Likert scale. The author reports internal consistency for the NDQ of between 0.83 and 0.88 across four studies of university students. Good internal consistency (α = 0.80) has been reported [36] along with preliminary evidence for the construct validity [37].
Results
Participant characteristics
Participants' mean CAPS score was 68.25 (SD = 17.68). Most participants (n = 29) served in Vietnam, with the remainder serving in a range of Australia's overseas deployments including Malaya, Cambodia, Somalia, Rwanda, East Timor, Iraq and Afghanistan. Two participants had no overseas deployment but were exposed to trauma (serious motor vehicle accident and interpersonal assault) in the course of their military service.
Participants' ages ranged from 28 to 65 (mean (M) = 56.03; standard deviation (SD) = 9.02). All were Caucasian with 90% Australian born. Over 70% were married or in de facto relationships and 85% were no longer working. Time since trauma ranged from 4 to 42 years (M = 31.75; SD = 12.75). The study participants represent a sample of veterans with chronic PTSD (mean duration of PTSD = 30.48 years; SD = 13.27).
Consistent with the high level of comorbidity associated with chronic PTSD [38,39], participants in this study reported problematic alcohol use (average AUDIT score of 15.18, SD = 11.79), moderate depression (average BDI-II score of 27.46, SD = 11.75) and moderate anxiety (average BAI score of 23.74, SD = 12.64).
Participants also reported significant sleep problems. Global scores on the PSQI ranged from 5 to 19 with an average score of 12.60 (SD = 3.85). With global scores of >5 considered to indicate significant sleep disturbance, all participants reported disturbed sleep, with the average rating indicating severe sleep disturbance. PSQI-A scores ranged from 1 to 18 with a mean sore of 9.80 (SD = 3.93), reflecting high prevalence of the sleep disturbances typically associated with PTSD.
Post-traumatic dreams
Participants' report on the pattern of their dreams since the trauma revealed considerable variability in frequency, attributed to the variable course of PTSD, changes in medication and alcohol use. Thirteen reported no change in frequency over time, 12 reported that dreams had become more frequent, 13 that they had become less frequent and two were unable to say. There was less variability in dream distress over time, with 23 reporting no change in distress, six reporting more distress and 11 reporting less distress over time. Similarly, with regard to degree of trauma replication over time, most (n = 27) reported no change in content while 10 reported less replication and three more. Chi square indicated a significant relationship between change in degree of replication and change in distress (x24, N = 40) = 20.02, p < 0.001). The small number of participants who reported an increase over time in trauma replication and/or distress attributed this to a reduction in alcohol use or changes in medication.
Participants reported between 1 and 3 current post-traumatic dreams meeting the DSM-IV B2 criterion, with about half (55%) reporting only one. The following data refer to the single dream chosen by each veteran as the most distressing or most typical of the dreams they experience.
Content. Ehlers and colleagues characterized daytime intrusive symptoms as brief sensory fragments of events immediately preceding the worst aspect of the trauma [19]. In contrast, the post-traumatic dreams of veterans in this study involved lengthy and elaborate storylines of the whole event or the person's worst fears of what could have happened. Nearly half (45%) of participants reported a replay post-traumatic dream. The most common dominant images in replay dreams were horrific scenes such as discovery of dead /mutilated bodies and scenes of combat. A further 30% of participants reported dreams that were mixed. The dominant image in most of these dreams was combat, with the changed element increasing the risk to self (e.g. mortars landing closer in dream than in reality). The remaining 25% of participants had dreams that were non-replay. For example, being called up again, being asked to do things they were not trained for, actions being ineffectual.
Mean (standard deviation) of CAPS scores across the three dream types of replay, mixed replay/non-replay, and non-replay were 71.33 (18.29), 67.17 (19.03), and 64.00 (15.49) respectively. ANOVA indicated no significant differences in PTSD severity (F (2,37) = 0.572, not significant (NS)) between veterans with replay, mixed and non-replay dreams. Mean (standard deviation) time since trauma was 32.06 (12.55) years, 27.67 (15.94) years and 36.10 (7.32) years for the replay, mixed and non-replay dreams respectively, with ANOVA indicating no significant differences (F (2,37) = 1.214, NS).
Affect. Fear was the most common affect associated with all types of post-traumatic dreams, being reported in 75% of the dreams. Of the replay dreams, 60% were associated with fear, while other less common emotions were helplessness (25%) despair (20%) and anger (15%), and in a small number of cases (10%), horror and guilt. Fear was associated with 90% of the mixed replay/non-replay dreams and with 70% of the non-replay dreams, alongside anger in 50% of cases.
In over 75% of dreams, the affect experienced in the dream was the same as that experienced during the trauma, even when the dream content was not a replay of that event. Of the remainder, six (15% of the total) reported an absence of emotion at the time of the event but experienced emotions in the dream that may have been suppressed during the event. These included, for example, veterans who reported that their ‘training kicked in and felt nothing’ at the time of the event but experienced fear when the event was replayed in their dream and others who reported feeling ‘numb’ during the event but experienced despair or guilt in the dream. In a small number of the replay dreams, the affect differed from that associated with the original event in a way that was consistent with secondary reflections on the original event; for example, fear at the time of the event had turned to anger in the dream. Previous research has found that anger is a factor in the maintenance of PTSD [40] and a negative predictor of treatment outcome [41], blocking the necessary activation of fear during prolonged exposure [42].
There were only three dreams from this sample of 40 in which neither the content nor the affect was the same as that experienced at the time of the trauma. Each of those dreams involved being called up again for service in Vietnam and feeling anger at ‘not being heard’.
‘Recurrent’. In this sample of veterans, all reported that the selected post-traumatic dream, whether replay, mixed or non-replay, had recurred since the time of trauma with the same or very similar content. In some cases there were minor variations that had always occurred in the dream. For example, the dream might start at two or three different points during the event, or the face of different family members might appear on a dead body. Importantly though, these variations had been present from the onset of dreams rather than developing over time.
‘Distressing’. Means (standard deviation) of NDQ scores across the three dream types of replay, mixed replay/symbolic and symbolic were 41.05 (7.79), 37.25 (11.49) and 36.50 (5.79) respectively. ANOVA indicated no significant differences between dream types on NDQ scores (F (2,37) = 1.15, NS). Ninety percent of participants rated their dream as 3 or 4 indicating the dream was ‘quite a bit’ or ‘extremely’ disturbing. A similar proportion (87.5%) indicated that the dream led to immediate awakening some (40%), or all of the time (47.5%). Just five participants reported that they only remembered the dream on awakening in the morning. T test revealed a significant difference between this group and others on rating of physiological arousal associated with the dream (M = 1.80, SD = 1.78 versus M = 3.09, SD = 1.07; t (38) = 1.56, p < 0.05).
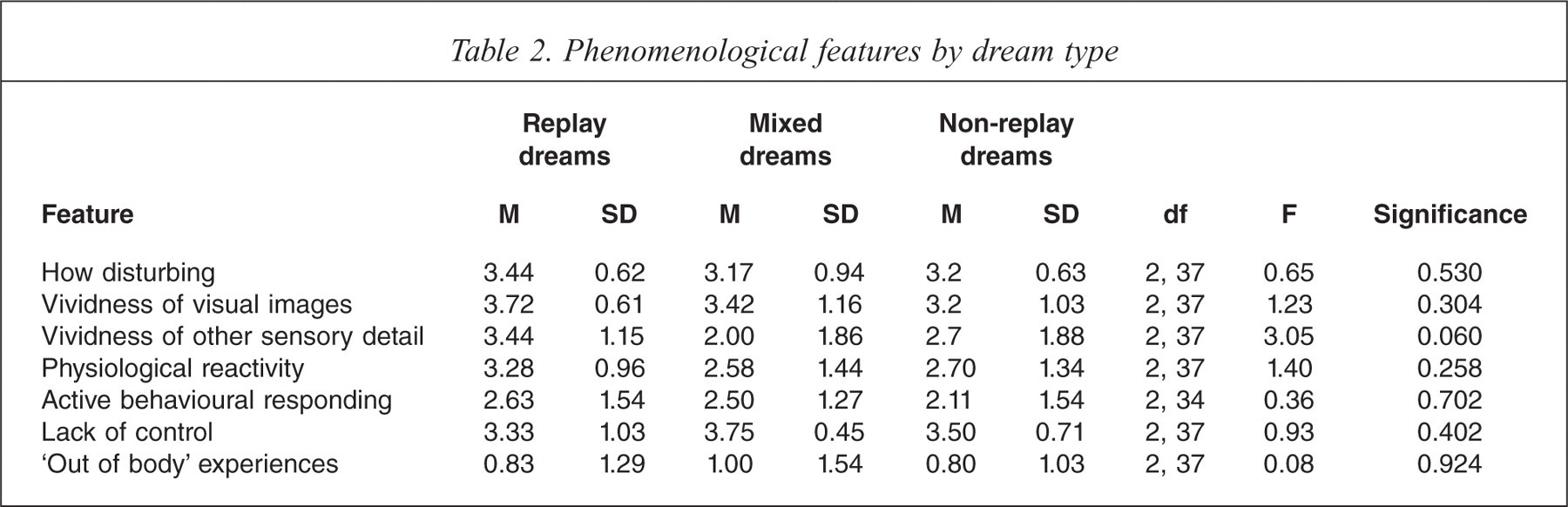
Other phenomenological features. The mean ratings and standard deviations for the three dream types on the key phenomenological features identified in daytime intrusions are presented in Table 2. Like daytime intrusions, the dreams in this study were rich in sensory detail, were associated with physiological reactivity and behavioural responding, and lacked a sense of control. ANOVA indicated no significant differences between dream types on any of these features. The difference between dreams on vividness of non-visual sensory details (sound, smell, taste and touch) approached significance (F (2,337) = 3.05, p < 0.06), with this phenomenon (particularly sound and smell), more consistently associated with replay dreams.
Phenomenological features by dream type
Discussion
This investigation of the dreams of veterans with PTSD provides preliminary empirical evidence for the key parameters of the symptom criterion of post-traumatic dreams of PTSD. All participants reported that the selected dream had recurred with little change since the trauma, irrespective of dream type, suggesting that those dreams that persist over time are more likely to be those that remain unchanged. As such, these results support the interpretation of ‘recurrent’ in the DSM definition to be the same dream recurring, rather than various recurring dreams of the trauma.
In almost all cases, dreams were rated as ‘quite a bit’ or ‘extremely’ disturbing and led to immediate awakening at least some of the time. The five dreams that did not lead to immediate awakening were associated with lower physiological arousal. Immediate awakening from dreams has been found to be related to severity of distress [43] and is specified in the DSM-IV classification of nightmare disorder. The results of this study suggest that most of the dreams of PTSD are sufficiently disturbing to be classified as nightmares.
In terms of content, there was little evidence that replay dreams were associated with more severe PTSD than non-replay or mixed dreams. This supports diagnostic criteria that include all dream types. The affect reported in most dreams in this sample (replay, mixed and non-replay) was the same as that experienced at the time of the traumatic event. There was no indication of greater emotional processing in non-replay dreams. Taken together, these findings support a diagnostic criterion that requires the content or affect of the nightmare to be the same as that experienced at the time of the event. This would encompass replay dreams in which the affect was different from that experienced at the time of the event (for example, fear experienced at the time of the event and anger or guilt experienced in the dream) as well as non-replay dreams in which the affect is the same as that experienced at the time of the event (for example, a ‘fictional’ combat scene associated with the same fear experienced during the real traumatic event). We would propose that it should also encompass dreams in which dream affect is consistent with emotions that may have been suppressed at the time of the trauma (for example, feeling ‘numb’ during the event but fear during the dream).
All the PTSD dreams were characterized by rich sensory detail and somatic involvement. Investigation of phenomenological features of non-PTSD dreams is required, however, in order to determine whether this differentiates PTSD from non-PTSD dreams.
Limitations
This study was restricted to veterans with chronic PTSD and limited by a small sample size of volunteer participants. The extent to which these findings can be generalised to a broader population of other veteran samples or civilians with PTSD is unknown. The limitations of retrospective dream recall in terms of under-reporting frequency [44] and potential bias towards dreams with negative content [45] are also acknowledged. The phenomenological features described are based on a single most distressing or typical dream and may not apply to all B2 criterion dreams. The current study did not investigate all of the dreams of participants, which may well include a mix of trauma and non-trauma related content [46,47] as well as dreams with varying degrees of associated distress [48].
The study participants were characterized by a high level of comorbid depression, anxiety and alcohol use and the majority were taking psychotropic medication. The potential impact of these factors on nightmares needs to be acknowledged. Previous research has established that increased nightmare prevalence [49] and distress [50] is associated with depression, anxiety and substance use disorders, although there is inconsistent evidence for the additive effect of comorbid conditions on nightmares in people with PTSD [51,52]. Further, vivid nightmares can be induced in some patients by antidepressant and antipsychotic drugs that affect the neurotransmitters serotonin and dopamine, as well as by withdrawal from substances such as alcohol and benzodiazepines that suppress rapid eye movement (REM) sleep [53]. Thus, the comorbid mental health problems, alcohol misuse and prescribed medication of the study participants may have contributed to their nightmare experience beyond the impact of their PTSD. Regrettably, accessing a chronic PTSD sample without these complications in order to explore this issue further would be extremely difficult.
The extent to which these findings can be generalized across a broader PTSD population needs to be established. Ideally, a similar investigation of trauma-related dreams in people with acute PTSD, and different trauma populations is required. Beyond that, an investigation of the non-trauma/trauma-related dreams of those who do not develop PTSD would elucidate issues of specificity and sensitivity. In practice, however, recruiting a sample of trauma survivors who continue to have trauma-related dreams but who do not meet criteria for PTSD is a significant challenge.