
Abstract
Existing evidence suggests that the prevalence of childhood sexual abuse (CSA) in Australia is up to 40% in women, and 15% in men [1]. As these estimates are high, researchers and policy commentators have been increasingly interested in determining which broad environmental factors are associated with CSA [2].
Views on the aetiology and risk factors of CSA are contained within the broad theories of child maltreatment in general [3]. Such models incorporate factors including the cultural values towards violence, socioeconomic status, and microsystem components such as family, neighbourhood, and schools. One theoretical approach put forward by ‘ecological’ theorists posits that CSA may be influenced by characteristics of the community, such as socioeconomic and familial environment around which CSA occurs [4]. Looking at each of these aspects separately, associations between socioeconomic status and CSA are not consistently found in research using self-reports of CSA [5–7]. The few existing studies show inconclusive results. Younger maternal age at birth was found as a risk factor in one study, although multivariable analysis was not performed [6]. Maternal marital circumstances such as being divorced or separated have been found to be associated with increased risk of CSA in the offspring, but only in conjunction with the presence of a non-biological male in the household [3]. A small effect between lower maternal educational attainment and increasing severity of CSA was explained by other variables in a study by Fergusson and colleagues [7]. On the other hand, evidence from clinical samples suggests that a disproportionate number of CSA comes from lower socioeconomic groups [8], but these associations may be due to greater monitoring of low SES populations by relevant agencies.
Characteristics of the familial environment appear to be associated with CSA. Parental substance/alcohol abuse was a risk factor in families reported to child protective services [9] and amongst the participants of the Christchurch longitudinal study in New Zealand [7]. A twofold increase in the risk of exposure to sexual abuse was also found in a large community sample of children who retrospectively reported parental substance misuse [10]. In the same cohort [11] respondents reporting a parental history of depression, mania, schizophrenia or antisocial behaviour were also two to four times more likely to have experienced CSA.
These findings suggest that low socioeconomic status and familial environment may be factors influencing CSA. It is possible that the identified socioeconomic factors may be indirectly related to CSA and these characteristics broadly reflect a social environment where reduced vigilance or difficulties in monitoring styles increase the possibility of sexual abuse. A neighbourhood effect could also operate. Families from lower SES are more likely to live in neighbourhoods with higher delinquency and antisocial conduct, where CSA is more likely to occur [12]. Finally, socioeconomic disadvantage may cause poor parent–child communication, which may in turn lead to increased exposure of sexual abuse in childhood. Therefore, the proposed research is rooted in an ecological framework.
A limitation of most existing studies is the use of cross-sectional or retrospective designs which make it impossible to address the temporality between CSA and socioeconomic factors. Longitudinal studies are able to follow similar families over time, thus increasing the accuracy to calculate the impact that early maternal and socioeconomic factors have on prospective CSA. Only two longitudinal studies have explored the association between socioeconomic factors and CSA. One study supported the conclusions that CSA is not related to SES. Fergusson [7] investigated whether social, familial and parenting factors were associated with an increased risk of CSA in 18 year old youths, and found a small effect between lower maternal educational attainment and CSA that was no longer seen in multivariable analysis. In contrast, a data linkage study of Brown et al. [6] using a longitudinal study of 644 families in upstate New York, USA, found that maternal youth and unwanted pregnancy were associated with both self-report and official records of CSA. Since young mothers who carry an unwanted pregnancy to term are more likely to have been brought up in deprived areas and live in relative poverty compared with their older counterparts [13], these associations may further indicate an indirect link between low SES and CSA [6].
The above evidence shows that whilst the role of socio-familial environment in CSA has been explored previously, factors have often been investigated in isolation and evidence from large longitudinal data is scant. This research project aims to build on existing research by prospectively investigating predictors of CSA within an ecological framework, focusing on early maternal and socioeconomic factors. We will be able to explore some extent of severity of CSA by separating those reporting non-penetrative from those reporting penetrative abuse. We will then prospectively assess the influence of several socioeconomic and maternal factors on both forms of abuse. This approach has not been utilized in previous longitudinal research on CSA. We will use data from the Mater-University of Queensland Study of Pregnancy (MUSP), an Australian birth cohort study of youth, to test whether there is a link between socio-familial environment and CSA.
Methods
Participants
The Mater-University of Queensland Study of Pregnancy (MUSP) [14], is a longitudinal study of women and their offspring born between 1981 and 1984 at the Mater Misericordiae Hospital in Brisbane, Australia. In total, 7223 pregnant women agreed to participate, delivered a singleton offspring who was not adopted prior to leaving hospital, and completed both initial phases of data collection. Following this, data were collected at 3–5 days after birth, 6 months after birth, and 5, 14, and 21 years after birth. We used measures from the 6 months follow up or earlier, to address the temporal nature of socioeconomic and familial factors and CSA. Offspring were compensated $20 at the 21 year follow up and apart from this, the participants were not compensated. Data was collected using a variety of methods, including physical assessments at clinics and face-to-face questionnaires administration. The response rate for CSA questions at age 21 was 3739 (52% of original cohort). Our cohort consisted of a selected subgroup of 2664 youths, who completed the childhood sexual abuse questions at the 21 year follow-up phase of the study, and had complete data on all variables included in the study.
Ethics committee approval for the study was obtained from the University of Queensland and the Mater Misericordiae Hospital at each stage of the study. Informed consent was obtained from the mothers at all follow-up phases. Both mothers and young adults provided individual informed consent at the 21 year follow up. Further information about the study is provided in detail elsewhere [14].
Measurement of sexual abuse
At the 21 year follow up of the MUSP, young adults were asked whether they had been forced to have sexual contact when they did not want and how many times this had occurred before and after the age of 16. We used the cut-off of 16 years of age, as this is the legal age of consent in the state of Queensland. They were also asked if they had ever experienced the following with someone more than 5 years older than them, and before the age of 16: (1) exposure or masturbation; (2) kissed or fondled at breasts or genitals; (3) sexual intercourse; (4) oral sex; (5) touched or masturbated the genitals of someone else. The response options were no, unsure, and yes. A composite sexual abuse variable, with ‘none’, ‘non-penetrative’, and ‘penetrative’, was created from the responses. Answering ‘yes’ to items 3 and 4 was coded as penetrative CSA and answering ‘yes’ to 1, 2, or 5 was coded as non-penetrative CSA. All other responses were coded as no CSA. The three CSA groups were mutually exclusive. If both non-penetrative and penetrative abuse was reported, the case was assigned to the penetrative group. Since we specifically wanted to investigate sexual abuse experienced in childhood, only sexual abuse prior to the age of 16 was used in the present study. Sexual abuse after age 16 was excluded from the analysis.
Socioeconomic variables
Socioeconomic status was measured using the following variables. Maternal age was grouped into three categories for ease of analysis, (12–19, 20–34, and 35 +). Maternal education was grouped into ‘incomplete high school’, ‘completed high school’, and ‘post high school’. Household income was determined by asking the mother at 6 months to select family income according to the following seven alternatives; AU$0–$2599 a year, $2600–$5199 a year, $5200–$10 399 a year, $10 400–$15 599 a year, $15 600–$20 799 a year, $20 800–$25 999 a year, and $26 000 or more a year. Income was collapsed into two groups ($10 399 or less, and $10 400 or more a year). Marital status was assessed at 6 months follow up (married, living together, single, and separated/divorced/widowed).
Maternal attitudes
Maternal attitudes towards the baby were obtained over three phases. Prepregnancy attitude was assessed using two questions asked in the prenatal period that were later collated. Mothers were asked whether the baby was wanted and had to answer yes/no/unsure to the following statements; (1) planned to get pregnant at this time, (2) meant to avoid pregnancy at this time, (3) wanted to get pregnant at this time, and (4) method of family planning failed. Scores for statements 2 and 4 were reversed and an omnibus measure created which displayed optimal internal consistency (Cronbach's alpha for the total combined score = 0.89). Mothers were also asked how they felt about their baby. Construction of this scale and the high reliability for its total scores (Cronbach's alpha = 0.85) have been reported in detail elsewhere [15]. Prepregnancy attitude was grouped as ‘Positive and baby wanted’, ‘Positive and unsure whether wanted/planned’, ‘Positive and baby not wanted/planned’, and ‘negative’. Postnatally (3–5 days after delivery), mothers were asked to circle, on a 5-point Likert-scale, how well the following statements reflect their feelings; (1) relieved when baby taken to the nursery, (2) prefer not to have the baby at night, (3) Can't resist nursing the baby, (4) Love to play with the baby, (5) Wish I could have the baby all the time. Statements 3, 4, and 5 were reversed and an omnibus measure created. The internal consistency for the total combined scores was acceptable (Cronbach's alpha = 0.74). Participants were grouped as ‘Contact wanted’, ‘Borderline’, and ‘Contact not wanted’. At 6 months post-delivery, mothers were asked to comment on the following statements regarding positive feelings towards caring for the baby: (1) Caring for my baby is very satisfying, (2) Feel so angry that sometimes I could smack my baby, (3) My baby makes me too tired, (4) My baby is so good I hardly know she/he is there, (5) Sometimes feel like hitting my baby, 6) Feel fed up looking after my baby all day. Statements 1 and 4 were reversed and an omnibus measure created. The internal consistency of the overall combined scores was acceptable (Cronbach's alpha = 0.75). Participants were grouped into ‘Always’, ‘Mostly’, and ‘Not always’. Mothers were asked at the 6 months follow up how long they had breast fed and the options were; ‘Still breastfeeding’, ‘4–6 months’, ‘7 weeks to 3 months’, ‘3 weeks to 6 weeks’, ‘2 weeks or less’, and ‘not at all’. These were collapsed into three categories, ‘Still breastfeeding’, ‘2 weeks to 6 months’, and ‘Not breastfed’.
Maternal lifestyle
Maternal cigarette consumption at 6 months was assessed by asking mothers weekly frequency and quantity of cigarettes smoked. The two variables were multiplied and collapsed into three categories. These were renamed ‘non-smoker’ (0 cigarettes a day), ‘moderate smoker’ (1–19 cigarettes a day), and ‘heavy smoker’ (20 + cigarettes a day) respectively. Maternal alcohol consumption was recorded in much the same way, with mothers asked how often they drank and how much they drank on these occasions, Answers were recoded into four categories; ‘Abstainer’ (0 glasses a day), ‘Light-drinker’ (0–0.5 glasses a day), ‘Moderate drinker’ (0.5–1 glasses a day), and ‘Heavy drinker’ (>1 glasses a day).
Maternal mental health
Maternal mental health was measured at the 6 montha follow up and included depression, anxiety, and stress. Anxiety and depressive symptoms were assessed using the Delusions-Symptoms-States Inventory (DSSI) [16]. The DSSI was validated against a clinical sample [17]. The scale contains two 7-item subscales measuring symptoms of depression and anxiety, which have been found to correlate strongly with other scales of depression including the Beck Depression Inventory [18]. The internal consistency of the overall combined scores for both depression and anxiety subscales was optimal (Cronbach's alpha = 0.827, and 0.829 respectively). Validation studies have found that a cut-off of four or more symptoms was consistent with an optimum combination of false positives and false negatives [17,19]. Consistent with the scale, symptoms of depression and anxiety were defined in this study as reporting four or more of the seven symptoms in the DSSI depression and anxiety subscales. Maternal stress was measured using the Reeder Stress Inventory (RSI) [20]. The scale comprises four items inquiring about recent feelings of tension, nervous strain, mental and physical exhaustion, and stressful daily activities. A reliability analysis of the combined scores of the scale achieved a Cronbach's alpha of 0.8, indicating good reliability. Items were summed and a cut off of 10% was used to define higher symptoms of stress.
Statistical analysis
We elected to categorize most measures used in our analysis, because of the skewed distribution of key variables and because our hypothesis did not suggest a linear association between the life course factors considered here and sexual abuse, but instead a focus on extreme groups with multiple SES problems and other predictors of sexual abuse.
Prospective analyses predicting childhood sexual abuse were conducted fitting a multinomial logistic regression model, with a 3-level categorical end-point outcome variable (‘no sexual abuse’, ‘non-penetrative abuse’ and ‘penetrative abuse’) and socioeconomic, lifestyle and mental health domains. Unadjusted and adjusted odds ratios (ORs) with 95% confidence intervals (CI) were calculated for each group of variables. Each analysis included three models. Model 1 was unadjusted, Model 2 was adjusted for gender and the influence of SES, attitude, and mental health variables independently (for example, for the analysis exploring SES, model 2 adjusted for all SES variables). Model 3 included all variables in a combined model to identify the strongest predictors for penetrative and non-penetrative abuse. Hence, associations were first evaluated separately for socioeconomic, maternal attitudes and lifestyle, and maternal mental health variables. For the socioeconomic variables, the initial multivariate model included all other SES variables. Following this, all maternal attitude and lifestyle and maternal mental health variables were entered into the final model simultaneously. Similarly for the maternal attitude and lifestyle variables, the first multivariate model includes all the maternal attitude and lifestyle variables and the second model includes all variables. The same modelling was performed with the maternal mental health variables. These results are for the 2664 young adults and their mothers with complete data on all variables included in the fully adjusted model.
Loss to follow up
In this study, complete data were available for approximately 40% of participants. Such loss can introduce bias in our results. In order to address attrition, we used inverse probability weighting (with robust methods to correct for standard errors estimates). We first used an exploratory logistic regression model to identify predictors of attrition. Those lost to follow up were significantly more likely to be born to mothers who did not complete high school (OR 1.58, 95% CI: 1.33, 1.89), were single (OR 1.46, 95% CI: 1.20, 1.79) reported greater symptoms of depression (OR 1.46, 95% CI: 1.08, 1.95) and smoked at baseline (OR 1.19, 95% CI: 1.09, 1.30). These measures were fitted in a logistic regression model (response versus non-response as outcome) to determine weights for each individual using the inverse probability of response [21]. We then repeated our multivariate analyses including the weighting adjustments. The results did not differ substantively from those presented in this paper. All analyses were performed using STATA version 10.
Results
Of the 2664 participants who completed the sexual abuse questions and whose mothers provided responses for all variables included in the analysis, 16% reported non-penetrative abuse and 8.8% reported penetrative abuse. Women more likely to report both non-penetrative and penetrative CSA with 20.2% of women reporting non-penetrative abuse compared with 11.4% of men and 10.2% compared with 8.1% for penetrative abuse. (χ2 = 63.78, p < 0.001).
CSA and SES
Table 1 shows the associations between childhood sexual abuse and socioeconomic factors. Except for gender, none of the SES variables were associated with non-penetrative CSA. For penetrative CSA, there were associations with several SES variables, with lower income, younger maternal age [13–19], lower education level and a marital status other than being married, all univariately associated with CSA. In the final model, incomplete high school, mother not married due to separation, divorce, being widowed, or only living with partner, remained significant.
CSA and maternal lifestyle and attitude
Both moderate and heavy maternal smoking was associated with an increased incidence of non-penetrative CSA (Table 2). Only heavy maternal smoking remained significant in the fully adjusted model. Never being breastfed was originally associated with non-penetrative CSA but was confounded by the other maternal attitude and lifestyle variables. Feeling positive about the baby, but not having planned/wanted the pregnancy increased the risk of non-penetrative abuse. Moderate and heavy maternal smoking was also associated with increased penetrative CSA and this remained significant in the final model (Table 2). High alcohol consumption and never breastfeeding were also associated with higher incidence of penetrative CSA, although these failed to attain significance in the final model.
CSA and maternal mental health
Table 3 shows the association between maternal mental health and CSA. Maternal anxiety was associated with non-penetrative CSA and this remained significant in the fully adjusted model. An association between maternal depression and higher incidence of penetrative CSA was confounded in adjusted analysis. There was no relationship between maternal stress and CSA.
Discussion
The aim of this study was to examine prospectively whether there were associations between maternal factors and SES during a child's early life and both penetrative and non-penetrative childhood sexual abuse reported at 21 years of age. In the fully adjusted model, we found that maternal smoking, unwanted pregnancy, and anxiety were associated with non-penetrative CSA, whereas lower maternal education, maternal smoking, and unmarried status remained significantly associated with penetrative CSA.
The prevalence of sexual abuse reported in this study was higher than that reported in a previous longitudinal study in New Zealand [7] where 17.3% of women and 3.4% of men reported having experienced CSA before the age of sixteen, with 5.6% of women and 1.4% of men reporting abuse involving attempted or completed intercourse. In total 29.9% of women and 19% of men in this cohort reported some form of CSA before the age of sixteen, with 9.9% of women and 7.5% of men reporting penetrative abuse. This could be due to a cohort effect or alternatively, to the different ages at which self-reports of CSA were elicited (21 years in the present study compared with 18 in the Fergusson et al. study [7]).
Existing evidence is inconclusive as to whether there is an association between SES and CSA. Some studies have found no associations between SES and sexual abuse [7]. In this large longitudinal study, we found that after accounting for a range of important confounding factors, those born of mothers who reported lower education were at increase risk of penetrative CSA. This is in contrast with findings from the New Zealand birth cohort study assessed at age 18 [7], where a relationship with maternal education was no longer seen after adjustment. Unlike the New York study [6] we were able to account for a range of important factors and found that the association between maternal age and CSA was no longer significant in the fully adjusted model. Maternal smoking was also an important predictor of both non-penetrative and penetrative CSA in this study. The association between smoking and low SES is well established [22,23]. Therefore it is possible that maternal social disadvantage, reflected here as having lower education and being a smoker, is itself associated with environmental risk exposures which we were not able to measure. These associations may reflect a familial and social environment where CSA is more likely to occur. For example, increased risk for penetrative CSA in children whose mothers were separated, divorced, widowed, or living with a partner but not married supports existing findings that exposure to non-biological males within the household heightens the risk of CSA [3]. Also, lower SES families are more likely to reside in areas with higher crime and antisocial activity, which could increase the probability of CSA [12]. Future studies with greater capacity to measure these and other environmental factors are needed to increase our understanding of these associations and identify mechanisms by which SES influences CSA.
An unwanted pregnancy has previously been associated with child maltreatment in general [6] and with CSA specifically [6]. We found a prospective association between mothers who reported in pregnancy they did not plan or want their babies and offspring self-reports of non-penetrative CSA at age 21. This finding warrants further investigation as it was not feasible to address it further in this study because of low numbers in some groups. Future studies should explore whether this association is true and the mechanisms by which it operates.
Finally, our study also suggests a link between maternal mental health and CSA with stronger statistical evidence for the association with non-penetrative CSA. This supports previous findings that suggest that parental psychiatric illness increases the risk for CSA [24,25]. CSA has previously been reported as a risk factor for post-natal depression [26], but has not been prospectively associated with an increased risk of CSA in the mother's offspring. The present study offers support for the findings in Walsh's study [25], who found that those exposed to CSA retrospectively reported higher rates of parental depression compared with controls. However, maternal depression at 6 months did not remain significant once other mental health factors were considered, and this relationship needs to be further investigated in future studies. Drawing conclusions from single point measures is problematic due to the dynamic nature of mental health and this finding should be considered preliminary and furthers the need for research in this area.
In this context it is worth noting that different predictors were associated depending on the nature of the abuse reported. For penetrative CSA the SES factors unmarried status and low maternal education level appeared to be influential, whereas maternal mental health status or attitudes toward the child were not. Conversely, maternal anxiety and unwanted pregnancy were significant factors for non-penetrative CSA but were not associated with penetrative CSA. It is possible that more serious forms of CSA are influenced by more systemic factors, such as family and social structure, whereas for other forms of abuse maternal factors, reflected by maternal poorer mental health and early lack of emotional commitment to motherhood, are more critical. If this study was supported by other research, there would be implications for intervention with young mothers at risk. This is, however, speculative, as more evidence is required to determine whether different factors are at play in influencing different forms of CSA. Hence, our findings should be seen as preliminary evidence, to be replicated and confirmed by other studies with similar measures and research designs.
The findings from this study are subject to some limitations. An important limitation is the lack of paternal data. Though the vast majority of child sex offenders are male, there is a paucity of longitudinal research addressing the relationship between paternal psychological and social characteristics with CSA. Although we used several maternal attitude variables these may have been insufficient to tease out the complicated relationship between parenting style and CSA. Another limitation is that self-reported measures of CSA status were only available retrospectively in this study. This may be susceptible to recall bias and socially desirable reporting, though some suggest that retrospective reports allow for ‘adequately reliable accounts’ [27].
Also, we had no data exploring other details of CSA, for example frequency and severity of the abuse, identity of the perpetrator, and the experience of multiple types of abuse co-occurring with CSA. Future studies with the capacity of investigating these additional characteristics are needed to better understand social and individual predictors of sexual abuse. Whilst our study is rooted in an ecological framework, it does not consider wider community effects, such as those concerning neighbourhood and school. Further research is needed to assess the impacts these have on CSA and how they interact with familial factors.
Another limitation is the loss to follow up in our cohort. Comparisons between those lost to follow up and those retained in the study showed that attrition was differential. This may introduce bias in the findings. A worst case scenario in our study would involve lower prevalence of risk factors and CSA among those lost to follow up, which would lead to results overestimating the association between the identified risk factors and CSA. However, as we found that those lost to follow up were more likely to be single, less educated, depressed and to be smokers, this is unlikely. Indeed, it is more likely that the bias is in the opposite direction, suggesting that the associations presented here may underestimate the magnitude of the association between the factors explored and later self-reported CSA. In order to explore this issue further, we have attached inverse probability weighting to subjects included in the analyses and found the weighted results did not differ substantively from those reported here. This provides some support for the claim that attrition is unlikely to have biased our results.
Despite these limitations, a key strength of this study is that it is a large birth cohort study spanning 21 years, the largest cohort on which these associations have been studied. This is the first large longitudinal study to look at both non-penetrative and penetrative CSA and our results suggest that different factors are influential for different forms of CSA. Future prospective studies are needed to confirm our findings but we offer preliminary support for CSA to be considered within an ecological framework similar to other forms of child maltreatment.
Odds ratios and 95% confidence intervals for gender and socioeconomic status variables and the association with CSA
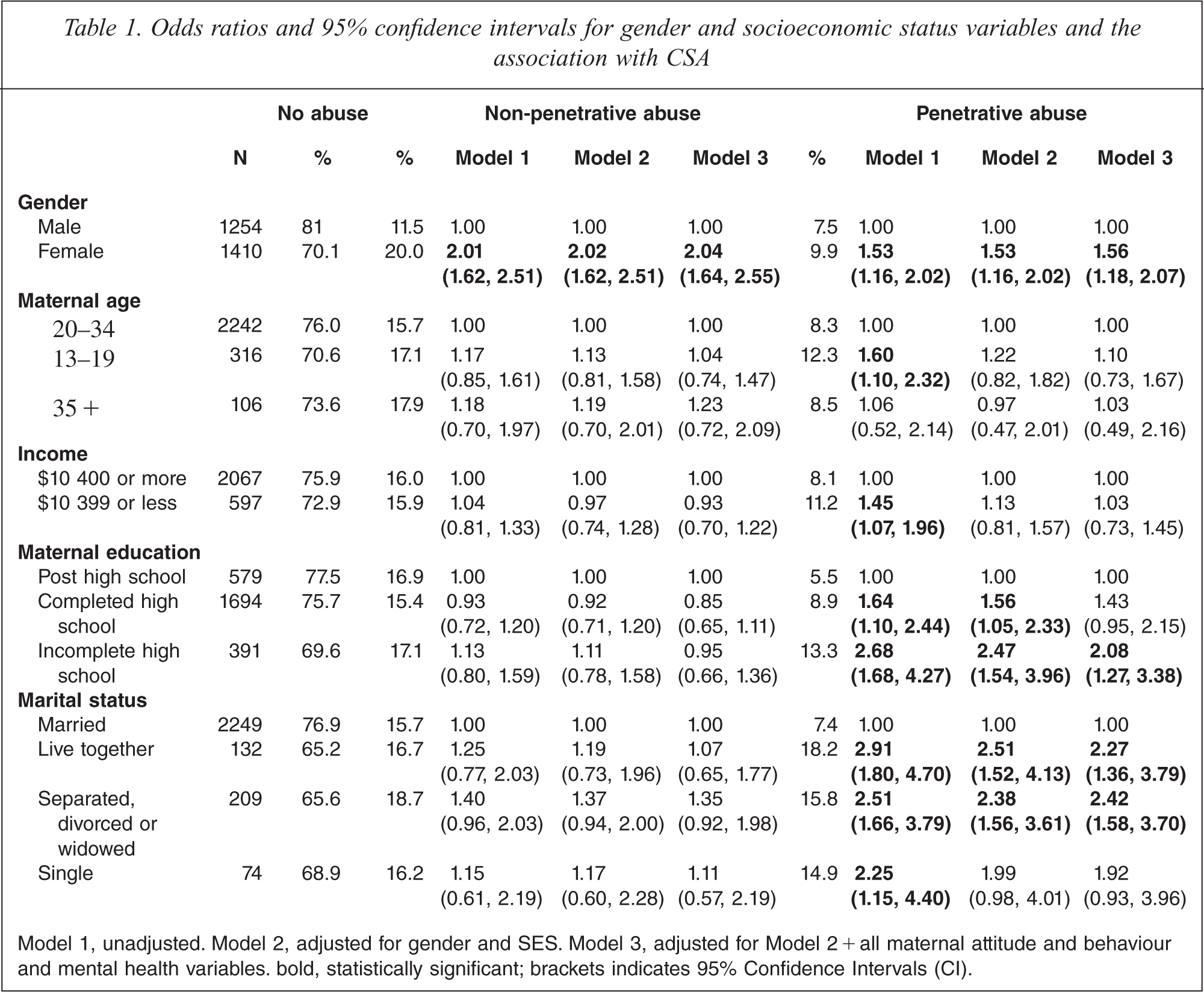
Model 1, unadjusted. Model 2, adjusted for gender and SES. Model 3, adjusted for Model 2 + all maternal attitude and behaviour and mental health variables bold, statistically significant; brackets indicates 95% Confidence Intervals(CI).
Odds ratios and 95% confidence intervals for maternal lifestyle variables and the association with CSA
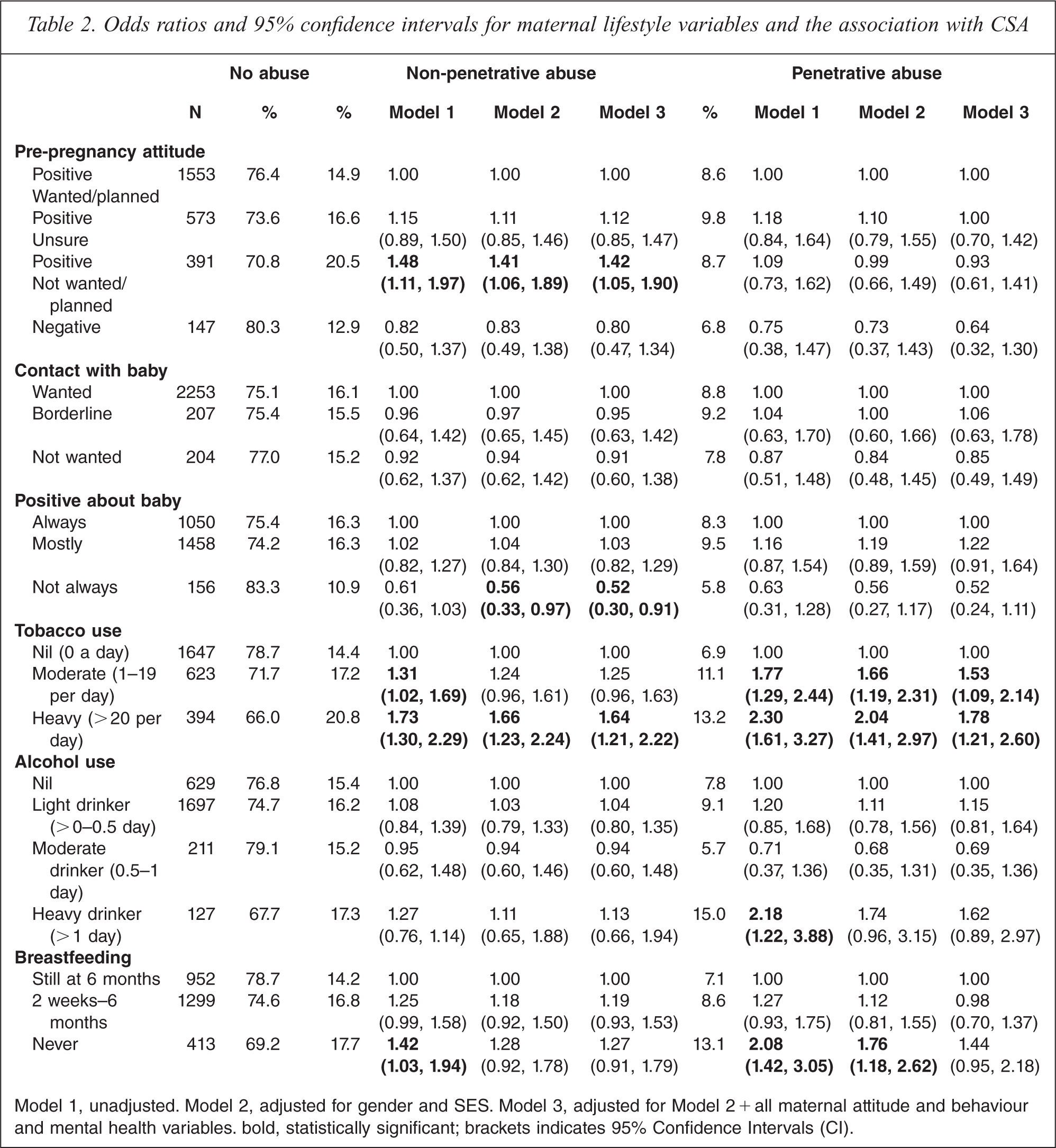
Model 1, unadjusted. Model 2, adjusted for gender and SES. Model 3, adjusted for Model 2 + all maternal attitude and behaviour and mental health variables bold, statistically significant; brackets indicates 95% Confidence Intervals(CI).
Odds ratios and 95% confidence intervals for maternal mental health variables and the association with CSA
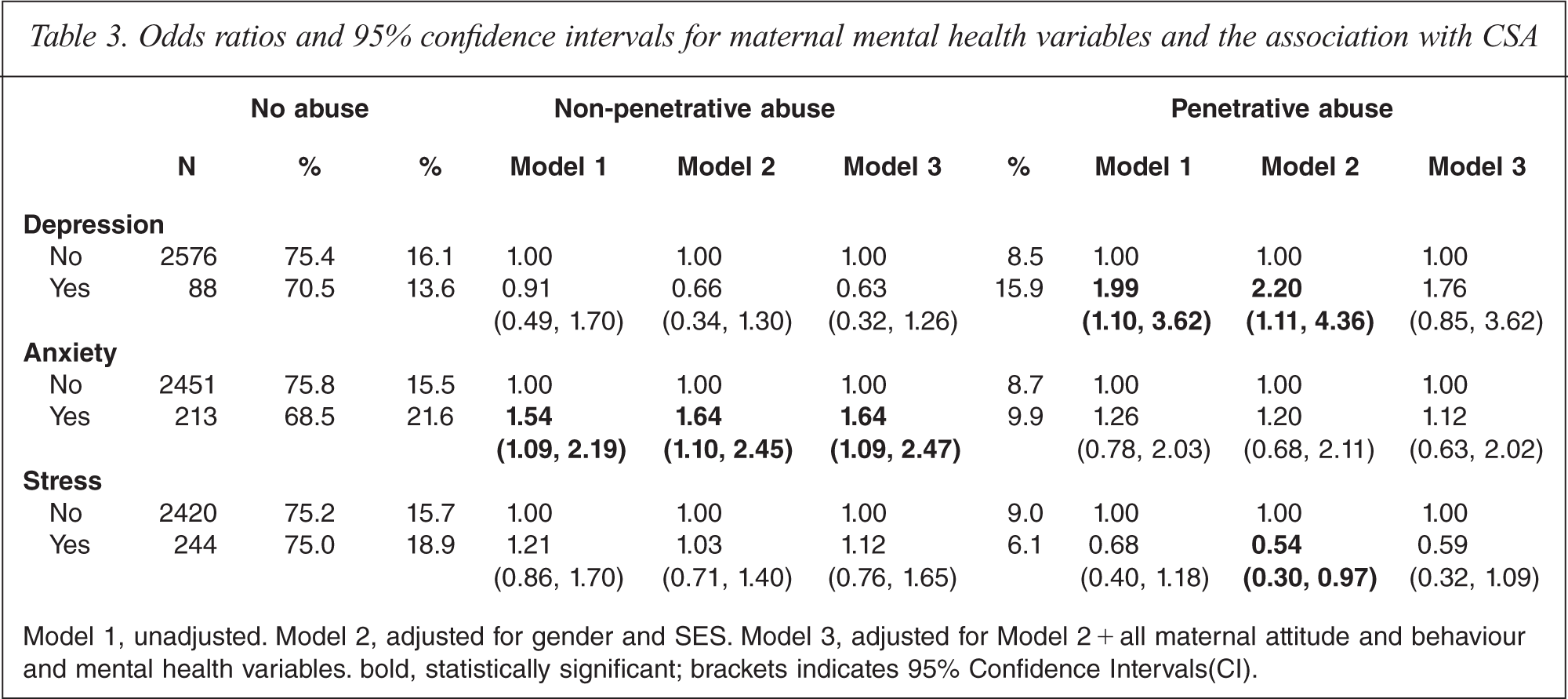
Model 1, unadjusted. Model 2, adjusted for gender and SES. Model 3, adjusted for Model 2 + all maternal attitude and behaviour and mental health variables bold, statistically significant; brackets indicates 95% Confidence Intervals(CI).
Footnotes
Acknowledgements