
Abstract
In the developed world in the last few decades there has been a decreasing number of psychiatric patients requiring long-term management in mental hospital settings and a significant move towards increased community care. This deinstitutionalisation has occurred for a number of therapeutic, humanistic and economic reasons [1]. First, there has been a natural progression towards deinstitutionalisation because of increasingly effective symptom control with better medication available and the development of a range of community-based services. Second, there has, in some situations, been an interventionist deinstitutionalisation process due to the recognition of the negative effects of institutionalism and liberal legal reform acknowledging the rights of the mentally ill. Finally, decentralised financial accountability for service delivery has enabled mental health treatment in the local normalised social environment.
Deinstitutionalisation has not proceeded without criticism, largely founded in diverse standards of planning, community care and socioeconomic resources [2,3]. In the USA, it has resulted in major homelessness and other social problems for the mentally ill, such as victimisation, neglect, stigma and violence [4,5]. In Italy, the lack of sufficient empirical data made it difficult to assess the effects of the introduction of Italian Public Law No. 180 upon mental hospitals [6,7]. In retrospect, problems predominantly arose in these countries as there was no unified or integrated system of deinstitutionalisation and the need has since been stressed for appropriate discharge planning, comprehensive community services, adequate funding, accommodation, access to social services, case management, continuity of care and evaluative research [8].
In the UK deinstitutionalisation has been occurring in the context of a national health service, providing organised community care in particular regions where there has been extensive evaluation of the process (for example the Team for the Assessment of Psychiatric Services or TAPS study [9,10]).
In Australia, the National Mental Health Strategy recommends the provision of care in the least restrictive setting. Actualising this ethos, the deinstitutionalisation of long-stay psychiatric hospital patients was planned in a Sydney mental health service. Comprehensive community care, accommodation, 24-hour supervision and funding were provided. This is the first of three papers (the other two are published in this journal [11,12]) reporting the detailed clinical, economic and ethnographic evaluation of this deinstitutionalisation. This plan was one important factor contributing to the closure of a large, long-stay psychiatric hospital in Sydney.
Method
The process of the deinstitutionalisation
The deinstitutionalisation plan was part of a New South Wales State Government initiated rationalisation of psychiatric services in a service area of Sydney. This plan involved the ‘amalgamation’ of two psychiatric hospitals (i.e. closure of one hospital) with the provision of funding to enable transfer of an initial 40 long-stay patients to the community. The hospital that eventually closed cared for some 217 long-stay mentally ill patients at the beginning of the study.
An independent committee of hospital and community staff identified patients who were both willing and suitable to transfer to the community. These patients were unlikely to have transferred to the community but for the planned closure. Only patients aged between 16 and 65 years, with a diagnosis of a serious mental illness and a continuous hospitalisation period exceeding 2 years were considered. In addition, patients were only included if they had not manifested any major behavioural problem, drug and alcohol problem, physical aggression or suicidality in the previous 2 years. From a social perspective, wherever possible, patients who were friends were to transfer to the same residence. Interested relatives of the patients were also consulted.
The community residences were designated for a continuing process of deinstitutionalisation. Vacancies due to either readmission or a move to more independent accommodation were only filled by long-term patients from the hospital.
The community setting
Four community residences with 10 beds per residence, were established in different subareas of the mental health service. The four residences comprised three community houses and one cluster of three-bedroom apartments. The community houses were situated on large suburban blocks and contained single and twin-share bedrooms with communal kitchen and dining areas. The apartment block held four self-contained units. All the residences were fully furnished and offered indoor and outdoor recreational areas and facilities. Each residence was supplied with a vehicle and residents had easy access to shops and public transport which were within walking distance.
Community care management
An adaptation of assertive community treatment was the model for community care [13]. This system of management stresses normalisation, treatment in the residential setting, intensive case management and 24-hour access to services.
Residents accessed local medical services such as the general practitioner, dentist and pharmacist who liaised with the community team on a shared-care basis. Psychiatric medical management, community rehabilitation programs and crisis intervention were provided by the subarea community mental health service. Respite care in community service accommodation and short-term hospitalisation were locally available when treatment was required outside the residential setting.
A multidisciplined team provided 24-h staff supervision and consisted of nurses and a psychologist, a social worker, an occupational therapist or a combination of these services. A number of staff transferred with the patients from the hospital to the community residences. The staff at each residence developed their own management policies and reported to the area community mental health service. Domestic services were required at various times at different residences and were provided by residential care assistants, cooks and cleaners. Over time, the level of staffing was reduced from the initial level of two per 8-h shift to one per shift, with additional staff allocated according to the daily schedule. Towards the end of the 2-year study period, 24-h supervision had in some cases been reduced and replaced with daily visits and 24-h telephone contact for staff assistance.
An intensive case management system operated at each residence. Case managers developed individual programs with the resident to address particular needs. The programs were monitored and varied according to each resident's progress. Programs ranged from one-on-one assistance for basic living skills (e.g. hygiene, cooking, shopping) to planning for more independent living (e.g. budgeting, self-administration of medication, acquiring sheltered or supported work). Techniques included prompting, modelling, task analysis, practical assistance and education. Case managers also ensured that residents had access to resources available from social services, educational facilities, community services and non-government organisations.
Residents were encouraged to pursue daytime activities and vocational programs were developed with case managers. Depending on their interest and capability they could attend the community mental health centre day program, community clubhouse activities, sheltered or supported work or general courses available to the wider community such as church groups, leisure activities and adult education courses.
The sample
An initial group of 40 long-stay patients transferred from the hospital to the community. During the first 18 months seven residents were permanently readmitted to the hospital and one resident died from unrelated medical causes. Additional patients transferred from the hospital to the community when vacancies arose. A total of 47 patients transferred to the community over the study period.
The criterion for successful transition to the community was a 2-year community tenure. There were seven replacements for the permanently readmitted patients of whom three had completed a 2-year follow up in the community by the end of the research project. The remaining four patients were still in the community, but had been there for shorter periods. The clinical evaluation will be reported on the 35 subjects who completed the 2-year follow up in the community and the seven subjects who were permanently readmitted to hospital.
Outcome measures
The major aim of this study was to assess the patients' clinical outcome over the 2 years post-discharge. The clinical measures used include the Brief Psychiatric Rating Scale (BPRS) [14], the Life Skills Profile (LSP) [15], the Social Behaviour Schedule (SBS) [16], the Montgomery Asberg Depression Rating Scale (MADRS) [17] and a Quality Of Life index (QOL) (available from the authors).
The QOL index assessed the residents' satisfaction with themselves, their futures and various aspects of their lives on a five-point rating scale. Areas covered in this measure were accommodation, residential policies, personal safety, food, clothing, money, mental health services, vocational and leisure activities, social and community contacts, love life and privacy.
Apart from the QOL, the measures were all informant-rated by case managers. Training and supervision in the completion of outcome measures were provided by the project (CH) researchers and a researcher from the study project (CH) administered the QOL. These data were collected in the month prior to discharge and then post-discharge at approximately 3, 9, 18 and 24 months. Levels of neuroleptic medication was also measured from discharge through the 2-year period.
Statistical analysis
Repeated measures linear regression using MLwiN version 1.02 [18] was utilised to model BPRS, LSP, SBS, MADRS and QOL outcome measures together with levels of neuroleptic medication. Such models, also known as multilevel or hierarchical models, consider repeated observations (level 1) to be ‘nested’ within patients (level 2). This approach is useful for data with differing numbers of observations per patient. Time was centred on each person's own average time, such that each person's intercept was his or her average score for each variable. For each of the analyses, the fixed effect (slope) was tested using the ratio of the estimate to its standard error, which has a t-distribution (df = n patients − 1) [19]. The significance level α was set at 0.05.
Covariates were added as fixed effects to the linear regression models in order to explain outcome measure differences between patients. Covariates included demographic, treatment and case history characteristics. Neuroleptic drug dosage was included as a covariate with the average level over the time entered. Given the small sample size, each covariate was considered on its own. The statistical significance of each covariate was tested with a t-test (estimate/standard error) with degrees of freedom equal to n patients − 5 covariates − 1 [19]. The significance level a was set at 0.05 for each covariate.
Results
Demographic and case history profile
During the study period 47 patients transferred to the community and included 25 men and 22 women. A total of 83 per cent (n = 39) were Australian born, 75% were single (n = 35), with the remainder being either divorced, de facto or in a long-term relationship. Only 47% (n = 22) had completed secondary education. Some 17% (n = 8) had never had paid employment. Nineteen subjects were diagnosed as having chronic schizophrenia, 19 as having paranoid schizophrenia, eight with schizoaffective disorder and one with developmental disability. The mean age of onset of psychiatric disorder was 18 years (range = 5–40 years), their mean age at first admission to hospital being 21 years (range = 9–50 years), while the mean age at final discharge was 41 years (range = 25–64 years).
The mean total length of stay in hospital from first to final admission, was 12.9 years (range = 2–43 years) while the mean length of stay for their most recent admission was 8.2 years (range = 2–43 years). The mean number of admissions to psychiatric hospitals was 11.6 (range = 1–36 admissions). The average proportion of the patients' total life spent in hospital amounted to 31%, while the average proportion of life spent in hospital since first admission, was 65%.
Patients were excluded from consideration for community transfer if they had exhibited ‘dangerous behaviour’ or ‘active suicidality’ in the previous 2 years. Nevertheless, some 66% of these 47 patients had demonstrated suicidality in the past, while 81% had demonstrated some earlier violence. Indeed, 17% had a forensic history and 47% had in the past had a drug or alcohol problem. Finally, 34% reported a history of serious mental illness in the nuclear family, with 17% reporting a family history of schizophrenia.
Permanent readmissions
Seven of the original 40 patients who transferred to the community required permanent readmission to hospital. Five of the seven patients were permanently readmitted between the 3 and 9 months follow up, one patient was readmitted between the 9 and 18 months follow up and one patient was permanently readmitted between the 12 and 18 month follow up. Assessment was discontinued following readmission.
These seven readmitted patients were significantly more likely to be women compared to those continuing in the community (86% and 43%, respectively) (χ2 = 1.034, p < 0.05); their BPRS scores were significantly higher prior to discharge (means = 64.9 and 53.7, t = 2.1, p < 0.05) and at 3 month follow up (means = 67.4 and 54.3, t = 2.1, p < 0.05). Similarly, they were on somewhat higher mean doses of neuroleptic medication prior to discharge (1668 mg and 1127 mg per day chlorpromazine equivalents) and at 3 months (1775 mg and 1204 mg) although these differences failed to reach statistical significance. On other measures they did not differ significantly. Physical aggression was a major factor in the decision to readmit in five of the seven patients, and the other two patients were readmitted due to severe behavioural problems.
Temporary readmissions
Excluding medical or surgical admissions, 37% (n = 13) of the 35 patients who successfully remained in the community setting for 2 year experienced at least one temporary readmission. Two subjects had two temporary readmissions each. The average length of readmission was 8 days (range = 1–71 days). The reasons for temporary readmission included florid psychosis, medication review, clozapine trial (which necessitated hospitalisation), physical or verbal aggression, self-harm and increased behavioural problems.
Outcome measures
The patterns of change in outcome measure over time are presented in Table 1. The results for demographic, treatment and case history covariates entered into the model are compiled Table 2.
Patterns of change in outcome measures over 2 years of community living
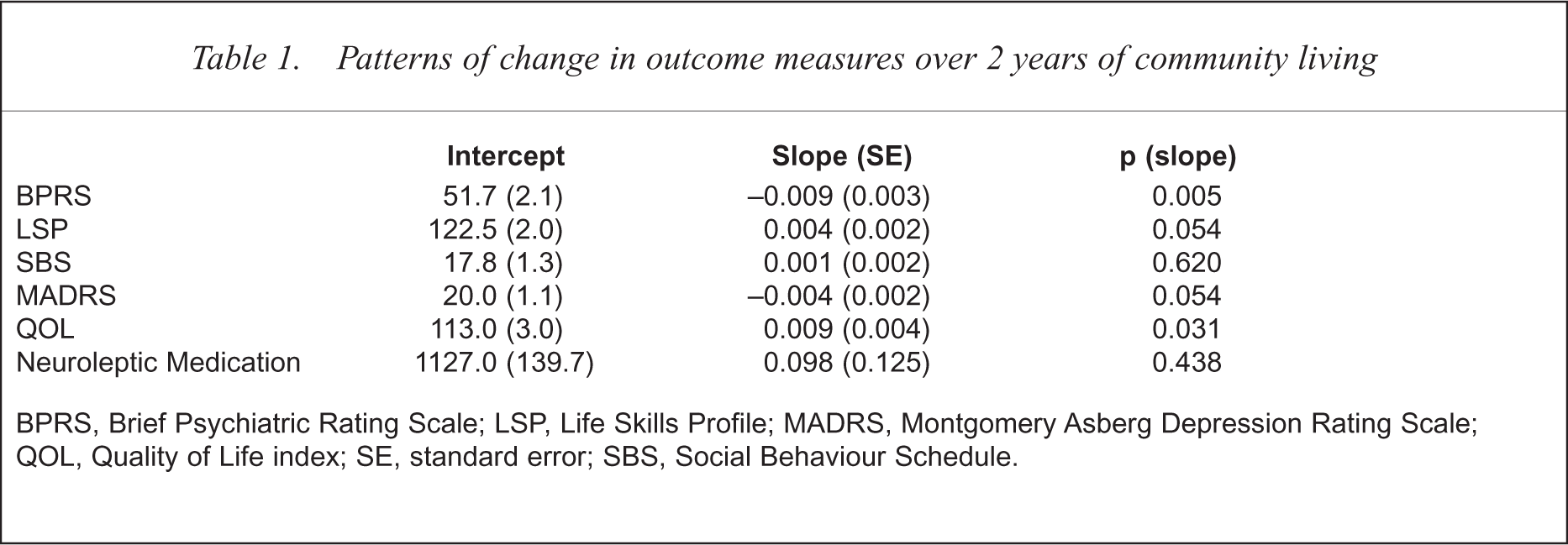
BPRS, Brief Psychiatric Rating Scale; LSP, Life Skills Profile; MADRS, Montgomery Asberg Depression Rating Scale; QOL, Quality of Life index; SE, standard error; SBS, Social Behaviour Schedule.
The effect of demographic, treatment and case history characteristics on clinical outcome measures
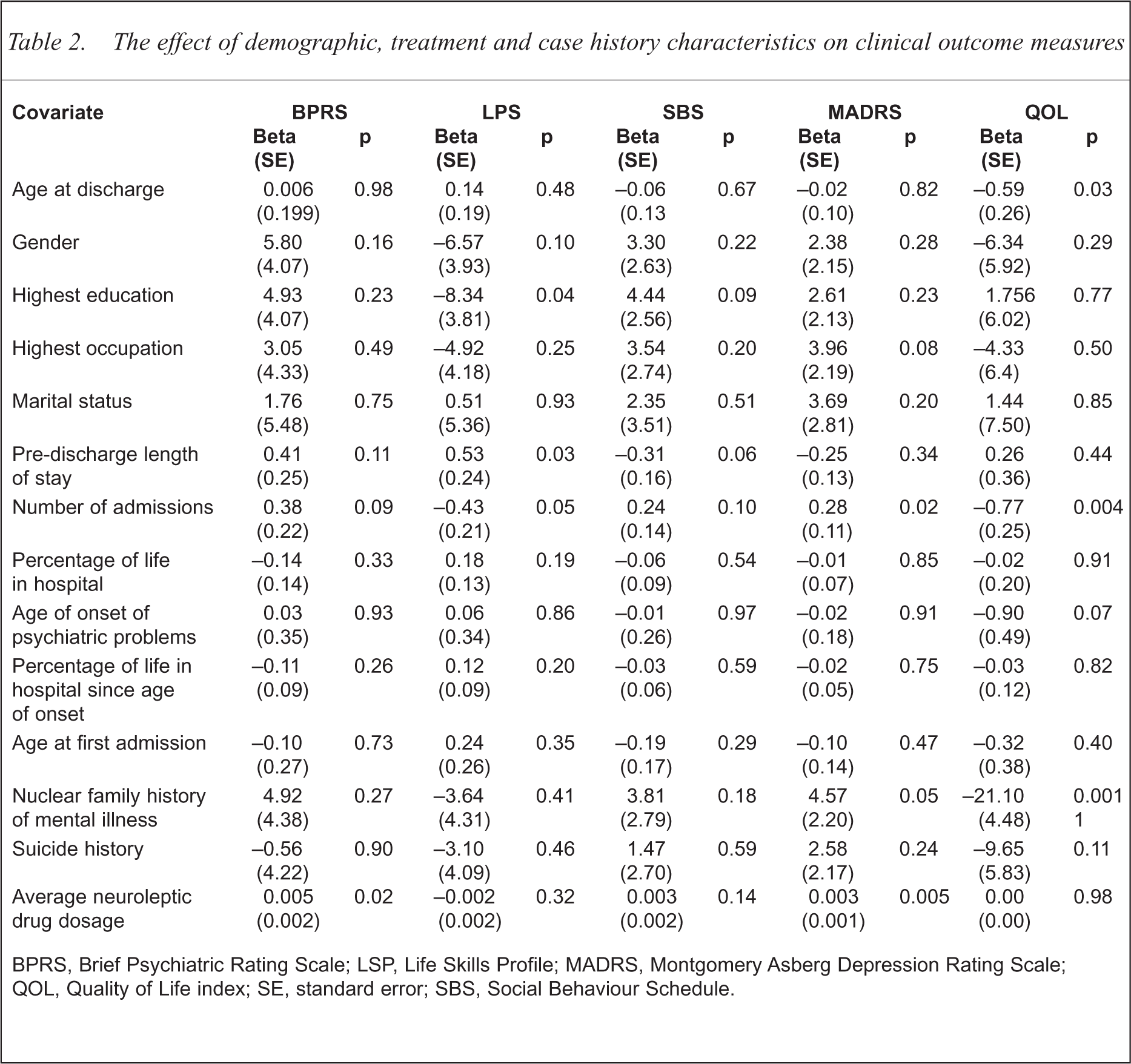
BPRS, Brief Psychiatric Rating Scale; LSP, Life Skills Profile; MADRS, Montgomery Asberg Depression Rating Scale; QOL, Quality of Life index; SE, standard error; SBS, Social Behaviour Schedule.
Brief psychiatric rating scale
Two years of community living resulted in a significant reduction in psychiatric symptoms (t = −0.009/0.003, p = 0.005). The only covariate associated with average differences in BPRS scores was the average level of neuroleptic medication. As would be expected, residents with more severe psychiatric symptoms received larger doses of neuroleptic medication (t = 0.005/0.002, p = 0.02).
Life skills profile
Although living skills did improve over the 2 years, the result was not significant (t = 0.004/0.002, p = 0.054). Some aspects of psychiatric history were associated with average LSP scores. Residents with lengthier predischarge periods in hospital (t = 0.53/0.24, p = 0.03) and residents with only primary as opposed to secondary school education (t = −8.34/3.81, p = 0.04) were more proficient at attending to daily living tasks.
Social behaviour schedule
Social behaviour problems remained unchanged over the 2-year follow up (t = 0.001/0.002, p = 0.62) and no significant effects of covariates were detected on SBS scores.
Montgomery Asberg Depression Rating Scale
Depression scores in general declined over the 2 years although the finding was not significant (t = −0.004 0.002, p = 0.054). Mood state was found to be associated with past psychiatric history. Residents who had experienced more numerous admissions to hospital (t = 0.28/0.11, p = 0.02) had higher levels of depression. More depressed residents also received larger doses of neuroleptic medication (t = 0.003/0.001, p = 0.005).
Quality of life
As opposed to the informant-rated outcome measures, there were varying amounts of missing data in this measure. Four residents were unable to participate in any interviews as they were either mute (n = 1), could not comprehend the questions (n = 1) or found the interview process disturbing (n = 2). Some residents (n = 13) were unwilling to participate in all of the repeated interviews due to lack of interest, answering the questions on previous interviews or being suspicious of the interview. A total of 65 per cent of residents with incomplete QOL data had a paranoid illness. Use of multilevel modelling, which has been demonstrated to be effective for the analysis of unbalanced data [20], allowed for the analysis of all available QOL data. The QOL was completed for 30 residents at predischarge, 29 at the 3-month, 22 at 9-month, 24 at 18-month and 22 residents at the 2-year follow up.
The 2 years of community living resulted in an overall significant improvement in QOL (t = 0.009/0.004, p = 0.03). There were, however, some significant negative influences on QOL from past psychiatric history. Residents who were older at discharge (t = −0.59/0.26, p = 0.03), had experienced a greater number of admissions (t = −0.77/0.25, p = 0.004) or had a nuclear family history of mental illness (t = − 21.10/04.48, p < 0.001) were generally less satisfied with their lives.
Pharmacotherapy
The mean doses of neuroleptic medication (in chlorpromazine equivalents) at predischarge, 1-year and 2-year follow ups were 1127 mg, 1204 mg and 1050 mg per day respectively. There were no significant differences in the average level of medication over the 2 years (t = 0.098/0.125, p = 0.44).
Of the 35 patients, five were on clozapine prior to discharge (mean dose = 390 mg, range = 170–750 mg), at 1 year 6 patients were on clozapine (mean dose = 517 mg, range = 300–750 mg) and at 2 years 10 patients were on clozapine (mean dose = 725 mg, range = 300–900 mg) (dosages in parentheses are daily amounts). Given that at different times of assessment, different proportions of patients were at varying stages of their clozapine administration, it is not relevant to compare mean doses at these three assessments.
Further independence
In the second year following hospital discharge, three residents moved to smaller group homes where staff supervision was on a daily visit basis with 24-h telephone cover. By the end of the study period, other residents had expressed a desire for a more independent lifestyle and were on waiting lists for similar group homes or registered with the Department of Housing for accommodation.
Discussion
It was anticipated that the move into the community and the significant pressures of change in lifestyle and accommodation would exacerbate psychiatric symptomatology. This did not occur. There was, in fact, a significant improvement in BPRS scores over the 2-year period. Although residents with more severe psychiatric symptoms tended to be maintained on higher doses of medication, these symptom improvements occurred without significant increases in the overall level of neuroleptic medication. Depression, however, did not significantly alter. A number of residents with a history of numerous admissions had a predisposition towards depression which contributed to this finding.
Living skills did not significantly change over the 2 years. Intuitively, the accomplishment of living skills can be related to a practical need to attend to daily duties in the community and the level of individualised staff assistance to accomplish these tasks. Variation in living skills proficiency was associated with the duration of predischarge rehabilitation and level of education. Although many residents still required assistance with living skills after 2 years, some residents had improved to the point where they were moving to less intensively supervised group homes. While the decrease in depression scores and the improvement in living skills scores were not statistically significant, the small sample may have contributed to the failure to reach statistical significance.
The lack of improvement in SBS scores was of interest. After establishing themselves in their new accommodation, the patients became more involved in wider community activities. There was greater pressure placed on their social behaviours in a more challenging environment. The persistence of problematic behaviours found in this and other studies [21–23] over 1, 2 and 5 year follow ups reinforces the need for continuity of care. A 5-year follow up has been commenced to track both community and readmitted residents' progress following this initial 2-year transition period.
Living in the community enhanced residents' life satisfaction. This occurred even though many residents expressed the desire to move to more independent accommodation by the 2-year mark. Lower levels of satisfaction associated with being older at discharge, having more admissions or having a family history of mental illness appeared to be related to perception of lost opportunities.
There is concern about lack of sensitivity to change in QOL measures [24]. This has been attributed to inclusion of symptom and social performance ratings in some measures [25]. Our QOL measure, an attitudinal measure of life satisfaction, avoided this problem. The lower response rate to QOL assessment leads to the possibility that the finding may be biased towards more favourable outcome, as the least satisfied may have been more likely to be nonresponders. Indeed residents with paranoid illnesses were less likely to respond. Our ethnographic paper [11] also reports improvement in life satisfaction that all residents experienced. Qualitative evidence of improved satisfaction is pertinent for those unable to complete all the quantitative QOL interviews.
Despite a comprehensive predischarge assessment, seven residents required long-term readmission. In comparison with those who continued to live in the community, this group exhibited factors found to be associated with failure to resettle in the TAPS study [26]. Readmission was precipitated by aggression or extreme behavioural problems and these patients had more severe psychiatric problems and were on higher levels of neuroleptic medication at predischarge and 3-month follow up. An unexpected finding was that a significantly greater proportion of those readmitted to hospital permanently were women and not men as in the TAPS study.
There were limitations to the design imposed by clinical considerations and resources. Patients were not randomised but were placed after meeting eligibility criteria and being agreeable to transfer. While most long-stay patients might be suitable for community care [27] our patients were given some choice. This study was therefore pre–post not case–control.
The patients had a history of being ‘difficult to place’ and had experienced prolonged hospitalisation. The majority had spent most (65%) of their adult lives in psychiatric hospitals. If not for the planned deinstitutionalisation, they would have remained in hospital. The clinical improvements support the community transfer of individuals with long-term mental illness when planned with adequate resources, comprehensive community psychiatric services, quality housing, rehabilitation programs and access to mental health care on a 24-h basis. Our economic and ethnographic papers detail the economic advantages of managing patients in the community and the advantages of community living experienced by residents.
Acknowledgements
Funded by the Commonwealth Department of Health and Family Services – Research and Development Grants Advisory Committee (RADGAC) and the Northern Sydney Area Health Services (NSAHS). We thank residents, relatives, hospital and community staff and management, for their assistance.