
Abstract
Delirium is a neuropsychiatric disorder characterized by disturbances of consciousness, attention, cognition, and perception with an abrupt onset and fluctuating course. Delirium usually has an underlying physiological etiology [1].
Delirium is a common event in the course of hospitalization, depending on the age of the patient and the severity of the illness. In a general hospital setting the occurrence of delirium may approach 30% in medically ill patients, 40% in the hospitalized elderly [2,3], and 85% in cancer patients and for those with terminal illness [4–6]. Upon admission to a hospital, 14–24% of elderly patients present with delirium and an additional 6–56% will develop delirium during the course of hospitalization [2]. Delirium is associated with poor functional outcome, prolonged hospitalization, and increased morbidity and mortality [7].
In addition to environmental interventions such as providing a safe and supportive environment, the guidelines for the management of delirium published by the American Psychiatric Association [8] recommend the use of typical antipsychotics, in particular haloperidol. However, with increasing frequency, practitioners select atypical antipsychotics as the initial somatic intervention for the amelioration of the symptoms of delirium [9]. Several studies suggest the efficacy and tolerability of atypical antipsychotics in providing relief from the distressing symptoms of delirium [10]. To date there is a single published case series and two published case reports examining the efficacy and tolerability of aripiprazole. Straker [11] reported on 14 patients with delirium who received aripiprazole. The results demonstrated that 12 out of 14 patients experienced a significant reduction (greater than 50% decline in delirium rating scores (DRS)) in their symptoms of delirium. Alao [12] reported two cases of delirium symptoms successfully ameliorated with aripiprazole (DRS: 28 to 6 and 18 to 6).
In order to further explore the efficacy and tolerability of aripiprazole, we performed a secondary analysis of patients with delirium who received aripiprazole and then compared this data to a case-matched sample of subjects treated with haloperidol.
Methods
Subjects
Subjects in this analysis included patients referred for delirium management to the Memorial Sloan Kettering Cancer Center (MSKCC) Psychiatry Service between July 2004 and June 2006. Clinical data including serial Memorial Delirium Assessment Scale (MDAS) ratings of delirium severity, Karnofsky Performance Scale (KPS) and Udvalg Kliniske Undersogelser Side Effect Rating Scale (UKU) scores, cancer diagnosis, medical conditions, all medications the patient received, potential etiologies of delirium, neuroleptics prescribed to ameliorate the symptoms of delirium, side effects and adverse effects attributed to the neuroleptic, and dose of neuroleptics were recorded in an Institutional Review Board (IRB)-approved Psychiatry Service clinical database.
Inclusion criteria were broad. Patients fulfilling the DSM-IV-TR [1] criteria for delirium were included. Exclusion criteria included patient or family objections to pharmacological intervention for the amelioration of the symptoms of delirium, inability to participate with delirium rating measures, severe agitation interfering with the interview, critical medical condition, or imminent death.
All patients and families provided verbal consent to be evaluated and receive neuroleptics for symptomatic relief of delirium. In patients with limited capacity to provide consent, the patient's primary caregiver provided verbal consent with the patient's ascent to intervention. All data were obtained from the routine care of patients diagnosed with delirium and entered into our IRB-approved database for subsequent analysis and a waiver obtained for the data analysis.
Measurements
Sociodemographic and medical variables were collected at the initial assessment. This information included age, gender, cancer diagnosis, stage of cancer (localized, advanced, metastatic or terminal), current psychiatric diagnosis, past psychiatric diagnosis, history of dementia, presence of brain metastases, and potential delirium etiologies.
Delirium severity was measured with the MDAS, a 10-item, four-point, clinician-rated scale [13]. The MDAS items reflect the diagnostic criteria for delirium in the DSM-IV-TR and assess disturbance in arousal and level of consciousness, cognitive functioning (memory, attention, orientation, and perceptual disturbances) and psychomotor activity. MDAS scores greater than 10 identified the presence of delirium and MDAS scores of 10 indicated the resolution of delirium in this analysis [14]. As proposed by Meagher, the categorization of delirium was based on the motoric subtype, hyperactive or hypoactive [15–17]. Additional scales included the Karnofsky Scale of Performance Status [18] to provide a measure of physical performance ability and an abbreviated version of the Udvalg for Kliniske Undersogelser Side Effect Rating Scale to measure side effects of neuroleptics [19].
Procedures
Data on cancer diagnosis, cancer stage, presence of brain metastases, delirium etiology, history of dementia, and sociodemographic data were collected at initial diagnosis of delirium (T1). MDAS and KPS, as well as side-effect rating were performed at initial diagnosis of delirium (T1) and repeated at 2–3 days (T2) and 4–7 days (T3). After seven days the observation period ended and patients continued on medication if necessary.
The treatment of delirium guidelines published by the American Psychiatric Association recommend (i) the identification of underlying etiologies, (ii) appropriate medical intervention to treat reversible etiologies, (iii) initiation of environmental interventions to provide safety and support, and (iv) relief of distressing symptoms with neuroleptics [8]. The psychiatrist providing the initial diagnosis of delirium selected which neuroleptic to prescribe to the patient. If the patient was receiving a neuroleptic at the time of initial diagnosis of delirium, this neuroleptic was discontinued and an alternative neuroleptic was selected. Patients in this analysis received either aripiprazole or haloperidol. We permitted all patients to receive haloperidol as needed for severe distress or agitation. We recorded as needed doses of haloperidol administered to the patient (and included this in the analysis). If the patient demonstrated worsening delirium by clinical observation or by MDAS scores, the current neuroleptic was discontinued and an alternative neuroleptic initiated. (We recorded ineffective relief provided by neuroleptic and included this in the analysis).
Sample characteristics
We identified 21 patients treated with aripiprazole and 32 patients treated with haloperidol in our delirium database. In order to provide comparable samples we case-matched the haloperidol patients to the aripiprazole patients by age, history of dementia, initial MDAS scores and subtype of delirium. The unsampled HAL patients were significantly younger and had higher initial MDAS scores than the sampled HAL patients.
Statistical analysis
Analyses of the database were performed with the SPSS 16 statistical software package for Windows. The sample was not normally distributed regarding MDAS and KPS scores and nonparametric tests were used. For multiple related measures the Friedman test was used, for pair-wise comparison of related samples the Wilcoxon test, for pair-wise comparison of independent samples the Mann-Whitney U test, and for categorical variables Fisher's exact test was used. Exact tests were used when possible.
Results
Sample characteristics
We retrieved 21 subjects from our delirium database treated with aripiprazole. The mean age of the patients was 69.6 (36–85, SD 11.9) years and was not significantly different from the case-matched 21 subjects treated with haloperidol with 64.0 (36–79, SD 11.7). Cancer diagnoses and etiologies were diverse in both groups and did not significantly differ; the number of potential etiologies contributing to delirium did not significantly differ between the two groups: ARI 4.9 (3–7, SD 1.0) and HAL 4.8 (3–7, SD 1.1). The mean initial MDAS scores did not significantly differ between the groups: ARI 18.1 (11–25, SD 4.3) and HAL 19.9 (12–25, SD 3.4). Hypoactive and hyperactive delirium were equally distributed among the two groups. Hypoactive delirium presented in nine patients (42.9%) and hyperactive delirium presented in 12 patients (57.1%). The KPS score at baseline was significantly higher in ARI patients at 28.1 (20–40, SD 6.8) compared to 22.4 (20–30, SD 4.4) in HAL patients (Mann-Whitney U: 118.5, Z = −2.9, p < 0.01).
Treatment characteristics
The mean initial aripiprazole dose was 15.2 mg and the mean observation termination dose was 18.3 mg. The mean haloperidol doses at the same observation time points were 4.9 mg and 5.5 mg respectively (Table 1). Over the course of treatment, MDAS scores declined from 18.1 at baseline to 10.8 at T2 and 8.3 at T3 in ARI patients (Friedman: chi square 31.87, df = 2, p < 0.001) and from 19.9 at baseline to 9.9 at T2 and 6.8 at T3 (Friedman: chi square 38.3, df = 2, p < 0.001) in HAL patients. There was no significant difference in the MDAS scores of ARI and HAL patients at T2 and T3. Resolution of delirium symptoms did not differ significantly between ARI and HAL patients at either subsequent observation point. KPS scores improved from 28.1 at baseline to 35.2 at T2 and 41.0 at T3 in ARI patients (Friedman: chi square 20.11, df = 2, p < 0.001) and 22.4 at baseline to 28.1 at T2 and 31.9 at T3 in HAL patients (Friedman: chi square 20.83, df = 2, p < 0.001). Differences between ARI and HAL at T2 and T3 were not significant.
Characteristics of aripiprazole (ARI) and haloperidol (HAL) in the treatment delirium and its motoric subtypes
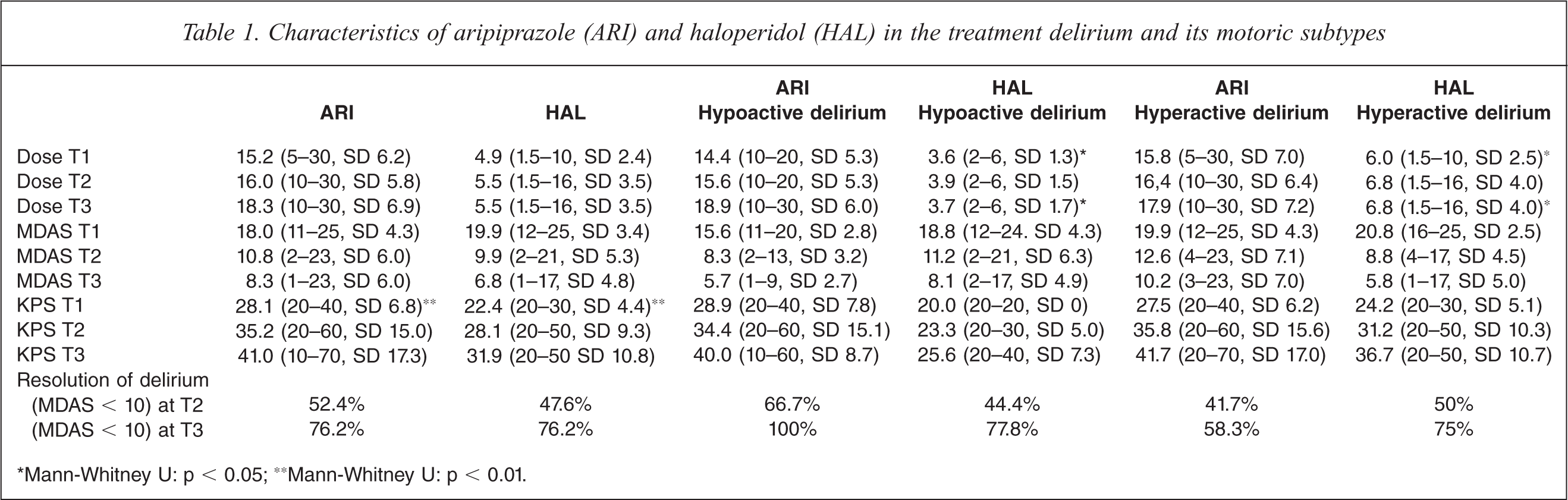
*Mann-Whitney U: p < 0.05; **Mann-Whitney U: p < 0.01.
Treatment characteristics of the motoric subtypes of delirium
Aripiprazole
In ARI patients with hypoactive delirium MDAS scores improved from 15.6 at T1 to 8.3 at T2 to 5.7 at T3 (Friedman: chi square 16.91, df = 2, p < 0.001). In ARI patients with hyperactive delirium MDAS scores improved from 19.9 at T1 to 12.6 at T2 to 10.2 at T3 (Friedman: chi square 15.27, df = 2, p < 0.001). We were unable to demonstrate a significant difference in the MDAS scores of ARI patients with hypoactive delirium compared to hyperactive delirium. Patients with hypoactive delirium experienced 66.7% resolution of symptoms at T2 and 100% at T3. Patients with hyperactive delirium experienced less successful amelioration of symptoms: 41.7% of patients obtained relief of symptoms at T2 and 58.3% of patients achieved resolution of symptoms. From our analysis, aripiprazole less effectively relieves the symptoms of hyperactive delirium than the symptoms of hypoactive delirium (Fisher exact: p < 0.05). The dose of aripiprazole administered to patients with hypoactive delirium did not differ significantly from that administered to patients with hyperactive delirium at T3.
Haloperidol (HAL)
In HAL patients with hypoactive delirium, MDAS scores improved from 18.8 at baseline to 11.2 at T2 to 8.1 at T3 (Friedman: chi square 16.19, df = 2, p < 0.001). In HAL patients with hyperactive delirium, MDAS scores improved from 20.8 at baseline to 8.6 at T2 to 5.8 at T3 (Friedman: chi square 22.29, df = 2, p < 0.001). There were no significant differences in MDAS scores between patients with hypoactive or hyperactive delirium at T2 and T3. Patients with hypoactive delirium who received haloperidol experienced 44.4% resolution of symptoms at T2 and 77.8% resolution of symptoms at T3. For patients with hyperactive delirium, 50% experienced resolution of symptoms at T2 and 75% achieved amelioration of symptoms at T3. Delirium resolution rates did not significantly differ in patients with hypoactive and hyperactive delirium receiving haloperidol. Patients with hyperactive delirium received a significantly higher dose of haloperidol than those patients with hypoactive delirium. At time points T1 and T3 patients with hyperactive delirium received 6.0 and 6.8mg of haloperidol compared to 3.6 and 3.7mg of haloperidol in patients with hypoactive delirium (T1 Mann-Whitney U: 23.0, Z = −2.3, p < 0.05 and T2 Mann-Whitney U: 25.5, Z = −2.0, p < 0.05).
Aripiprazole in comparison to haloperidol
MDAS scores of patients that received aripiprazole did differ significantly from MDAS scores of patients that received haloperidol at time points T2 or T3. There was no significant difference in the ability of aripiprazole to ameliorate the symptoms of delirium more effectively than haloperidol at time points T2 and T3 in either subtype of delirium, hypoactive or hyperactive.
Side effects
No extrapyramidal side effects (EPS) were encountered attributable to the treatment of delirium with aripiprazole in contrast to 19% of patients experiencing EPS with haloperidol. In patients who received haloperidol, Parkinsonism occurred in 19.0% and dystonia in 9%. Patients with hyperactive delirium who received significantly higher doses of haloperidol experienced EPS with greater frequency.
Discussion
Our analysis indicates that aripiprazole, an atypical antipsychotic, previously described in case series and case reports, may have comparable efficacy to haloperidol, the current recommended pharmacological intervention for the amelioration of the distressing symptoms of delirium.
The mean observation termination dose in patients treated with aripiprazole was 18.3 mg (10–30), similar to Alao's case report (15 and 30 mg aripiprazole) and higher than in Straker's case series with a mean of 8.9 mg (5–15 mg) aripiprazole. In our aripiprazole-treated sample MDAS scores declined significantly in delirium and its motoric subtypes. Interestingly, the delirium resolution rates were significantly higher in the hypoactive subtype. This may be in part due to the fact, that in subjects with hyperactive delirium the number of patients with prior cognitive deficits were higher (n = 4) compared to subjects with hypoactive delirium. Within the subject group with hyperactive delirium prior cognitive deficits were associated with a limited treatment response.
In this analysis, aripiprazole did not differ significantly in treatment effects from haloperidol. Aripiprazole and haloperidol were equally effective in providing relief from symptoms of delirium. Aripiprazole demonstrated an advantage in tolerability by the absence of extrapyramidal side effects. Approximately 19% of patients who received haloperidol experienced extrapyramidal side effects. The patients who experienced EPS were more likely to have the hyperactive subtype of delirium and severe agitation, and subsequently required significantly higher doses of haloperidol to achieve symptom control. In comparison, the dosing of haloperidol necessary to achieve symptomatic relief of hypoactive delirium was significantly lower. No patient in this group suffered EPS. Review of our data suggests that dosing regimens of haloperidol to achieve effective amelioration of the symptoms of delirium may be adjusted based on subtype of delirium present. The analysis of our aripiprazole data did not demonstrate differences in dosing requirements to achieve symptomatic relief of delirium differentiated by subtype.
Overall the treatment results of aripiprazole in the management of delirium are promising in comparison to the current recommended pharmacologic intervention, haloperidol.
Although the data collection has strengths including systematic evaluation and documentation of etiologies contributing to the delirium, differentiation of subtype of delirium present whether hypoactive or hyperactive, indication of severity of medical illness through KPS scores, and observation and recording of side effects, several important limitations are noted.
Our analysis is based on a retrospective analysis of prospectively collected data. Selection of neuroleptic intervention was based on psychiatrist's preference. Comparison of aripiprazole to haloperidol required us to case-match patients. Severely agitated patients were excluded from our analysis. The total number of patients included in the analysis was limited to 21 in each medication group.
Further investigations, particularly double-blind, randomly assigned, controlled designs of atypical antipsychotics and typical antipsychotics would be ideal to assess the results of our current analysis.
In summary we demonstrated that there was no difference in efficacy between aripiprazole and haloperidol in the amelioration of the symptoms of delirium. Treatment with haloperidol resulted in a higher rate of extrapyramidal symptoms for patients.
Footnotes
Acknowledgements