
Abstract
Keywords
Numerous studies have demonstrated negative community attitudes towards people with mental illness [1], and public health initiatives have been undertaken in an attempt to reduce stigma [2]. Stigma amongst clinicians has received less attention, despite the possible impact on the quality of medical care received by the mentally ill.
People with chronic mental illnesses such as schizophrenia tend to receive worse medical care than other patients. For example, individuals with comorbid mental disorders, especially those with psychosis, are significantly less likely to undergo coronary revascularization procedures after myocardial infarction than people without mental disorders [3,4]. It has been suggested that physician bias may contribute to the poorer care received by the mentally ill [3].
People with schizophrenia have high rates of medical comorbidity [5] and premature mortality [6]. They are likely to require care for chronic illnesses such as diabetes, as well as presenting with acute events such as myocardial infarction. It is important that they are treated with equal respect and concern, and have access to the same quality of medical treatment, as members of the community who are not mentally ill.
Rao et al. [7] surveyed health professionals, including doctors, and found highly stigmatized attitudes towards the mentally ill. Even within mental health services, stigma is evident [8]. Nordt et al. [9] found no difference between mental health professionals and members of the public in their attitudes to people with schizophrenia.
We decided that an intervention to reduce negative attitudes towards people with schizophrenia would be most effective in the final year of the medical course, proximal to students moving to different hospitals and taking on clinical responsibilities as an intern. Whilst initiatives to reduce stigma have generally consisted of educational programmes, there is evidence that contact interventions providing interaction with a person with mental illness may be more effective [10]. Corrigan et al. [11] found that a videotape showing a person talking about his mental illness (considered a contact intervention) was more effective than an educational videotape in improving the attitudes of community college students. Similarly, Mann and Himelein [12] found that a humanizing approach, which included exposure to first person narratives about mental illness, was more effective than didactic teaching in improving the attitudes of psychology students.
Simulated hallucinations can provide a more direct experience of psychosis. A virtual reality environment simulating psychosis has been developed [13] but such a facility would not be widely available for teaching purposes. A self-guided tour of an environment simulating psychosis has been constructed in Second Life, an Internet-based virtual reality world, and has been positively evaluated by users [14].
The use of simulated auditory hallucinations for teaching purposes has been described in studies involving medical [15] and nursing [16] students. A range of different methods and outcome measures were used. Bunn and Terpstra [15] found that mean empathy scores on the Jefferson Scale of Physician Empathy [17] improved after medical students had listened to 40 min of recorded hallucinations via mp3 players, whilst simultaneously participating in cognitive tasks then walking around the medical centre. However, students who had low empathy scores at the beginning of the session had even lower scores post-test. Nursing students who undertook an orientation session at a mental health site and then listened to a 45-min tape of auditory hallucinations had greater improvement in scores on the Medical Condition Regard Scale [18] than students not exposed to the simulated hallucinations [16].
In contrast, a study by Brown and colleagues [19] found that exposure to 16 min of simulated hallucinations delivered using a portable CD player led to an increase in stigma, measured using the Attribution Questionnaire [20]. After the intervention, psychology students were less likely to help and interact with people with mental illness and were more in favour of enforcing treatment for the mentally ill. Brown et al. [21] also compared listening to an audio segment of 16 min of simulated auditory hallucinations with a contact intervention, a 16-min film about a person with schizophrenia. Stigma was measured using the Social Distance Scale [22] and the Affect Scale [23]. The contact intervention was effective in reducing stigma on both measures, whilst participants (psychology students) who listened to simulated hallucinations preferred greater distance from people with mental illness and had more negative emotions towards these people after the intervention.
We designed a workshop for final year medical students that included both contact and experiential components. Our goal was to develop an effective, practical intervention that could be incorporated into the ongoing teaching programme.
Methods
Participants
This study was conducted with University of Adelaide final year medical students during their 6-week psychiatry rotation. A total of 87 students participated in the study. Of the participants, 63% (n = 55) were female. All participants gave written informed consent. Approval was obtained from institutional research and ethics committees.
Procedures
After giving written informed consent, participants completed the AMIQ [24]. They then watched and discussed the 40-min contact DVD. Next, they watched a 10-min segment of a TV show in which a well known presenter participated in a simulated hallucination workshop at a mental health conference.
Students then worked in pairs. For 45 min, one student listened to simulated hallucinations delivered via an mp3 player, at a conversational volume. The students completed a range of tasks together. After 45 min they swapped roles.
At the end of the workshop there was a period of general discussion and feedback. Participants completed the AMIQ and wrote a reflective paragraph describing their experience of the workshop.
Interventions
Contact DVD
The DVD is about a young university student who develops schizophrenia. He describes his illness well, and is engaging and likeable. Despite his chronic illness, he is able to continue working and maintain a strong social network.
Simulated hallucinations
The negative studies of simulated hallucinations [19,21] involved 16 min exposure, whilst the duration of exposure in the positive studies was 40–45 min [15,16]. Our simulated hallucinations therefore lasted for 45 min. The studies cited above have all used simulated hallucinations developed by the National Empowerment Centre [25]. We developed our own simulation with voices with Australian accents, as we anticipated that the American voices developed by Deegan [25] would seem like listening to television for our Australian students, and would be easily ignored. Our voices did not include derogatory, suicidal or homicidal content.
Measures
The 5-item AMIQ is a brief self-administered questionnaire. Participants respond to a short fictional vignette describing an individual who suffers from schizophrenia. Each question is scored on a 5-point Likert scale (maximum +2, minimum −2) with ‘neutral’ and ‘don't know’ being scored 0. The score for the five questions was added giving a total score between −10 and +10. Lower scores indicate more negative attitudes.
Results
Results of a paired sample t-test showed a significant improvement in the student's attitudes to people with schizophrenia following the workshop. Their mean AMIQ score improved from −1.7 (SD = 2.7) prior to the workshop to −0.62 (SD = 2.7) after the workshop (t(86) = −4.22, p < 0.001).
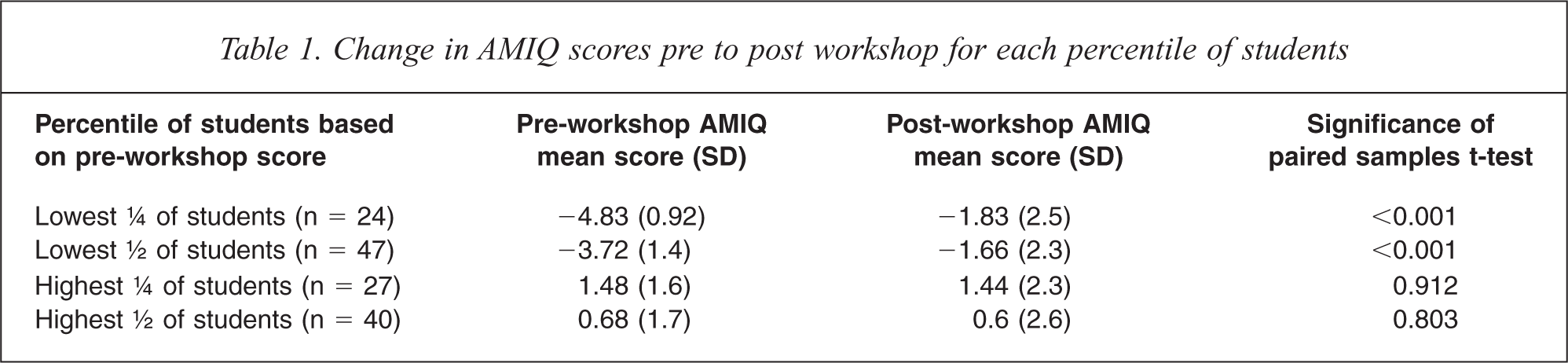
We divided participants into percentiles, based on baseline AMIQ scores. It is apparent that the increase in mean scores is due to improvement by students with lower baseline scores (see Table 1).
Change in AMIQ scores pre to post workshop for each percentile of students
Gender
A mixed ANOVA revealed no significant gender difference in the change in scores over time (Wilks Lamba = 0.97, F(1.85) = 2.42, P = 0.123).
Reflections
Students found the workshop useful and described a better understanding of the everyday difficulties of living with chronic psychotic symptoms. Comments included:
‘Very good experience to gain an insight into how hallucinations influence the quality of life/daily functioning of a person with schizophrenia’ ‘I was not as chatty or interactive with my partner as I usually am…I was constantly distracted by the voices and found myself wanting to listen to them’ ‘Gives a good picture of how distressing it can be for schizophrenia patients.’
Discussion
The results of this study indicate that a workshop combining providing a personal account of schizophrenia with a simulated experience of auditory hallucinations is effective in improving medical student attitudes to people with schizophrenia. Interestingly, unlike Bunn et al. [15] we found that students with the most negative attitudes before the workshop improved, whilst those who had less stigmatizing attitudes showed little change. The workshop was positively received by the students and feedback indicated that it was a valuable experience. The simulated voices we used were less distressing than those used in other studies, but were still effective.
In considering why some studies using simulated hallucinations have had a negative effect on attitudes [19,21], it is apparent that in these studies the simulated hallucinations were not presented along with other educational material, with the expressed aim of helping students understand more about schizophrenia. As an isolated experience it is not surprising that a film, with a narrative and context, would be more effective than simply listening to simulated voices, which could be quite frightening.
On reviewing the previous studies in this area it is apparent that comparison between studies is confounded by the use of different measures. Empathy is not the same as lack of stigma. Further, the concept of stigma contains a number of elements [26], and the different rating scales sample these elements to varying degrees. Kassam et al. [27] have developed the Mental Illness: Clinicians’ Attitudes: Medical Student Version, but this scale also includes items measuring attitudes to psychiatry as a speciality. It would not be suitable for comparing the attitudes of different groups such as the general public or other health professionals. Some more general stigma scales take a positive response to items indicating that a person with this illness is more likely to drink too much, take illegal drugs, and be subject to discrimination, as evidence of stigma on the part of the respondent [28]. In the case of schizophrenia there is evidence that these statements are generally true. There is a need for a comprehensive rating scale, sensitive to change, and specific to schizophrenia.
The difference in results between those with low pre-scores and those with higher pre-scores requires further exploration. If our finding that students with negative attitudes benefit most from this type of workshop is replicated, this reinforces the need to develop these interventions further as part of the medical school curriculum. For example, helping students understand the experience of people with physical disabilities using experiential learning methods may be useful in countering the decline in empathy reported during medical training [17].
The results of this study are limited in that there was no comparison group. The AMIQ, as a self-report instrument, may not necessarily reflect behavioural changes, which may be better measured through observation. Although students were assured anonymity in their responses, social desirability bias may have affected the results.
These results indicate that improving medical student attitudes is possible, using a low cost, easily delivered intervention. If such interventions are more widely adopted as part of medical student training, and enhanced attitudes are shown to persist into clinical practise, then perhaps people with schizophrenia and comorbid physical illnesses will receive the same quality of medical care as other members of the community.
Footnotes
Acknowledgements