
Abstract
Keywords
The observation that schizophrenia patients often did not take their antipsychotic drugs was the first step in investigating subjective experiences. Medication non-adherence was linked to the occurrence of extrapyramidal symptoms, especially subtle akathisia, and to a dysphoric response to antipsychotics [1,2]. Non-adherence proved to be the most important risk factor for relapse of psychosis [3].
While generally accepted definitions of quality of life are lacking, researchers consider as determining factors: physical health status, daily life functioning, psychological status and subjective well-being, social interactions and support, economic status and external resources [4–6].
Subjective well-being is generally defined as ‘subjective experience, as constituting aspects of mental or physical state, which patients report regardless of etiological attributions’ [7]. Physicians and researchers cannot make reliable judgements about patients’ subjective well-being [8−10]. Distinguishing between patient's subjective experience and psychopathology proved to be difficult [7,9,11,12]. Affective, cognitive and reality distortion symptoms can disturb subjective assessments. Psychiatrists assumed that patients with schizophrenia could not reliably assess their own subjective well-being [5,13].
After the introduction of atypical antipsychotics, more research focused on measuring subjective experiences in schizophrenia patients. Since the 1990s, several studies have shown that the majority of patients with schizophrenia (63–95%) are able to complete self-rating scales reliably and consistently [7,8,12,14,15]. Subjective experience became an independent outcome measure relevant for adherence and recovery [11,16,17].
Assessment of subjective well-being
Illness-specific quality of life instruments are more sensitive to treatment effects than generic scales [18–20]. There are a number of schizophrenia-specific quality of life instruments available [19].
In early research several observer-rated scales were developed, e.g. the Drug Response Index (DRI), Neuroleptic Dysphoria Scale (NDS), Quality of Life Scale (QLS) and Subjective Deficit Syndrome Scale (SDSS) [21–24]. In assessing subjective well-being, self-rating scales are preferred over expert ratings [9]. As patient perspective became more relevant, self-rating instruments were more frequently used: Drug Attitude Inventory (DAI), Rating of Medication Influences (ROMI), Subjective Well-Being under Neuroleptic Treatment (SWN), Personal Evaluation of Transitions in Treatment (PETiT), Schizophrenia-Quality of Life (S-QoL) [25–29]. Several of these instruments were not originally developed for measuring subjective well-being or quality of life in its broader meaning. Consequently, comparability is difficult and research results are not easily interpreted.
Subjective Well-Being under Neuroleptic Treatment
The instrument mostly used in recent research on subjective experience of schizophrenia patients is the Subjective Well-Being under Neuroleptic Treatment scale [12,27]. Originally it was constructed as a 38-item self-report scale with 20 positive and 18 negative statements in six-point Likert scales referring to the last 7 days. The currently used 20-item version (SWN-K) consists of 10 positive and 10 negative items. Patients generally need 5 to 10 minutes to complete this short version. To calculate the total score and subscores, ten negatively formulated items have to be reversed. The total score ranges from a minimum of 20 (poor) to a maximum of 120 (excellent). Subjective experience is measured in five subscales: emotional regulation, self control, mental functioning, social integration and physical functioning [11].
In a study with the 38-item SWN, subscales correlated significantly with negative symptoms and global psychopathology, but not with positive symptoms and extrapyramidal side effects [27]. In another study with the 20-item SWN, subscales correlated modestly with the Positive and Negative Syndrome Scale (PANSS) positive subscale, correlations with negative and global PANSS scales were stronger. Correlations with the PANSS showed that less than 16% of the variance of any SWN subscale could be explained by any PANSS subscale. Subjective well-being could not be reliably predicted by psychopathological measures [11].
An estimated 5% to 20% of schizophrenia patients are unable to understand the items and cannot reliably fill in the form [3], whereas most acutely psychotic patients are able to use the SWN [27]. The psychometric properties are good. Internal consistency measured with Cronbach's alpha ranges between 0.79 and 0.96. In several studies, reliability measurements have been replicated, also in different languages [7,12,30,31]. The SWN is translated into more than 40 languages. The SWN has shown to be sensitive to medication change [7,12]. It is a useful tool in detecting patients at risk for non-adherence and provides an independent outcome measure [11,27]. In recent research, the SWN was considered a quality of life instrument [32].
The SWN is used in RCTs, double blind controlled studies and clinical trials in different patient populations including adolescents, patients with chronic and recent onset illness, outpatients and hospitalized patients (Table 1). Recently, a 10-item and a 5-item scale have been constructed without considerable loss of validity. The correlation between the 10- and 5-item SWN was 0.967 [33].
Clinical trials using the SWN
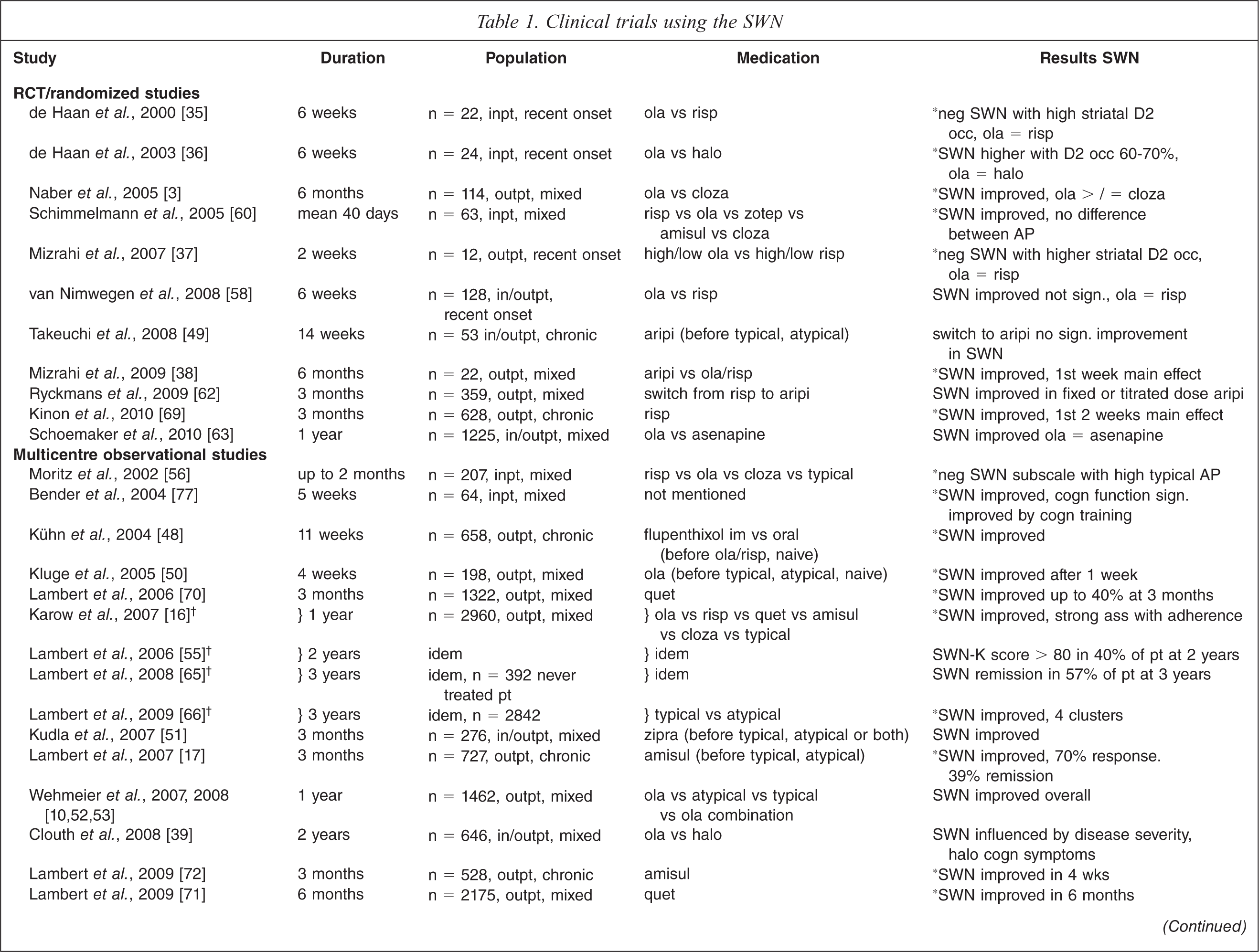
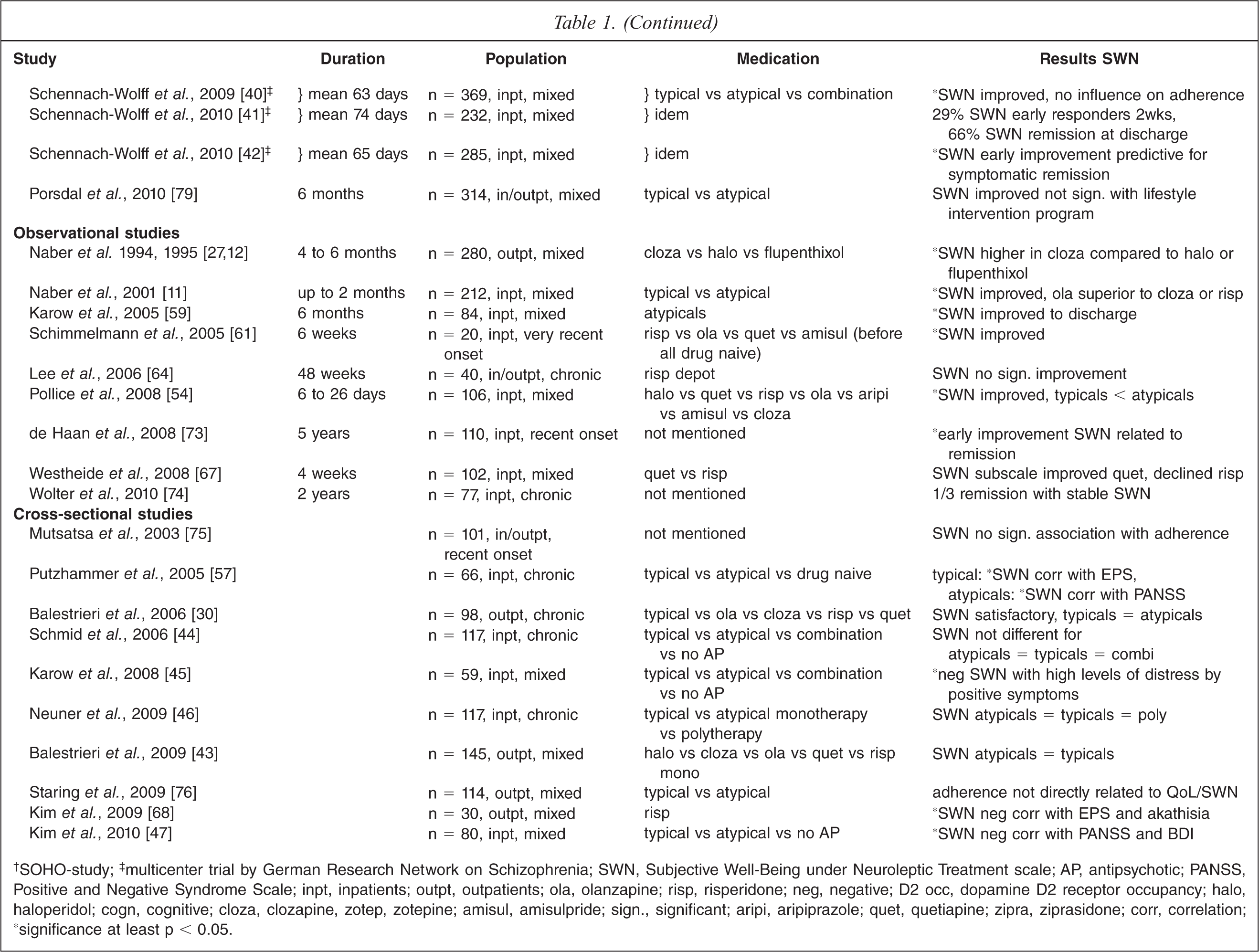
†SOHO-study;‡ multicenter trial by German Research Network on Schizophrenia; SWN, Subjective Well-Being under Neuroleptic Treatment scale; AP, antipsychotic; PANSS, Positive and Negative Syndrome Scale; inpt, inpatients; outpt, outpatients; ola, olanzapine; risp, risperidone; neg, negative; D2 occ, dopamine D2 receptor occupancy; halo, haloperidol; cogn, cognitive; cloza, clozapine, zotep, zotepine; amisul, amisulpride; sign., significant; aripi, aripiprazole; quet, quetiapine; zipra, ziprasidone; corr, correlation; ‘significance at least p < 0.05.
Aim of this review
Research findings of subjective well-being in schizophrenia patients are inconsistent due to different concepts of quality of life and different questionnaires, used in different populations. Therefore, interpretation and comparison are difficult [34].
The aim of this review is to analyse all available publications on relevant research using the SWN, in order to evaluate measuring of subjective well-being in schizophrenia patients with a single instrument.
Method
A MEDLINE and Embase search was performed for studies published between January 1994 and August 2010, and references. Keywords were: ‘Subjective well-being under neuroleptic treatment, SWN, subjective well-being, subjective experience, schizophrenia, psychosis’. We selected original publications written in English, German or Dutch clinical trials using the SWN. Review articles were excluded. We found 52 publications covering 44 clinical studies using the SWN in a schizophrenia population.
Results
Table 1 shows all relevant publications of 44 clinical trials using the SWN in schizophrenia: 11 RCTs, 14 multicentre, nine observational and ten cross-sectional studies.
SWN and D2 occupancy
Several studies were performed on the influence of different medication and dopamine D2 receptor occupancy on subjective well-being using PET or SPECT scans.
De Haan et al. [35] assessed subjective well-being, psychopathology, extrapyramidal symptoms and D2 receptor occupancy with [123I]IBZM SPECT in 22 stabilized schizophrenia patients using olanzapine or risperidone. Researchers were blind to clinical outcome. Negative subjective well-being, depression (r = 0.46, p = 0.02) and negative symptoms (r = 0.45, p = 0.02) correlated with high D2 receptor occupancy, but extrapyramidal symptoms did not.
In a randomized double-blind study these findings were confirmed [36]. A total of 24 adolescent patients with recent onset schizophrenia were randomly assigned to receive olanzapine 7.5 mg or haloperidol 2.5 mg for 6 weeks. Subjective well-being, psychopathology and extrapyramidal symptoms were assessed at baseline and endpoint. After 6 weeks the striatal D2 receptor occupancy was assessed with [123I]IBZM SPECT. Subjective well-being improved significantly in the haloperidol group, with a mean occupancy of 65.5% (p = 0.004). In the olanzapine group neither superior subjective response nor superior efficacy to haloperidol was measured, and the mean D2 receptor occupancy was 51%. The researchers concluded that a D2 receptor occupancy between 60–70% was significantly associated with optimal subjective well-being (p = 0.004).
Mizrahi et al. [37] performed a double-blind controlled study to examine the relationship between striatal and extrastriatal dopamine D2 receptor binding potential and adverse subjective well-being. Twelve patients with recent onset psychosis were randomly assigned to low and high doses olanzapine (2.5 mg or 15 mg daily) or risperidone (1 mg or 4 mg daily). Subjective well-being, motor side effects, and striatal and extrastriatal dopamine D2 receptor binding were evaluated after 2 weeks of continuous antipsychotic treatment. [11C]raclopride and [11C]FLB 457 positron emission tomography (PET) scans were used, respectively. Significant associations were found between SWN total score and high striatal blockade (r = −0.66, p = 0.01), and between SWN total score and high temporal blockade (r = −0.76, p = 0.003). Lesser blockades in the striatum, insular cortex, parts of frontal and temporal lobe were associated with greater feelings of well-being. There was no difference between patients taking olanzapine or risperidone and no association between subjective well-being and PANSS positive symptoms. Negative subjective well-being was found without overt motor side effects.
Recently, Mizrahi et al. [38] compared the effect of dopamine D2 occupancy produced by a partial agonist antipsychotic (aripiprazole) to that of antagonist antipsychotics (risperidone or olanzapine) on subjective well-being. The SWN score was related to dopamine D2 receptor occupancy using [11C]raclopride PET. Eleven patients switched to aripiprazole and showed a significant improvement in their subjective well-being mainly in the first week. This effect was sustained for 6 months and was observed despite very high levels of dopamine D2 occupancy (82–99%). In contrast, the subjective well-being of eleven patients using full antagonist antipsychotics was worse with higher ventral striatum D2 occupancy (57–89%).
SWN in relation to antipsychotic medication
Comparison between atypical and typical antipsychotics
Results of clinical trials on subjective well-being using typical versus atypical antipsychotics are contradictory.
There is evidence that subjective well-being improved with both typical and atypical antipsychotics. The importance of comparable dosages and optimal D2 receptor occupancy was shown in a randomized controlled SPECT study comparing olanzapine and haloperidol [36]. The level of D2 occupancy predicted subjective well-being with both medications. This level is associated with the dosage of antipsychotic medication. Improvement of subjective well-being was also found in observational studies, without significant differences in typical versus atypical treatment groups [10,39–42]. In studies with a cross-sectional design, subjective well-being in patients treated with atypical or typical antipsychotics was not different [30,43–47].
In one study switching from atypicals and starting medication-naive patients on flupenthixol improved subjective well-being significantly [48]. In another study switching typical and atypical antipsychotics to aripiprazole had no significant effect on subjective well-being [49].
Several multicentre and observational studies reported better subjective well-being with atypical antipsychotics than with typical medication [11,12,16,27,50–54]. Post-hoc analyses of the German sample of the Schizophrenia Outpatient Health Outcomes (SOHO) study showed that first-line treatment with an atypical antipsychotic increased significantly the likelihood of complete remission compared to typical antipsychotics [55] (see Definitions of remission and recovery below).
High dosages of typical antipsychotics (at least 400 mg chlorpromazine equivalent doses) were associated with negative subjective well-being [56]. The use of typical antipsychotics was also related to more extrapyramidal side effects and cognitive side effects, probably due to high dosages [39,56,57].
Comparison between various types of atypical antipsychotics
Research results comparing subjective well-being of patients treated with different atypical antipsychotics are inconsistent.
Subjective well-being as measured by the SWN improved in most studies. No difference was found in comparisons between olanzapine and risperidone [35,37,58] and other atypical antipsychotics [38,54,59–63]. In two studies switching to aripiprazole or risperidone depot did not improve subjective well-being [49,64].
In other comparative studies improvement of subjective well-being was most likely when patients used olanzapine [3,10,11,16,55,65,66], clozapine [3,16,55,65,66], quetiapine [67] or aripiprazole [62].
Monotherapy with atypical medication was related to improvement of subjective well-being regardless of the type of atypical antipsychotic agent; risperidone [68,69], olanzapine [50], quetiapine [70,71], amisulpride [17,72] or ziprasidone [51].
SWN as a predictor of outcome
Definitions of remission and recovery
Recently, a consensus was reached about definitions of schizophrenia remission and recovery with symptomatic, functional and combined criteria [65,66,72].
Symptomatic remission (at least 6 months) or recovery (at least 24 months) was defined as achieving a CGI-SCH score of no worse than ‘mild’ in assessments of overall severity, positive, negative and cognitive sub-scores and no hospitalization in the respective time period [65,66].
Functional remission or recovery was defined as a fulfilment of three criteria: (i) paid or unpaid full or part time employment or being an active student or head of a household with employed partner; (ii) independent living, alone or with peers or partner; and (iii) social relationships with more than two contacts in the last 4 weeks or having a spouse [65,66].
Subjective well-being (SW) response was defined as an improvement of at least 20% and at least 10 points in SWN-K total score from baseline. SW early response was defined as a SWN-K total score improvement of at least 20% and at least 10 points within the first two treatment weeks [17,42]. SW delayed response occurs within the first 4 weeks [72]. The criterion of adequate subjective well-being or SW remission was met with SWN-K total score > / = 80 points [10,17,65,66].
Complete remission was defined as combined symptomatic, functional and SW remission [65,66,72].
Improvement of symptoms
Subjective well-being was repeatedly found to be influenced by psychopathology. In several studies high symptom severity was correlated with negative subjective well-being [10,17,39,41,42,52,53,57,59,72]. However, some studies found a relatively weak association between symptom severity and subjective well-being [3]. Subjective well-being was influenced by anxiety [59,71], depression [35,47,59,71], negative [3,12,17,35,56,57,59,60,72] and positive symptoms [3,16,17,45,59,60]. Subjective distress in patients with side effects did not correspond to clinicians’ severity ratings [61].
Early improvement of subjective well-being was predictive for long-term symptomatic remission in first episode schizophrenia patients, whereas early improvement in severity of symptoms was not [73]. In several studies subjective well-being improved during the first weeks [38,42,50,58,69,72,73]. Early SWN responders showed significantly more improvement in clinical status and functioning compared to early non-responders [50,69]. Early response in subjective well-being and social functioning predicted overall outcome significantly better than response in positive or negative symptoms [17,55,72,73]. Patients with severe schizophrenia can have a delayed response within 4 weeks [72].
Low subjective well-being, severe negative symptoms and neurological side effects at baseline, as well as enduring positive symptoms were predictive for low subjective well-being and non-adherence later on [41,42,60,61].
Clusters of subjective well-being
Four clusters of subjective well-being were identified in large studies (European SOHO, External Assessment of Quality of Life in Out-Patients with Schizophrenia (EASE)) [53,66]: patients with stable high SW, stable moderate SW, stable low SW and improving SW. The group of stable low subjective well-being accounts for approximately 30% of the study population in different trials [17,66] and the improving cluster for approximately 20% [53,66].
In the SOHO study predictors for the stable low cluster were a low baseline SWN-K score, a long duration of illness and no recovery at 3 months. The early improvement cluster was predicted by symptomatic recovery at 3 months and good functioning at baseline [66].
In the EASE study predictors for improving SW cluster were absence of treatment with oral antipsychotics in pre-study and no medication change due to lack of efficacy at baseline. For the low SW cluster change of medication due to lack of efficacy and high CGI-S scores were predictive [53].
Cut-off scores for the SWN-K with good predictive value were found for the stable high cluster (SWN-K baseline score >80) and the stable low cluster (SWN-K baseline score <60). These scores can be used for early outcome prediction and treatment planning [66].
Remission
Remission and recovery rates in post-hoc analyses of the SOHO study, an outpatient population, were between 47% and 60% for symptomatic criteria, 27% and 45% for functional criteria and 42% and 57% for adequate subjective well-being. Complete remission was reached by 13% and 28% of the patients [55,65].
In a recent study of inpatients, symptomatic and functional remission occurred only in 10%. Approximately one third of the patients reached SW remission but none complete remission [74]. In a multicentre inpatient study 66% of patients fulfilled the criteria for adequate subjective well-being and 29% were early responders within 2 weeks [41]. Symptomatic response was reached by 81% and symptomatic remission by 48% of the patients [42]. Baseline SWN-K scores, PANSS global subscore, side effects and educational status were found to be predictive of adequate subjective well-being. Concerning symptomatic remission SF-36, SWN-K baseline scores and SWN-K early improvement showed significant predictive value [41,42].
SW response at 4 weeks was predicted by subtype of schizophrenia (paranoid or disorganized), lower severity of illness, and fewer negative symptoms. SW remission at 12 weeks was predicted by SW response, fewer negative symptoms and better functioning at 4 weeks [17]. Overall, remission and recovery was mainly predicted by the functional status at baseline and early remission of the three outcome measures (symptomatic and functional status and subjective well-being) at 3 months [65].
Quality of life
In the EASE study correlations between subjective and objective assessments were strong when measured by the SWN and the Quality of Life Scale [52]. A linear correlation was found between improvement of QLS and SWN-K [10,52,69]. The SWN seemed to be more sensitive for medication change than the QLS [10]. In the acute phase, correlations between QoL and PANSS were only low to moderate [59].
Recently, different self-rating scales were studied in relation to subjective quality of life. The SWN particularly correlated highly with the WHO-QoL suggesting that subjective well-being and quality of life as measured with these two scales are comparable [32]. In cross-sectional and longitudinal studies subjective well-being and quality of life scales are moderately congruent [52,59,66,72].
Adherence
Results of studies associating subjective well-being with medication adherence are inconsistent and differ across study designs and patient populations.
In several studies no influence of subjective well-being on adherence was found, not in first episode patients nor in long-term follow up [40,73,75,76]. Predictors of positive attitude towards adherence were reduction of psychopathology [40,76], employment [40], greater illness insight [40,75] and treatment with atypical antipsychotics [40]. Substance misuse and adverse side effects showed no significant association with adherence [40,75]. Only Staring et al. [76] reported high adherence to be associated with more adverse medication effects as indicated by the SWN.
On the other hand, strong associations of subjective well-being with adherence were found. Subjective well-being was a substantial predictor of mid-term adherence with antipsychotic medication in first- and multiple episode patients of the SOHO study [16,55,65,66]. In this study which lasted 12 months, adherence was 1.4 times higher when SWN scores increased by 20 points. Changes in positive symptoms and extrapyramidal symptoms were also associated with adherence [16]. In another study [12] non-adherent patients had significantly worse SWN-K scores than those adhering to treatment. These studies indicated that subjective well-being can be a major predictor of adherence, with considerable implications for relapse, rehospitalization and long-term clinical outcome [3,11,70].
Determinants of SWN
According to Wehmeier et al. [53] the broad range of determinants predicting quality of life can be classified into three groups: patient-related predictors; illness-related predictors; and treatment-related predictors.
Patient-related determinants
Patient-related parameters predicted subjective well-being poorly. Older patients seemed to be less satisfied in some studies, patients with an occupation, higher educational status and an active coping style report better subjective well-being in other studies [10,41,42,44,54].
Illness-related determinants
For illness-related parameters, results are diverse. In general, a more severe illness, more positive and negative symptoms, depression, anxiety and hostility correlated with negative subjective well-being [references under 3.2]. Lambert et al. found differences between subtypes of schizophrenia, the subtype of schizophrenia was of influence; paranoid and disorganized subtypes correlated with positive and the residual type with negative subjective well-being [17,70]. Other studies could not find a correlation [61,73]. Despite similar severity of psychopathology, significant differences in SWN-K scores were found between schizophrenia (57.7), schizoaffective disorder (64.1) and bipolar disorder (79.5) [71].
Illness duration, smoking and coffee use were not related to subjective well-being in several studies [11,36,44,56,60,72]. Less craving for cannabis improved subjective well-being in one study [58]. Improvement in subjective well-being was significantly greater in first-episode patients than in multiple-episode patients [70].
Treatment-related determinants
Treatment-related parameters are most often investigated in research comparing typical and atypical medication, reviewed above. The use of atypical antipsychotics is associated with better subjective well-being [3,10,11,16,30,35,36,50,51,54,56,58–60]. However, typical antipsychotics improve subjective experience also [10,30,36,48,54]. Extrapyramidal side effects influence well-being in a negative way [37,39,54,57,68] and other side effects worsen subjective experience too [16,59,60,67]. Change in medication is correlated with negative subjective well-being, probably due to a more serious illness or treatment resistance [12,53].
Cognitive therapy had a positive effect on subjective well-being [77], whereas lifestyle intervention had no influence [78]. There are indications that a longer hospitalization [54], involuntary admission [44], lower psychosocial functioning [17,51] and higher care giver's burden as experienced by the patient [44] correlate with lower subjective well-being.
Six prospective studies of patients with recent onset psychosis [35–37,58,61,73] and seven prospective studies of chronic psychotic population [17,48,49,64,69,72,74] were analysed. There are indications that high dosages of medication give more side effects in recent onset patients. Drug naive patients seem to be more sensitive to side effects than chronic patients with a history of medication use [61].
Most clinical trials had a study duration up to 6 months. Several studies reported a longer follow-up [39,53,63,64,66,73,74]. De Haan et al. [73] demonstrated that early improvement of subjective well-being in recent onset patients was related to remission at 5 year follow up. Treatment of a chronic population with risperidone depot during 48 weeks showed no significant improvement of subjective well-being [64].
Discussion
In reviewing the literature on subjective well-being in schizophrenia, we limited our search to studies using the SWN scale in order to avoid conceptual problems and improve comparability. The SWN is the most widely used scale to measure subjective well-being and has good psychometric properties. No substantial differences were found in subjective well-being as measured by the long (38-item) or short (20-item) version of the SWN. Recently developed 10- and 5-item versions can be time saving instruments for future clinical use [33,79].
Comparability remained limited due to differences in objective, methods, design and study population. The available data are not suited for quantitative analysis. Nevertheless, the findings of randomized controlled trials and observational studies lead to similar conclusions. The key finding is that subjective well-being of patients with schizophrenia improved during treatment in almost all studies. The multicentre studies, funded by pharmaceutical companies, focused mainly on comparisons between medications. Most differences between antipsychotic medications, generally small, can be explained by dosage differences. An optimal dosage is more important than the kind of medication. Several studies have shown that a striatal dopamine D2 receptor occupancy between 60% and 70% correlates with positive subjective well-being of patients with schizophrenia. Higher occupancy of D2 receptors is correlated with negative subjective well-being and often with non-adherence [80–84].
Recently, Mizrahi et al. [38] found a significant improvement in SW, notwithstanding high striatal dopamine D2 occupancy by aripiprazole. A likely explanation is that, in contrast to full antagonists, this D2 partial agonist allows for physiological dopamine functions and better subjective experience despite high dopamine D2 occupancy [36,37,80,82,84,85].
In studies comparing atypical with typical antipsychotic medication, small differences in SWN scores in favour of atypical antipsychotics may be the result of more sedative and antidepressant and less extrapyramidal effects, next to dosage discrepancies. In several studies, dosages of typical antipsychotics are relatively high compared to dosages of atypical antipsychotics [86–88].
Cross-sectional studies failed to show differences in subjective well-being, probably due to their relatively low sensitivity as compared to longitudinal studies.
On the association of subjective well-being with psychopathology, research findings are ambiguous. In some studies PANSS scores correlate poorly with subjective well-being [9,10]. In other studies PANSS negative and global psychopathology correlate substantially with SWN scores [11,27]. Severe illness with more psychopathological symptoms is reported to be predictive for negative subjective well-being [45]. In several studies, early improvement of SWN predicted better clinical outcome [38,42,50,58,69,72,73].
The knowledge of predictors of subjective well-being is still poor and questions on causality are unsolved. The use of antipsychotic medication reduces psychotic symptoms which may increase subjective well-being, but can also increase adverse medication effects reducing subjective well-being [76].
Subjective welI-being is probably influenced by many variables. Recent onset patients appear to be more sensitive to higher dosages than chronic patients [81,87,88]. Acute schizophrenia patients with good understanding of their illness often report a lower subjective well-being, possibly because these patients are more aware of the consequences of their mental illness [45]. Patient characteristics such as personality, self-esteem, cognitive functioning and differences in metabolism and neurotransmission may influence subjective well-being as well as social support, objective life circumstances, therapeutic interventions and other environmental parameters [34,59,89–91]. These are important factors to consider in further investigations, particularly in prospective studies. New research developments focus on genetic dispositions of subjective well-being [92].
Clinical implications
In schizophrenia, subjective well-being improves with antipsychotic medication.
Optimal dopamine D2 receptor occupancy is associated with better subjective well-being.
Early improvement of subjective well-being is predictive for the long term outcome of schizophrenia.
The SWN-K is a useful tool for prediction of response and subsequent recovery.
Footnotes
Acknowledgements
The authors alone are responsible for the content and writing of the paper.