
Abstract
Schizophrenia and schizoaffective disorders are defined by DSM-IV [1] in terms of characteristic symptoms and social or occupational dysfunction. Diagnostic perspectives focusing on symptoms and global assessments of functioning have traditionally been used by clinicians, vocational professionals and researchers to assess, explain and predict vocational impairments [2]. Subjective experiences and consumer perspectives of occupational impairment are seldom utilized [3] despite a long-standing recognition that residual states of illness encompassing subjective experiences, even without characteristic symptoms of schizophrenia, are relevant to longer-term social recovery [4], [5].
Nature and origin of subjective experiences
Huber et al. [4] differentiated three categories of schizophrenia remission. One, a ‘pure defect syndrome’ was found to comprise residual syndromes and subjective complaints not specific to schizophrenia with no positive or negative symptoms, prevalent in 43% of discharged patients. A second, a mixed residual syndrome (prevalence 34%) included characteristic symptoms, contrasted with a third category, complete remission (22%). Subjective complaints included: cognitive disturbances; mental and physical exhaustion; disturbances of well-being; exaggerated impressionability; hypersensitivity to noise and weather; sleep disturbances; and decreased initiative, energy, drive and endurance.
Hatfield [6] identified four types of inner experiences as frequent sources of stress for people with schizophrenia: struggling with inner experiences of altered perceptions; cognitive confusion; attention deficits; and impaired identity. Similarly, Liddle and Barnes [7] observed psychological deficits not specific to schizophrenia, including loosening of associations, flattening of affect, impaired concentration and anhedonia. Although of limited diagnostic value, and possibly transient in nature [8], these deficits are likely to have an influence on social and occupational adjustment.
Employment-restricting subjective experiences may also result from impairments in social functioning [9], neuroleptic side-effects [10] and negative subjective responses to neuroleptics [11]. These could be exacerbated by prevalent substance and poly-substance misuse [12], where substance misuse can be reactive to the subjective distress of auditory hallucinations [13]. Subjective experiences encompass common life experiences shared with the wider community as reflected in the use of nonillness terminology such as ‘out of step with the rhythm of life’ [14].
Subjective experiences and employment functioning
The social cognitive career theory [15] provides a relevant framework for explaining career development among people with serious mental health disorders. In this theory, personal characteristics, illness characteristics, and environmental factors (e.g. family background, social/cultural context) combine to shape individual career learning experiences both in terms of availability of performance opportunities, and self-assessment of performance and expectations of success. Career learning experiences influence efficacy beliefs which in turn have reciprocal effects on behaviour. Hence, subjective experiences which impact on expectations of successful task performance, influence self-efficacy and career learning experiences. Self-efficacy represents a person's perceived capability to execute an action. Hence it is likely that subjective experiences perceived to impair work functioning are mediated by impairments to self-efficacy [16], [17]. This is an important conceptual link to the established empirical relationship between self-efficacy and vocational performance [17–20].
Subjective experiences perceived to impact on employment are likely to arise at the intersection of individual characteristics, diagnostic symptoms, and work performance expectations. Such subjective experiences are likely to reveal more about the nature of an individual's specific employment restrictions than information derived from a diagnostic perspective alone. This view is consistent with the proposal that inner experiences act as mediators between cognitive dysfunction and behaviour [21] and that cognitive impairments underlie subjective experiences, sometimes rendering work unduly stressful [22]. These proposals are consistent with the findings that individual employment experiences are idiosyncratic, affected in complex and interrelated ways by individual characteristics and circumstances [23], and that subjective and meaningful work experiences lead to recovery and improvements in self-concept and selfefficacy [24].
Psychometric properties of subjective measures
Subjective experiences can be validly and reliably measured. For instance, Bitter et al. [25] found adequate internal consistency and construct validity for the Subjective Deficit Syndrome Scale (SDSS), concluding that the measure helps elucidate why some clinically remitted patients continue to fail in social and occupational functioning. Selten et al. [26] found high test-retest reliability for the experience of disruption and distress in the Subjective Experience of Negative Symptoms (SENS) scale, derived from the Scale for the Assessment of Negative Symptoms (SANS [27]). Hamera et al. [28] examined symptom distress and symptom intensity statements from an expanded version of the Brief Psychiatric Rating Scale (BPRS [29]) concluding that in a residual phase of illness, self report is more valid for assessing positive and non-psychotic symptoms than for deficit symptoms.
Aims
The aim of the current study was to develop a selfreport scale of subjective experiences of illness perceived to impact on working as an alternative source of information to a diagnostic perspective for identifying the specific vocational assistance needs of people with schizophrenia or schizoaffective disorder. To our knowledge this is the first reported attempt to measure subjective experiences perceived to impact on employment while relating these to measures of illness severity and disability, and to employment outcomes among community residents with schizophrenia or schizoaffective disorder.
Method
Item pool
An item pool was created to represent seven symptom domains identified from the literature: (i) cognitive (including disorganization and confusion), 20 items; (ii) negative (including anhedonia), 16 items; (iii) attention and memory, 16 items; (iv) affective, 23 items; (v) delusional, 23 items; (vi) social, 22 items; and (vii) medication and drug usage, 11 items. Brief descriptors were derived from: the Test of Attentional Style [30]; the Frankfurt Questionnaire of Complaints [31]; the Subjective Deficit Syndrome Scale [25]; the Positive and Negative Syndrome Scale [32]; the Subjective Experience of Deficits in Schizophrenia [7]; the Subjective Experience of Negative Symptoms [26]; and the Mental Health Research Institute Unusual Perceptions Schedule [13]. Thirty additional descriptors were written to ensure each domain was adequately represented.
Pilot study
A card-sort and visual analogue scale (VAS) interview method was designed specifically for people with schizophrenia. Descriptors were presented on cards (9 cm × 6 cm). The approach was prompted by the method developed for assessing descriptions of auditory hallucinations [13]. Subjective experiences were rated using a visual analogue scale [33] to record relative severity, frequency of occurrence, manageability, and whether each would be a problem when employed.
Participants (n1 = 26) were recruited from local psychosocial rehabilitation and community mental health services. Inclusion criteria were: (i) a self-reported diagnosis of schizophrenia or schizoaffective disorder; (ii) not currently an inpatient or experiencing an acute episode; (iii) aged between 18 and 60 years; (iv) not known to have a severe intellectual disability or a severe head injury; (v) has provided informed consent; and (vi) can communicate sufficiently in English to complete interviews without assistance. People with secondary comorbid conditions such as anxiety, depression, and substance misuse, and people with no interest in vocational rehabilitation, were not excluded. The structured interview was repeated after 4 weeks and within 5 weeks for those who could be located (n2 = 21).
Item revision
New descriptors were created to represent any specific and plausible difficulties reported during the pilot study. Items frequently queried were modified or removed to improve face validity. The descriptor ‘Difficulty correcting my mistakes’ was added to capture error utilization [34], considered important for work performance. Face validity, stability, and responsiveness were examined in line with texts on scale development [35], [36]. Items were required to achieve medium responsiveness (endorsed by 20–80% of participants). Items were removed if stability could be explained by chance at 5% or more confidence. Items met this binomial distribution criterion where 68% or more participants consistently endorsed (or not) a particular experience after 28–35 days. Reliability of perceived impact on employment was estimated from Spearman correlations. Due to low statistical power (n = 21) this latter criterion did not exclude otherwise promising items. Variances were examined to identify items with particularly high standard deviations relative to estimate size.
It was considered important to reduce the item set to a manageable size for routine use. To achieve this, items were flagged for removal where the mean reported work confidence exceeded 60%. While this criterion ensured that items perceived to have a relatively strong impact on employment functioning were retained, a risk of excluding potentially useful items with a lesser perceived employment effect was introduced. On balance, this risk was considered outweighed by the need to reduce the item set to 50 items or less.
Perceptions of experienced professionals
Lack of insight and anosognosia, when present, can suppress subjective experiences and minimize impact on perceived capacity for employment [37–39]. To counter this possibility, the views of experienced allied mental health and vocational rehabilitation professionals were sought. Eleven experienced staff, defined as three or more years experience with psychiatric disability, attending a vocational rehabilitation seminar, independently rated 62 descriptors from the pilot study for perceived impact on the employment of a hypothetical consumer. Items with employment confidence ratings of 60% or higher were removed if similar self-ratings were obtained in the pilot study. The 42 items with the best properties were retained for use in the 12-month longitudinal study.
Recruitment to a longitudinal study
Participants were sought from the wider Brisbane metropolitan area bounded by Caboolture, Ipswich, and Tweed Heads South. Pilot study inclusion criteria were supplemented by a requirement for confirmation of DSM-IV [1] diagnoses of schizophrenia or schizoaffective disorder. Written informed consent was obtained from 111 people of whom 104 met baseline inclusion criteria. There were no refusals to provide informed consent, and no one who expressed an interest in participating was considered incapable of providing consent. One person exercised the right to withdraw from the study after completing the first interview.
Interviews and measures
Interviews were conducted by three registered psychologists experienced at interviewing people with psychoses. Interviews were repeated at 6 and 12 months, arranged at participants' homes or at a local service provider office, whichever the participant preferred. The protocol did not include diagnostic assessment. Instead, confirmations of mental health diagnoses were sought in writing from general medical practitioners and from public and private psychiatrists. Treatment professionals were asked to verify stated DSM-IV [1] diagnoses. Outstanding requests were followed up monthly until all confirmations were obtained.
Each participant provided information about health status, demography, family, social and vocational activities, and assistance received. Social support was assessed using four items from the brief version of the Social Support Questionnaire [40], [41]. Health outcomes were assessed using two scales with known reliability and validity, the Health of the Nation Outcomes Scale [42] and the Clinical Global Impressions (CGI) severity item [43–45]. No interventions were implemented by the research team. Official information about Federal income support and public funded vocational assistance was supplied to all participants.
Statistical analyses
Subjective experiences not experienced in the past 6 months were considered equivalent to experiences rated as having no impact on the ability to work normally. Construct validity was examined at baseline via coefficient alpha and by principal factor analyses. Testretest reliability was assessed during the pilot study supplemented by a small baseline sub-sample. Criterion validity was assessed by examining baseline correlation patterns with respect to known correlates of employment variables. All analyses were conducted using SAS [46].
Results
Respondents
Baseline interviews were completed by 111 people recruited between May and August 2001. Of the 104 people meeting inclusion criteria, 94 (90.4%) completed second interviews and 94 (90.4%) completed third interviews. Reasons for non-participation at the second interview included: lost contact (n = 7), withdrawn (n = 1), deceased (n = 1), and incarcerated (n = 1). Two non-participants at the second interview completed the third interview. Ninety-two people (88.5%) completed all three interviews. Telephone interviews were needed for two people who had moved out of the catchment area. There were no partial refusals, and missing data (< 1%) eventuated when a particular variable could not be assessed. Participant demographic characteristics are shown in Table 1. The mean age of male participants at baseline was 36 years and 8 months (n = 77, SD = 9 years and 10 months, range 19–56 years). Female participants were of similar age (mean = 36 years and 3 months, n = 27, SD = 8 years and 8 months, range 23–52 years).
Demographic characteristics by role category for urban residents with schizophrenia or schizoaffective disorder at baseline (n = 104)
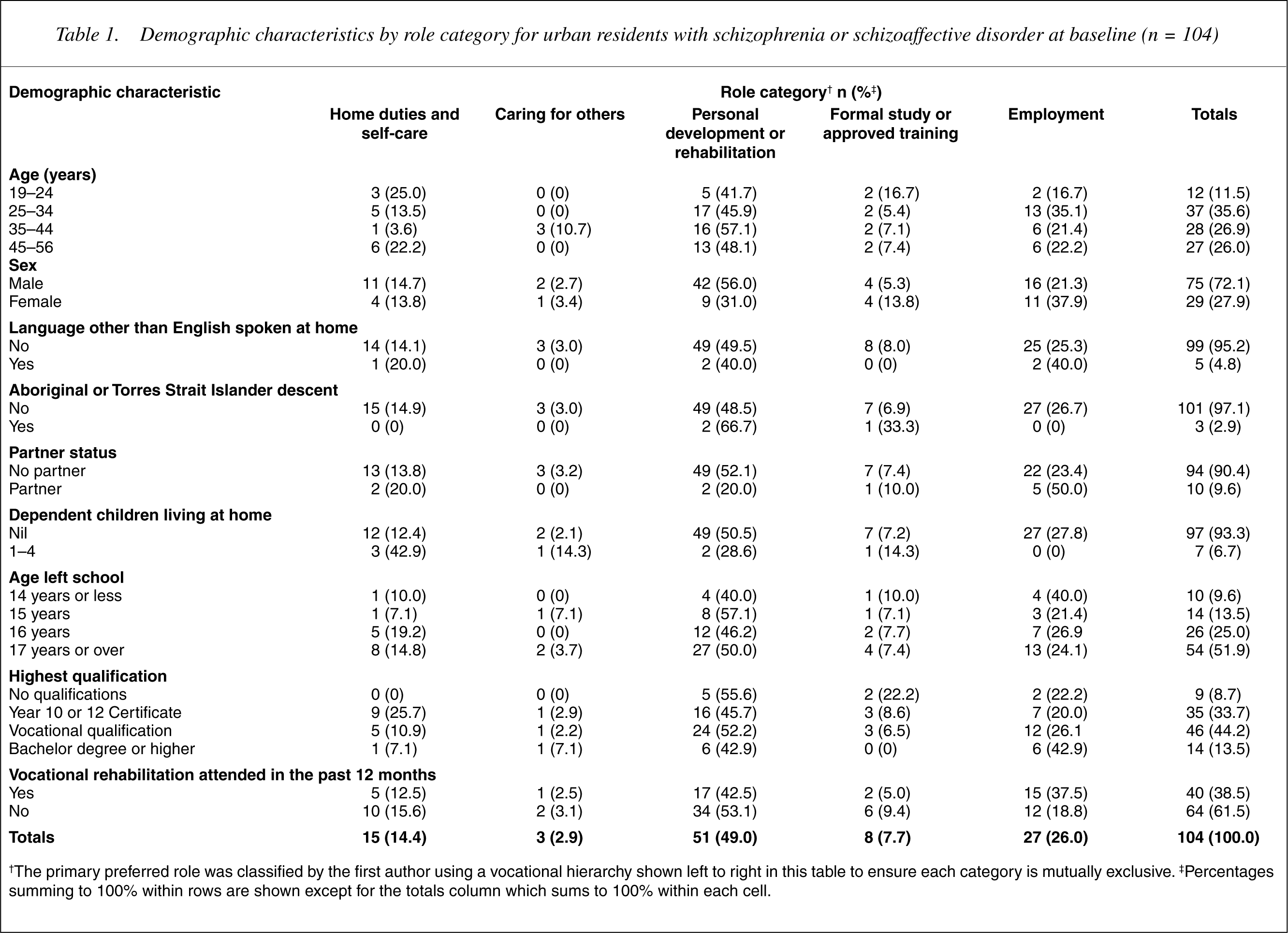
†The primary preferred role was classified by the first author using a vocational hierarchy shown left to right in this table to ensure each category is mutually exclusive. ‡Percentages summing to 100% within rows are shown except for the totals column which sums to 100% within each cell.
Diagnostic validity
DSM-IV [1] diagnoses were confirmed for all participants by July 2002. Of those meeting inclusion criteria, 96 had a confirmed diagnosis of schizophrenia and eight had a confirmed diagnosis of schizoaffective disorder. The validity of treating professionals' diagnoses was checked by accessing with ethics approval, the research diagnoses for a subsample (n = 17) who had also participated in separate studies involving the Diagnostic Interview for Psychosis [47] which incorporates items from the WHO Schedules for Clinical Assessment in Neuropsychiatry [48] and the diagnostic algorithm from the Operational Criteria for Psychosis [49]. In all cases, treating professionals' diagnoses were confirmed with no diagnostic discrepancies (100% agreement).
Construct validity
The 38-item set of work-related subjective experiences was compared to 20 established scales to identify content overlap and content divergence (see 50] where 16 items had similar content such that 42.1% of the new scale overlapped with 17.8% of the SCL-90. At the other extreme, three of four items from the Role Functioning Scale (RFS, 65) had a degree of content similarity, indicating 7.9% of the new scale overlapped with 75% of the RFS. The new scale encompassed 50–100% of four smaller established scales (rows 4,5,7 and 18 of Table 2).
Content overlap† and divergence of the Work Related Subjective Experience (WRSE-38) with respect to a sample of 20 established scales
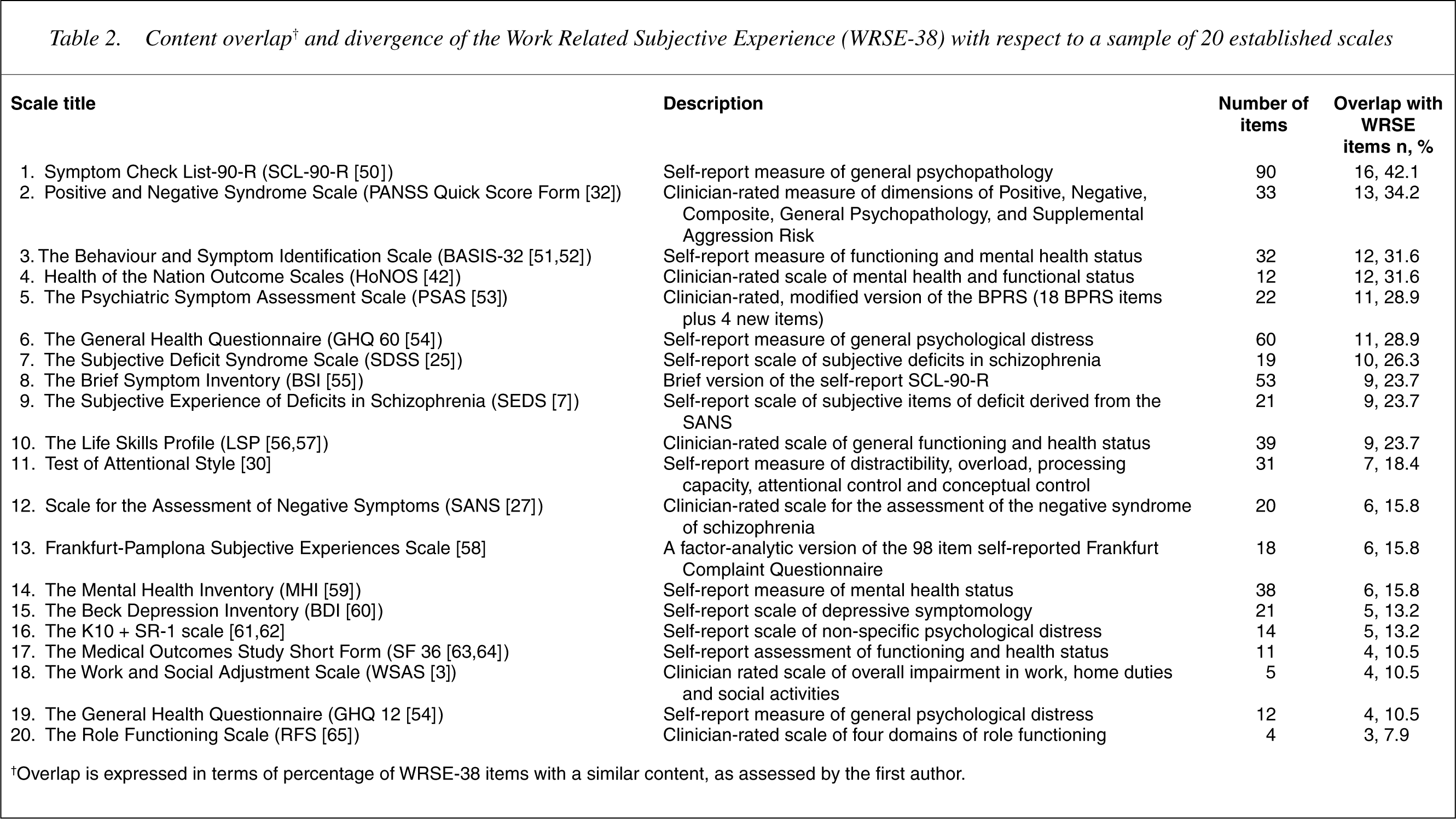
†Overlap is expressed in terms of percentage of WRSE-38 items with a similar content, as assessed by the first author.
This comparison indicated that work-related subjective experiences represent a broader domain than experiences addressed by any one established measure examined. The focal difference is that unlike established measures, the new measure only includes subjective experiences perceived to impact on employment. The broader content domain and partial content divergence from established scales supported the validity of the new construct. However, this evidence does not exclude the possibility that an established scale may adequately serve this purpose (e.g. the SCL-90) when modified to elicit perceptions of impact on employment functioning.
Internal consistency
Internal consistency was examined by Cronbach's coefficient alpha analysis at baseline. This revealed four items which did not contribute to internal consistency of the measure considered as a single dimension. When deleted, each marginally increased the value of coefficient alpha for the remaining items. Other items when removed, marginally decreased the alpha coefficient, indicating good internal consistency for 38 items (alpha = 0.927). The ratio of sample size (n = 92) to the number of repeat measure items (3 × 38) precluded the use of confirmatory factor analysis as a reliability test at subsequent interviews. However, the reliability of the single dimension (38 items) was supported by strong alpha values at 6 and 12 months (0.927–0.939 and 0.926–0.939 for 42 items) despite elapsed time, sample size reduction (104–94) and item reduction (42–38).
Factor structure
Principal factor analysis revealed an unrotated first factor accounting for 10.5% of the variance. The four non-contributing items in the previous analysis did not load in the single factor solution (loadings 0.06–0.26). Loadings by the remaining 38 items ranged from 0.28–0.69. Of these, eight were considered marginal (0.28–0.40). The single factor solution indicated removal of otherwise promising items (these were retained) with high face validity in vocational settings (e.g. ‘Too many cigarettes’, 0.28; ‘Trouble recognizing people’, 0.29; ‘Hard to get started in the morning’, 0.33; ‘Difficulty learning new things’, 0.35). Multi-factor structures were also explored. The eigenvalue criterion (< 1.0) indicated that up to five factors were likely. Orthogonal and oblique rotations of 2–5 factor solutions were examined for interpretable and simple structures (loadings < 0.40 on one factor only). Of these, a five factor orthogonal solution appeared the most interpretable, accounting for 16.2% of the variance.
Factor loadings for the preferred solution are shown in Table 3. The five factors and their alpha coefficients were: ‘Psychological distress’, 0.84; ‘Memory and decision making’, 0.83; ‘Thinking and communicating’, 0.77; ‘Symptom control’, 0.76; and ‘Energy management’, 0.65. Although a clear pattern emerged, some loadings were unexpected. ‘Difficulty learning new things’ loaded on ‘Energy management’ and appeared to represent the mental energy required for workplace learning. ‘Worried about money’ loaded on ‘Thinking and communicating’ rather than on ‘Psychological distress’, suggesting that being ‘Worried about money’ impacts on people indirectly via general ‘Thinking and communicating’ than through causing direct psychological distress. Similarly, ‘Hard to get started in the morning’ loaded on ‘Psychological distress’ rather than on ‘Energy management’, perhaps emphasizing the challenging daily burden of psychological distress over an on-going problem of energy management. The marginal loading of the item ‘Too many cigarettes’ was also informative suggesting that tobacco craving among heavy smokers can impact on workplace ‘Thinking and communicating’.
Baseline factor structure† of subjective experiences perceived to impact on employment by community residents with schizophrenia or schizoaffective disorder (n = 104)
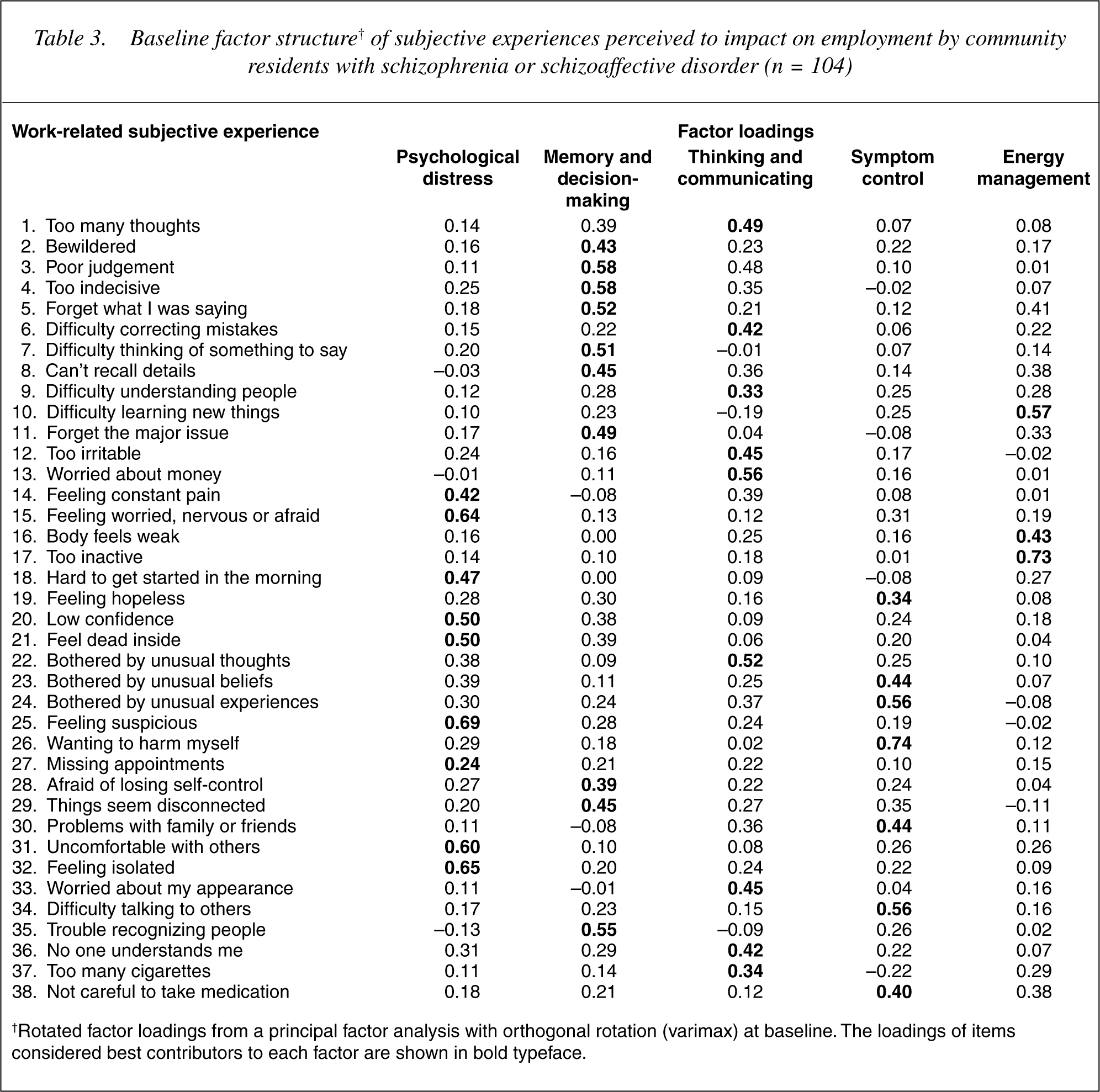
†Rotated factor loadings from a principal factor analysis with orthogonal rotation (varimax) at baseline. The loadings of items considered best contributors to each factor are shown in bold typeface.
Items grouped by original source dimensions at baseline were examined for internal consistency. This was satisfactory for source dimensions consisting of five or more items, numbered as in Table 3 (‘Delusional’, items 22–26, 0.80; ‘Social’, 30–34, 36, 0.79; ‘Attention & memory’, 1–2, 5, 7–9, 11, 0.77; ‘Cognitive’, 3–4, 6, 10, 28–29, 35, 0.74; ‘Affective’, items 12–15, 19–21, 0.73). Internal consistency declined for the smaller ‘Negative’ dimension (items 16–18, 27, 0.53) and for the ‘Drug and medication’ dimension (37–38, 0.28). Item source dimensions had similar satisfactory internal consistency when sufficient items were present, indicating that these remain plausible alternatives to the observed factors. Independently of a promising factor structure, the high internal consistency (0.93) of the 38-item set supported a uni-dimensional application of the new measure.
Test-retest stability and reliability
The 28–35 day test-retest stability (see Table 4) refers to the proportion of people who consistently reported the presence or absence of a particular subjective experience. Reliability was indicated by correlations between repeated ratings of perceived impact on employment functioning. In the pilot study (n = 21) long-cycle test-retest reliability was calculated from the VAS. At baseline, although clearly underpowered (n = 5), the correlation pattern at 1–8 days (compare columns 3 and 5 in Table 4) suggested promising test-retest reliability, particularly for more specific items. Encouragingly, no single item had consistently low stability and test-retest reliability. However, the low power of the baseline sample and the limited convergence among measures of stability and reliability indicate further investigation of this attribute is essential.
Test-retest stability and reliability of subjective experiences perceived to impact on employment by community residents with schizophrenia or schizoaffective disorder
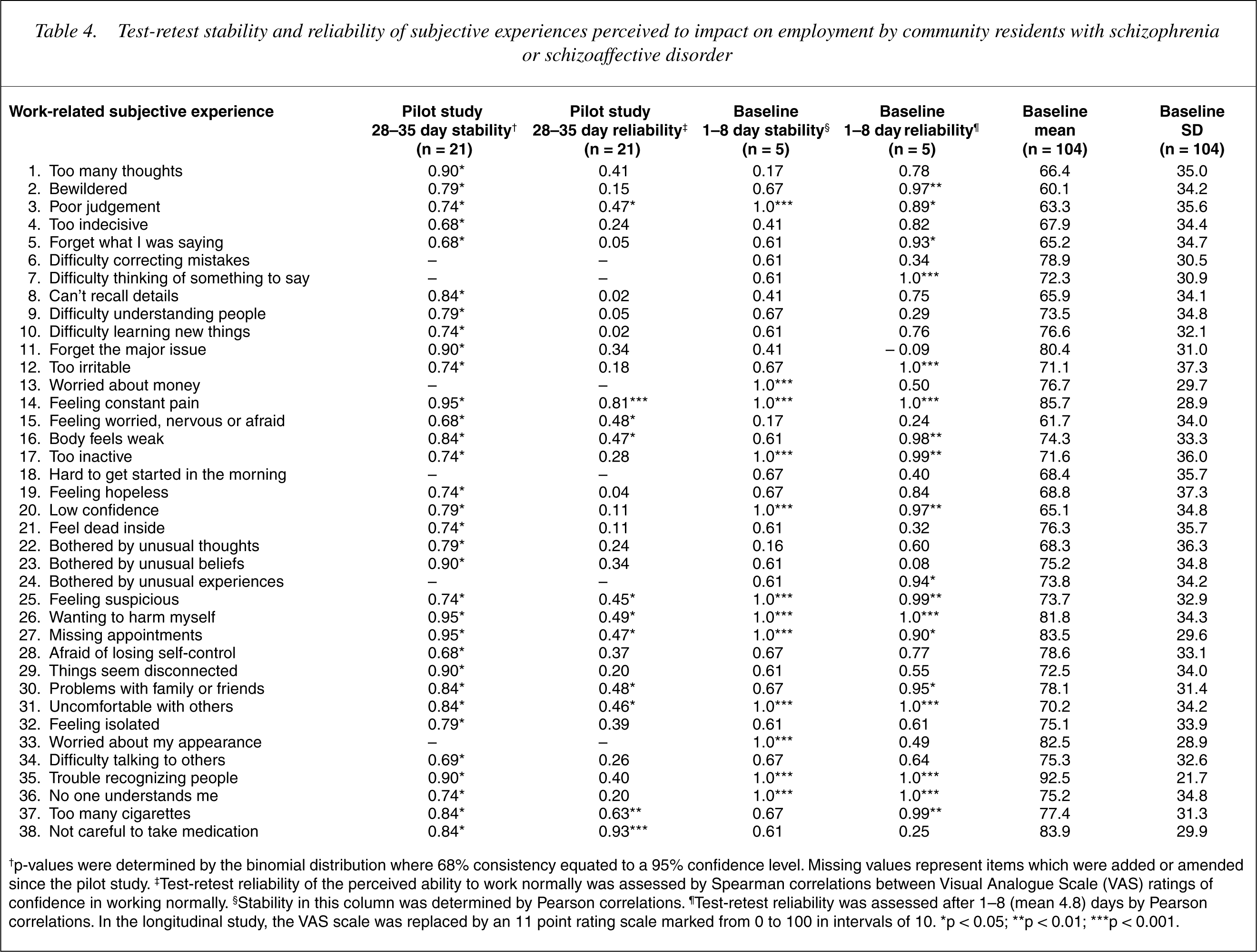
†p-values were determined by the binomial distribution where 68% consistency equated to a 95% confidence level. Missing values represent items which were added or amended since the pilot study. ∥Test-retest reliability of the perceived ability to work normally was assessed by Spearman correlations between Visual Analogue Scale (VAS) ratings of confidence in working normally. §Stability in this column was determined by Pearson correlations. ∥Test-retest reliability was assessed after 1–8 (mean 4.8) days by Pearson correlations. In the longitudinal study, the VAS scale was replaced by an 11 point rating scale marked from 0 to 100 in intervals of 10. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Responsiveness
Individual trajectories of mean work-related subjective experiences over 12 months were graphically examined. Without interventions, it was expected that work-related subjective experiences would endure. Mean scores were examined for time effects by repeated measures analysis of variance. The omnibus result (p = 0.14; df = 2, 282; F = 2.0) and both individual contrasts (p1 = 0.66, p2 = 0.30) indicated stable means, not statistically different at baseline (mean = 74.29, SD = 17.80), 6 months (M = 77.13, SD = 17.46) and 12 months (mean = 77.27, SD = 16.20).
Although means were stable, there was marked individual variation in terms of grand mean deviations and time-related fluctuations. The possible causes include: measurement error; the transient nature of subjective experiences; or stable subjective experiences with varied perceived impact on employment, possibly related to the experience specificity. Responsiveness to individual differences was indicated because each individual (n = 92) had a unique 12 month trajectory of work-related subjective experiences.
Criterion validity
This was assessed by examining convergence with disorder severity where the severity measure also correlated with employment variables. Work-related subjective experiences were associated with total Health of the Nation Outcome Scale (HoNOS) score (r = −0.54, p < 0.001); CGI severity score (r = −0.50; p < 0.001); and Course of illness (r = −0.40; p < 0.001). Total HoNOS and CGI severity scores were also correlated (r = 0.71; p < 0.001). Work-related subjective experiences achieved similar correlations to the HoNOS total score and CGI severity score with respect to current employment. Work-related subjective experiences performed better than HoNOS item 12. Differences emerged with respect to other employment related variables (see Table 5). The new measure was not associated with having a current vocational goal, weeks worked in the previous year, or years since last employed, and unlike the HoNOS and CGI, was weakly associated with previous years of continuous employment.
Criterion validity of Work-related subjective experiences (WRSE-38) among community residents with schizophrenia or schizoaffective disorder at baseline (n = 104)
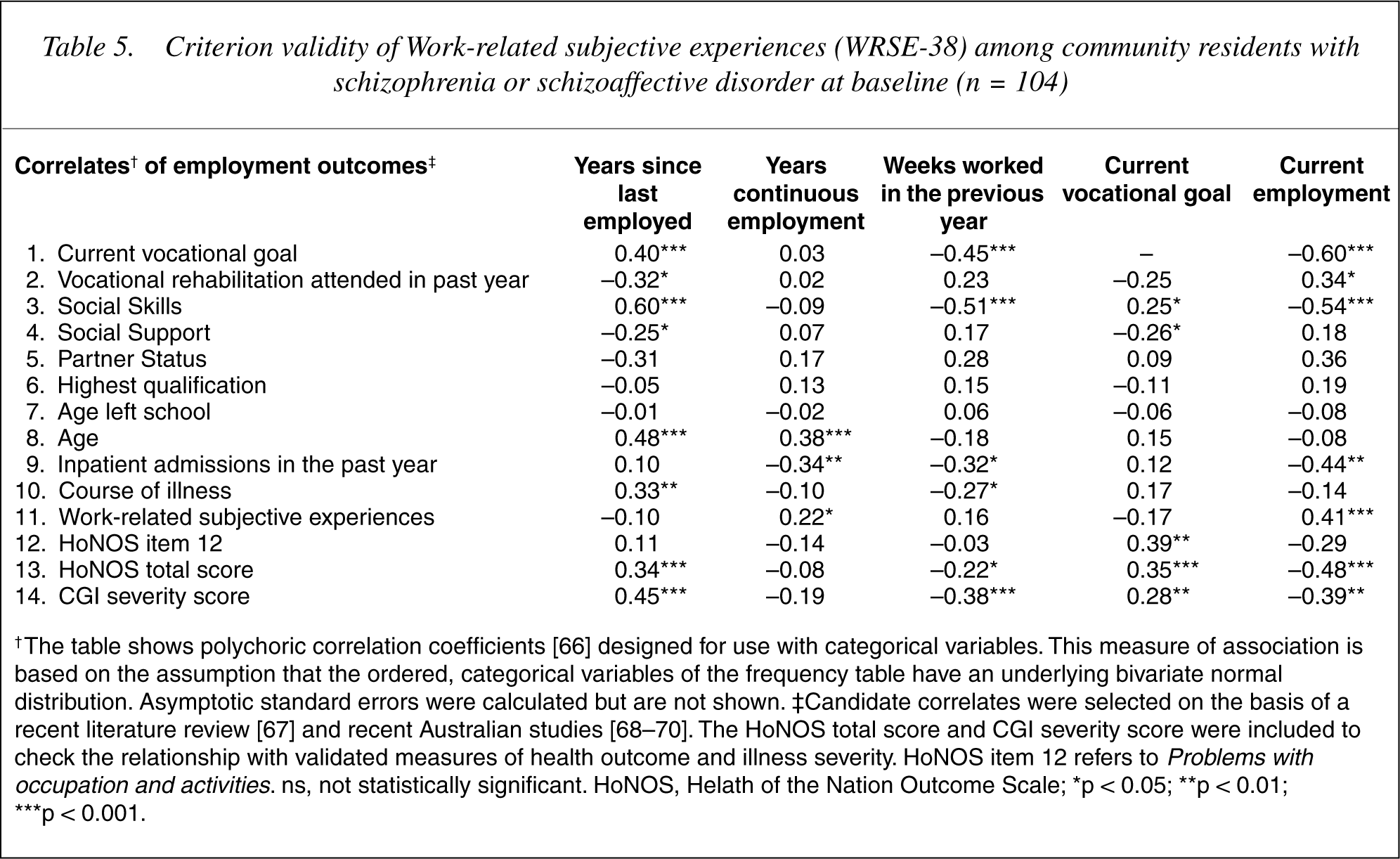
† The table shows polychoric correlation coefficients [66] designed for use with categorical variables. This measure of association is based on the assumption that the ordered, categorical variables of the frequency table have an underlying bivariate normal distribution. Asymptotic standard errors were calculated but are not shown. ‡Candidate correlates were selected on the basis of a recent literature review [67] and recent Australian studies [68–70]. The HoNOS total score and CGI severity score were included to check the relationship with validated measures of health outcome and illness severity. HoNOS item 12 refers to Problems with occupation and activities. ns, not statistically significant. HoNOS, Helath of the Nation Outcome Scale; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Alternative explanations
Possible confounding by extraneous variables was examined at baseline. Work-related subjective experiences were not related to: interviewer ratings of credibility of the information provided; ability to take medication regularly; current or previous problems with alcohol or drugs; the order of two major question subsets (work related subjective experiences, and work related self-efficacy); the length of interview; or the identity of the interviewer.
Discussion
The results indicate that work-related subjective experiences are a promising source of new information that may in time contribute to explaining individual career learning experiences according to the social cognitive career theory [15]. These data suggest that the new measure is similar to the HoNOS total score and the CGI severity score in terms of strength of association with employment outcomes. The new scale seems a stronger correlate of current employment than HoNOS item 12, and interestingly, stood out through no association with the presence of a vocational goal. Although the new measure cannot be considered superior to either the HoNOS or the CGI as a predictor of employment outcomes, it is potentially more useful in vocational contexts through being able to identify specific subjective experiences perceived to contribute to employment restrictions.
Consequently, the new measure may have applications throughout supported employment or vocational rehabilitation with respect to assessing assistance needs for specific tasks. Each item, when endorsed, may facilitate communication about how the specific experience impacts on the perceived capacity to perform the required activity, and how these perceptions lead to activity restrictions and subsequent needs for assistance. Adverse work-related subjective experiences, if not ameliorated, could impair performance and lead to negative career learning experiences [15] and degraded self-efficacy [19–22] for critical activities.
The evidence reported here indicates that the new scale has face validity grounded in consumer reports, construct validity, high internal consistency, a plausible factor structure, elements of test-retest stability and reliability, individual responsiveness, criterion validity, and conceptual links to career development and to selfefficacy, an established predictor of work performance. Consequently, the new measure may have promising research and vocational applications, including potential use as an intermediate variable in investigations of the effectiveness of vocational rehabilitation and supported employment programs.
Limitations
This study was limited by resources which precluded probability sampling and restricted both sample size and the maximum length of interviews. These limitations were partly addressed by: restricting the diagnostic range; diagnostic validation by standardized research protocols; use of repeated measures; and by incorporating brief health outcome measures in the design. Although psychometric indicators were favourable, short cycle test-retest reliability, discriminant and predictive validity, and the validity of single items in vocational counselling are yet to be investigated. In addition, the preliminary psychometric properties are based on people with schizophrenia or schizoaffective disorder, hence further investigations exploring the utility of the measure in other psychiatric disorder populations are required.
Although the new measure appears promising, it is premature to conclude that it is superior to existing measures of illness severity and disability at predicting employment assistance needs. There is also insufficient evidence that the subjective experiences chosen are an optimal set of experiences for understanding career learning experiences and for exploring the nature and origin of employment restrictions. The more transient or unstable experiences and those with more extreme responsiveness which were eliminated, could be more useful than the retained items. It is also plausible that other psychopathology scales such as the SCL-90 when modified to assess confidence for working normally, may be similarly effective.
Conclusions
Subject to satisfactory results from on-going psychometric investigations, work-related subjective experiences promise to inform supported employment and vocational rehabilitation. The scale provides the structure for an individual exploration of a sample of subjective experiences perceived by others as relevant to employment functioning. Furthermore, the scale provides the framework for a discussion of how specific subjective experiences contribute to employment restrictions and the corresponding implications for specialized treatment, vocational interventions, or workplace accommodations.
Although the new measure is expected to contribute useful information, there is no evidence yet that an exploration of work-related subjective experiences leads to better vocational outcomes, or that individuals with more intensive assistance needs can be accurately identified. Nevertheless, the correlation with current employment is encouraging, as is the theoretical relevance to work performance and convergent validity with respect to standard measures of illness severity and disability.
The latter indicates links to clinician rated disability status with some evidence of independence from the diagnostic and global functioning perspectives. However, more evidence is needed before the scale can be described as a valid contributor to the early assessment of assistance needs in supported employment or vocational rehabilitation. The scale and user instructions are available from the corresponding author on request.
Footnotes
Acknowledgements
This investigation was conducted with ethics approval from the University of Queensland, West Moreton Health District, and Princess Alexandra and Royal Brisbane Hospitals' Human Research Ethics Committees. Financial support was provided by CRS Australia, The Schizophrenia Fellowship of South Queensland and the Queensland Centre for Mental Health Research (QCMHR). We thank: John McGrath of QCMHR and Nicholas Buys of Griffith University for comments on the original research proposal; Teresa Fawcett and Siobhan Coulter for data collection; and Stepping Stone Clubhouse and Tweed River Valley Fellowship for inkind support. We also sincerely thank all research participants without whom this study would not have been possible.