
Abstract
Stimulants have been used in medicine since 1935 for treatment of a variety of conditions including attention deficit hyperactivity disorder (ADHD), narcolepsy, obesity and depression [1]. Currently in Australia, short acting preparations of methylphenidate and dexamphetamine have Therapeutic Goods Administration (TGA) indications for ADHD and narcolepsy. Long-acting preparations of methylphenidate are only indicated for ADHD [2]. Given the low prevalence of narcolepsy, estimated to be 25–50 per 100,000 [3], the majority of stimulant prescribing in Australia is thought to be for attention deficit hyperactivity disorder.
In 1998, the Australian child and youth national survey of mental health and well-being estimated the 12-month prevalence of ADHD in children aged 6 to 17 years was 11.2% with a higher prevalence in men (15.4%) than women (6.8%) [4]. In some individuals there is a continuation of symptoms into adulthood [5] with the full disorder persisting in 15% of subjects at age 25 years. Between 40% and 60% of adult subjects met criteria for partial remission of ADHD [6].
Psychosocial interventions are the first line treatments for ADHD. Pharmacotherapy should be reserved for those individuals with more severe symptoms or impairment, or for those individuals with moderate impairment who have not responded to psychosocial interventions. Stimulants (methylphenidate and dexamphetamine) have been shown to be a cost effective intervention for ADHD [7] and are recommended as the first line pharmacotherapy for ADHD [8].
International trends in prescribing of stimulants have been reported. Studies conducted in Canada, France, Netherlands, California, Israel and Australia have all shown increases in stimulant prescribing in recent years. Differences in the duration of the study period, the baseline rates of stimulant prescribing and age of patients receiving stimulant medication (children only compared to children and youth) prevents direct comparison of the studies [9–14].
Studies have reported trends of stimulant use in Australian states with an increase in the use of stimulants in children in Western Australia and New South Wales between 1984 and 2004 [15,16] and in adults in New South Wales between 1990 and 2002 [17]. There were regional variations in Western Australia with stimulant prescribing rates in urban areas 2.3 to 5.3 times greater than remote areas [18]. In South Australia there has been no consistent trend of change in stimulant prescribing with rates of prescriptions varying between 1990 and 2006 [19].
We examined the national rates of dispensed prescriptions of stimulant medication for children, youth and adults in the Australian population between 2002 and 2009 and report the trends in dispensed stimulant prescriptions over this time by gender and age.
Methods
Data and data analysis
The data on the number of prescriptions dispensed for stimulants were obtained from the Drug Utilisation Sub-Committee (DUSC) of the Australian Department of Health and Ageing, The data were drawn from two sources. The first was the Medicare Australia records of prescriptions submitted for payment of a subsidy under the Pharmaceutical Benefits and Repatriation Pharmaceutical Benefits Schemes (PBS/RPBS). The second was an ongoing survey of a representative sample of community pharmacies from the Pharmacy Guild of Australia, which provides an estimate of the non-subsidized (private and under general co-payment) use of prescription medicines in the Australian community [20]. The majority of prescriptions (92%) dispensed in the Australian community (including residential care) were subsidized through the PBS. Although stimulants were publicly subsidized for those who met the Authority restrictions, it was also possible to obtain a private prescription at a higher cost to the patient.
Anonymized data on subsidized scripts included details of the drug product dispensed and information on the patient's gender and age. The use of prescription medicines dispensed to inpatients in public hospitals was not available for this report. In Australia, discharged patients from hospital are typically provided with only a short supply of medications, typically a maximum of one month's supply. Further prescriptions are provided by medical practitioners in the community. Data was also available on the average number of stimulants written by three different classes of prescribers: general practitioners (GPs); psychiatrists; and ‘other specialists’, which included paediatricians. Data differentiating other specialties and sub-specialisms were unavailable.
The quantity of each drug dispensed was standardized using the defined daily dose (DDD) per 1000 population per day (DDD/1000 population/day). The DDD, established by the WHO Collaborating Centre for Drug Statistics Methodology, corresponds to an estimated average daily dose used for a medication's principal indication [21]. Utilization was calculated for drugs with an anatomical therapeutic chemical code starting with N06BA, indicating psychostimulants. The drugs (with the defined daily dose in brackets) included: dexamphetamine (15 mg), methylphenidate (30 mg) and modafinil (300 mg). Age-standardized drug utilization rates for women and men were calculated for the period June 2002 to June 2009 (with appropriate half-year adjustment) using census mid-year population data [22]. For example, the utilization of 10 DDD/1000/day of dexamphetamine would correspond to about 1% of the population taking a standard 15 mg of dexamphetamine each day. Information on the gender and age of persons receiving a prescription were not available before 2002 as date of birth was not verified in prescription data prior to this.
All calculations were completed using Microsoft Office Excel 2003. The dataset incorporates all prescriptions in the time period studied. The large number of prescriptions would render all differences as statistically significant, regardless of clinical relevance [23].
Results
Overall use of individual stimulants
Total dispensing of stimulants increased 87% from 2.93 to 5.47 DDD/1000 population/day between 2002 and 2009 (Figure 1), representing an average increase of 11% per year. Although dexamphetamine prescriptions fell 13% from 2.02 to 1.75 DDD/1000 population/day and was dispensed almost exclusively through the PBS, total methylphenidate dispensing between 2002 and 2009 increased by 300%, from 0.45 to 1.81 DDD/1000 population/day in 2009. Most of the increase in methylphenidate can be attributed to the increase in dispensing of long-acting preparations. Methylphenidate 10 mg use increased after it became subsidized on the PBS in August 2005. There was immediate uptake of the extended release formulation of methylphenidate after it was introduced in April 2007, in addition to the existing use of the short-acting forms.
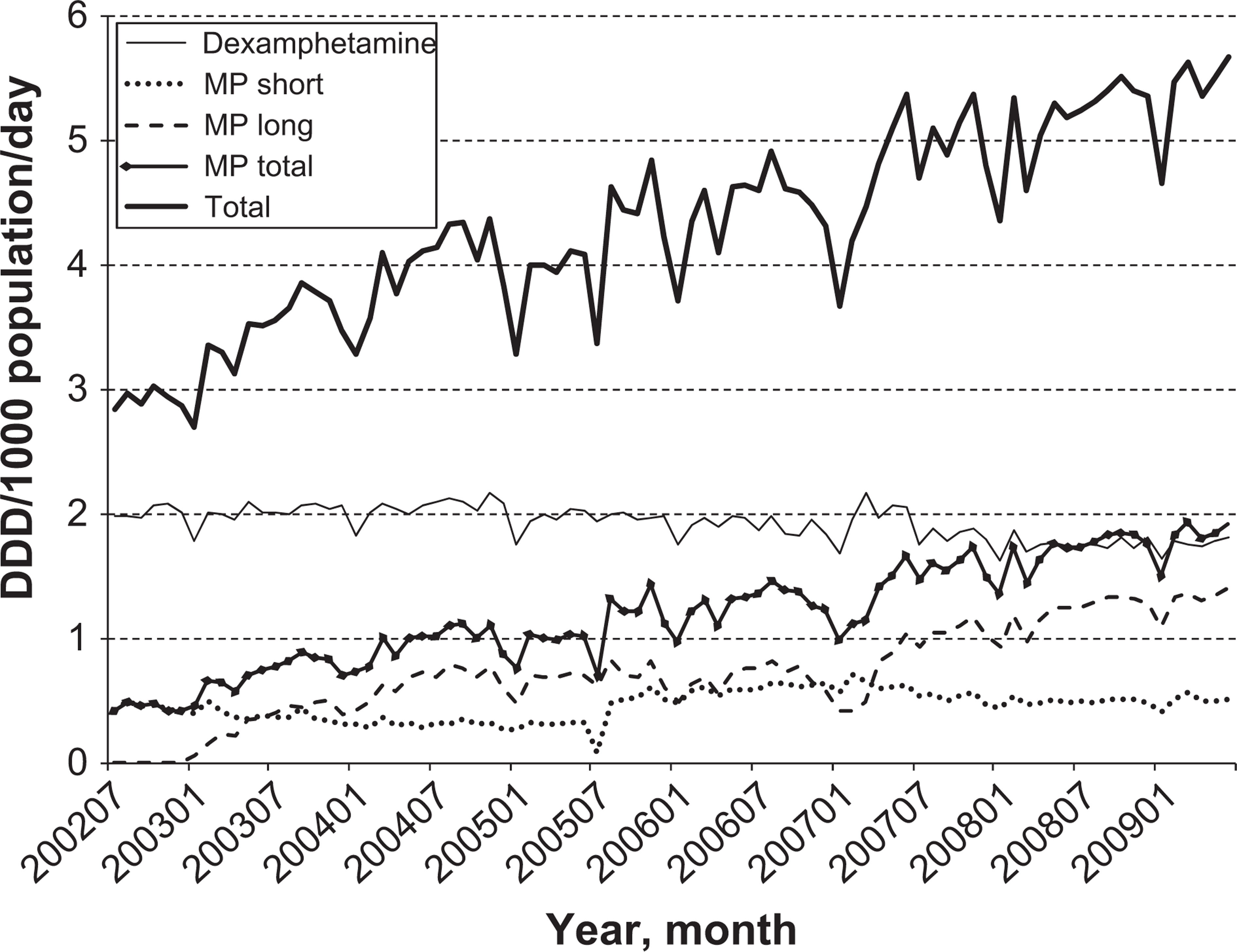
Drug utilization (DDD/1000 population/day) of dexamphetamine, methylphenidate (MP; short-acting, long acting and total) and combined total for each month between July 2002 and June 2009.
Stimulant use by class of prescriber
Figure 2 shows stimulant dispensing by category of prescriber averaged over twelve month periods in 2003, 2006 and a 6-month period in 2009. Dispensed prescriptions written by general practitioners (GPs) for dexamphetamine remained stable over time (Figure 2). From January 2009 to June 2009, GP prescriptions for dexamphetamine were dispensed on average 1.7 times more than methylphenidate (0.25 versus 0.15 DDD/day) and prescriptions for dexamphetamine written by psychiatrists were dispensed 3.9 times more than methylphenidate in the same period (0.52 versus 0.13 DDD/day). Prescriptions for methylphenidate written by ‘other specialists’ (including paediatricians) were dispensed 4.5 times more than dexamphetamine (1.18 versus 0.26 DDD/day). There was a 61.7% decrease in the average number of dexamphetamine prescriptions dispensed between 2002–2004 (0.78 DDD/1000 population/day) and 2007–2009 (0.3 DDD/1000 population/day) for ‘other specialists’ compared to a 17.1% reduction in dexamphetamine prescriptions by psychiatrists (0.63 to 0.52 DDD/1000 population/day). There was an almost three-fold increase in dispensing of methylphenidate prescriptions written by ‘other specialists’ between 2006 and 2009 from 0.32 to 1.21 DDD/1000 population/day.
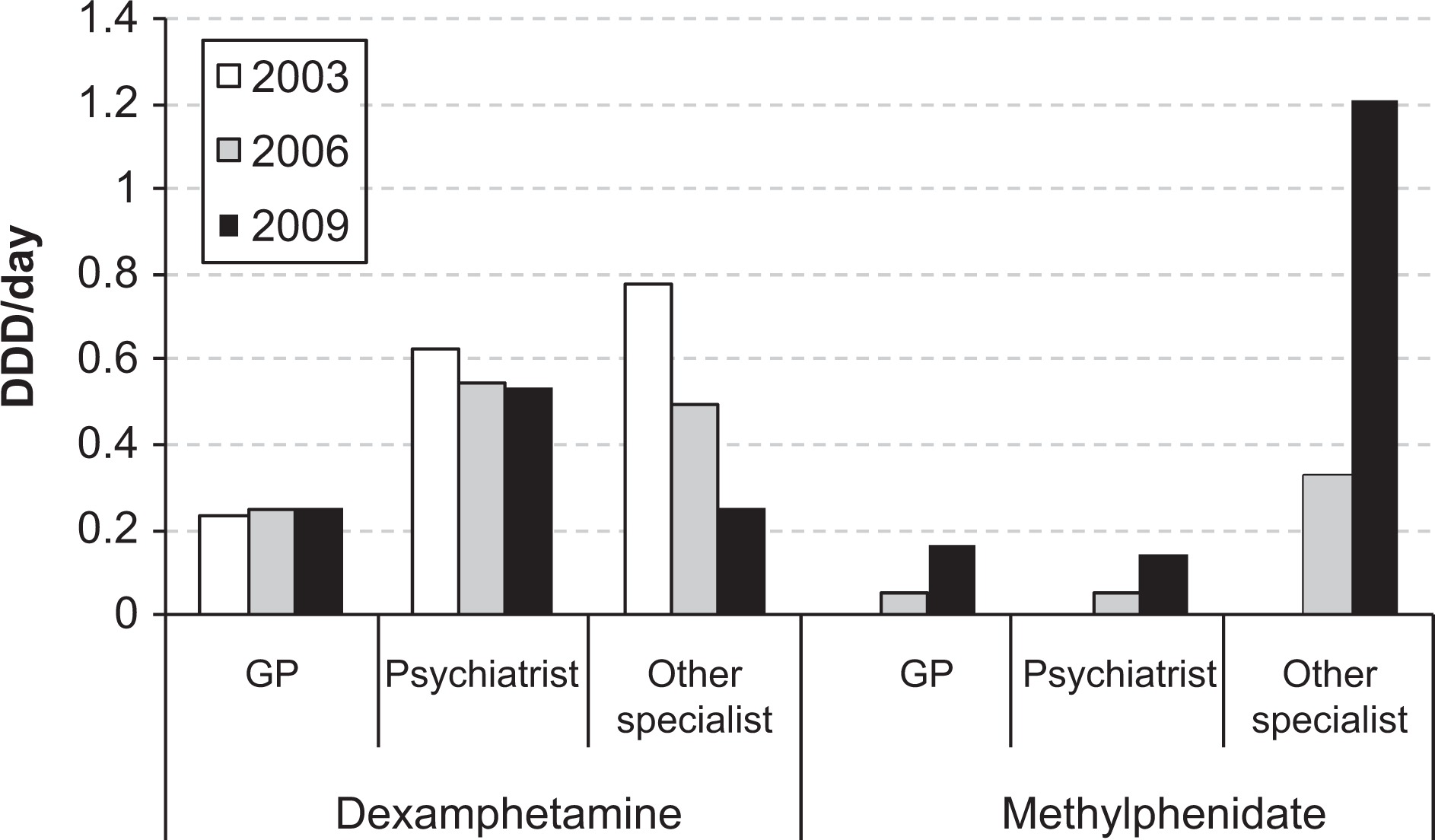
Drug utilization (DDD/day, averaged for each month within a year) for dexamphetamine and methylphenidate by prescriber category (GP, psychiatrist or other specialist, including paediatricians) for 2003, 2006 and 2009.
Stimulant use by gender and age
In 2007, age- and population-adjusted stimulant dispensing was higher in men than women (Figure 3) consistent with the higher prevalence of ADHD in men [2]. Until 2007 the data was received in 5-year age groups (which show more detail) but in 2008 and 2009 the data was provided only in 10-year age groups (data not shown). In 2007 (averaged over the first 6 months), dexamphetamine and methylphenidate were most commonly dispensed to patients aged 10–14 years: dexamphetamine dispensing was 1.3 DDD/1000 population/day in girls and 5.76 DDD/1000 population/day in boys, a 4.4-fold difference. The corresponding dispensing for methylphenidate was 2.07 DDD/1000 population/day in girls and 10.36 DDD/1000 population/day in boys, a 5-fold difference. The dispensing in boys aged 10–14 years corresponds to about 1.04% of boys aged 10–14 years receiving a standard dose of methylphenidate (30 mg) each day. Methylphenidate dispensing decreased for those aged 15 years or more and there was little dispensing of methylphenidate for those aged 25 years or over. There was, however, considerable dispensing of dexamphetamine to those aged over 25 years, with a gradual decline across the lifespan. The continued dispensing of dexamphetamine was observed in both women and men, with a greater magnitude in men. There was residual dispensing of dexamphetamine into older ages: 0.05 and 0.1 DDD/1000 population/day in women and men aged 80–84 years, respectively.
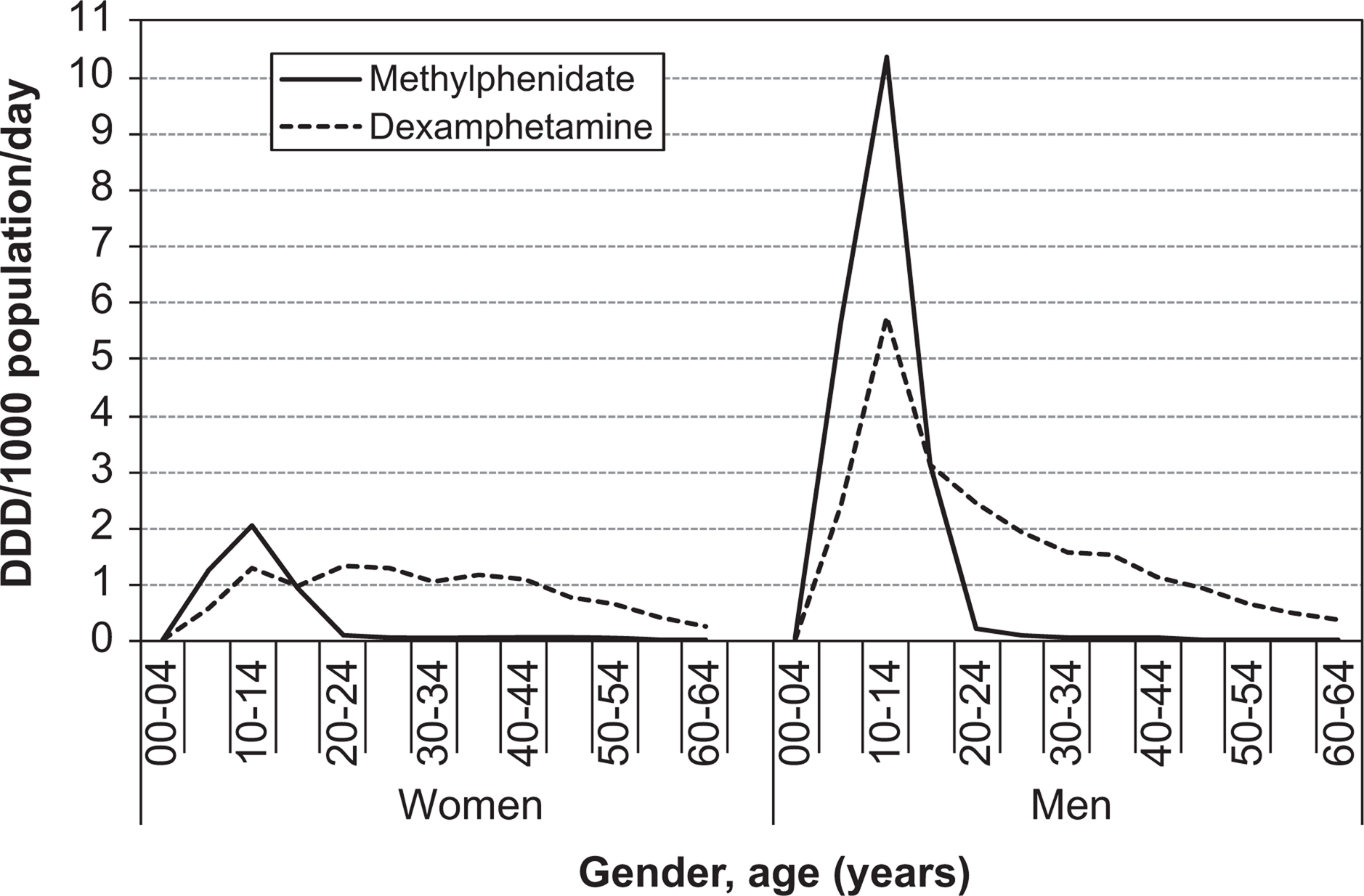
Subsidized dexamphetamine and methylphenidate utilization (DDD/1000 population/day) by gender (women on the left, men on the right) by five-year age groups (0–64 years) for 2007 (average of first 6 months).
Discussion
There was an 87% increase in stimulant dispensing in Australia between 2002 and 2009. Dexamphetamine remained the most commonly dispensed stimulant, with prescriptions falling 13% between 2002 and 2009. The increase in stimulant dispensing was attributable to a 300% increase of dispensed methylphenidate following PBS subsidization of the short-acting preparations from 2005 and longer acting preparations from 2007. Although the most likely explanation for the increase in methylphenidate dispensing was government subsidy, increased prescribing of stimulants for ADHD has also been reported in North America and Europe [9–13]. We conjecture that this may be due to a number of factors including studies showing the effectiveness of stimulants for ADHD treatment [24], increased public awareness of ADHD, societal changes (for example children living in smaller housing, greater expectations of students to remain at school) and the influence of marketing by pharmaceutical companies [25].
Dispensing of stimulant prescriptions for both men and women peaked at 10–14 years of age. We hypothesize that this coincides with increasing cognitive demands in the school environment and increasing expectations from parents, teachers and perhaps the students themselves.
The use of stimulants was approximately five times greater in men than women, although the Australian prevalence of ADHD is 2.45 times greater in men than women [4]. Thus the amount of stimulants dispensed to men compared to women is disproportionately greater compared to the relative sex differences in the prevalence of the disorder. This may be explained by a gender difference in symptom profiles with men more likely to have comorbid disruptive behavioural disorders compared to women [26]. Additionally, the doses prescribed to men may have been on average higher than those prescribed to women resulting in the increased drug utilization in men relative to women.
The rising trend of stimulant dispensing over the study period will inevitably draw public scrutiny. In 2007, approximately 1% of men and 0.5% of women aged 10 to 14 in Australia were dispensed stimulant medication. This is lower than the reported Australian or international prevalence of ADHD [4,27]. Medical practitioners need to provide patients and carers with both pharmacological and non-pharmacological options for the management of ADHD and collaboratively determine the most appropriate management for each individual. Future epidemiological surveys should examine whether the use of stimulants is restricted to a minority of patients with ADHD symptoms, as was evident in the national survey conducted in 1998 [28].
There are several limitations in this study. Beyond gender and age, we were unable to determine other characteristics of stimulant medication users. Further research is needed to explore which patients are receiving stimulants. Dispensed prescriptions may not reflect actual medication consumption. Stimulants are recognized as potential drugs of abuse and the risk of diversion of stimulants remains a potential problem [29].
We were unable to determine what proportion of stimulant dispensing was for narcolepsy [3] or the short-term treatment of depression [30], particularly for older persons [31]. The Drug Utilisation Sub-Committee (DUSC) and Pharmacy Guild data do not allow for gender or age stratification in private or under general co-payment prescription data. Thus there are limitations on data analysis of non-subsidized scripts. The use of prescription medicines dispensed to inpatients in public hospitals is not captured by this study but the missed contribution is likely to be small compared with overall prescribing rates.
The defined daily doses are standardized as the maintenance dose in adults. Hence, the lower DDD in younger children compared to the 10–14 year olds may reflect a lower dosage rather than a lower number of patients prescribed stimulants. Similarly, doses prescribed to adults may be higher than those prescribed to 10–14 year olds. Therefore, the data presented here, especially for young children, are likely to be conservative. No further information was available on the ‘other specialists’ category of prescribers. Although we believe this will consist predominantly of paediatricians, we have no way of verifying this. Previous research has shown interstate and intrastate variability in stimulant prescribing [14–19]. Unfortunately, data available from the Drug Utilisation Sub- Committee (DUSC) of the Australian Department of Health and Ageing did not allow interstate comparisons.
In spite of the above limitations, this is the most comprehensive report to date of Australian national trends of stimulant dispensing. A major strength of this study is that it represents the complete capture of all subsidized dispensing of stimulant medications by gender and age in the Australian community during the study period. This study may serve as a baseline against which to compare national use of stimulant medication. Given the availability of different formulations of methylphenidate, it will be of interest to examine how the availability of new agents such as atomoxetine [32] influences the prescribing behaviours of Australian medical practitioners for treatment of ADHD. It will also be of interest to examine whether this trend of increased stimulant dispensing continues.
Footnotes
Acknowledgements
We acknowledge the assistance of Hera Lutsenko in data analyses.