
Abstract
Processing of facial expressions of emotion is central to human interaction, and has important effects on behaviour and affective state. A range of methods and paradigms have been used to investigate various aspects of abnormal processing of facial expressions in major depression, including emotion specific deficits in recognition accuracy, response biases and attentional biases. The aim of this review is to examine and interpret data from studies of facial emotion processing in major depression, in the context of current knowledge about the neural correlates of facial expression processing of primary emotions. The review also discusses the methodologies used to examine facial expression processing. Studies of facial emotion processing and facial emotion recognition were identified up to December 2009 utilizing MEDLINE and Web of Science.
Although methodological variations complicate interpretation of findings, there is reasonably consistent evidence of a negative response bias towards sadness in individuals with major depression, so that positive (happy), neutral or ambiguous facial expressions tend to be evaluated as more sad or less happy compared with healthy control groups. There is also evidence of increased vigilance and selective attention towards sad expressions and away from happy expressions, but less evidence of reduced general or emotion-specific recognition accuracy. Data is complicated by the use of multiple paradigms and the heterogeneity of major depression. Future studies should address methodological problems, including variations in patient characteristics, testing paradigms and procedures, and statistical methods used to analyse findings.
The ability to identify and interpret facial expressions of emotion is crucial to functioning in social networks and to interpersonal relationships. This is because facial expressions can signal our emotional states and those of others, and also because they influence the production and regulation of affective states and behaviour in response to these signals [1]. Affective states may then influence sensitivity to and selective attention towards facial emotional expressions.
Although there is some debate regarding how many primary or discrete facial expressions of emotion there are, Ekman [2] has described six, which are often called the six ‘basic’ emotions. These include sadness, happiness, surprise, anger, disgust, and fear. Ekman's studies report that many populations (including isolated tribes) are able to recognize facial expressions of these emotions [3].
Abnormal facial emotion processing has been studied in a range of psychiatric conditions, including major depression. This is of interest, firstly because studies of facial emotion processing may provide important information regarding abnormalities of regional brain functioning in major depression. Secondly, abnormal facial emotion processing may directly give rise to some of the affective and social symptoms in major depression and other psychiatric disorders. Thirdly, changes in facial emotion processing may help in the prediction of or monitoring of response to treatment in major depression [4].
This review will examine findings from behavioural studies of facial emotion processing in major depression, including emotion specific deficits in recognition accuracy, emotion specific response biases and attentional biases, examine the literature on neural correlates of facial emotion processing in major depression, and examine the methodology of studies of emotional facial emotion processing in major depression.
To do this we conducted a general review on all available literature of facial emotion processing in major depression.
Method
Search strategy
Electronic database searches were carried out for relevant papers utilizing MEDLINE and Web of Science from 1980 up until December 2009. In the initial search, the terms ‘major depression’, ‘depression’, ‘major depressive disorder’, ‘mood disorders’ or ‘affective disorders’, and ‘facial emotion processing’ or ‘facial expression recognition’ were used. To ensure inclusion of all possible available articles including the most recent, ScienceDirect was also searched using these key words in the ‘abstract, title, key words’ field. We also checked the reference lists of all the relevant papers. The Web of Science was also used to review the articles that had cited the relevant articles found through the above search strategies.
Inclusion criteria
We selected only those articles examining facial emotion processing in adult samples with a diagnosis of major depression. All studies were limited to English language publications.
Results
A total of 40 studies met the inclusion criteria (see Table 1). The studies used a range of testing paradigms and methods. The clinical characteristics of the depressed groups varied substantially.
Studies of facial emotion processing in depressive disorders
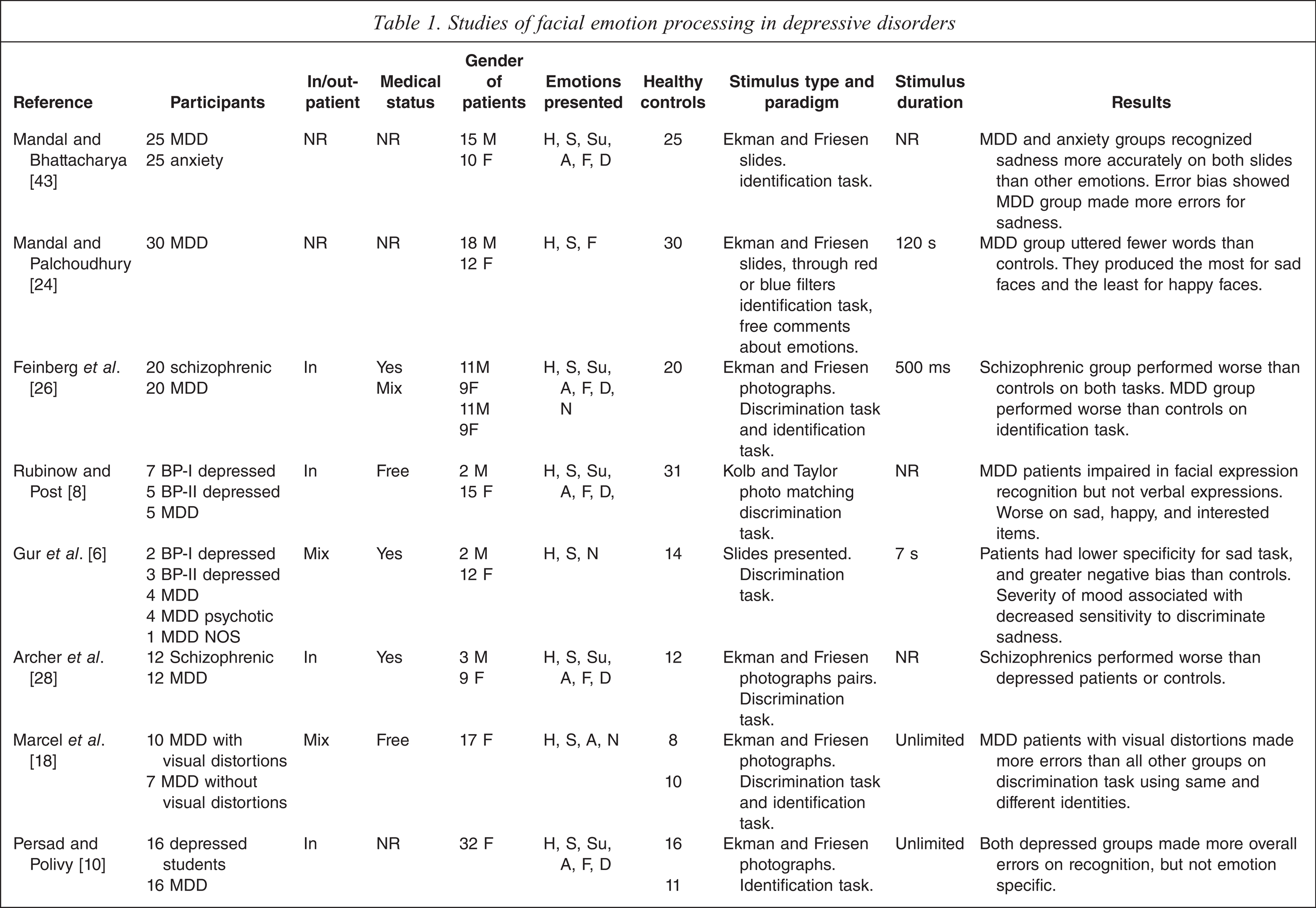
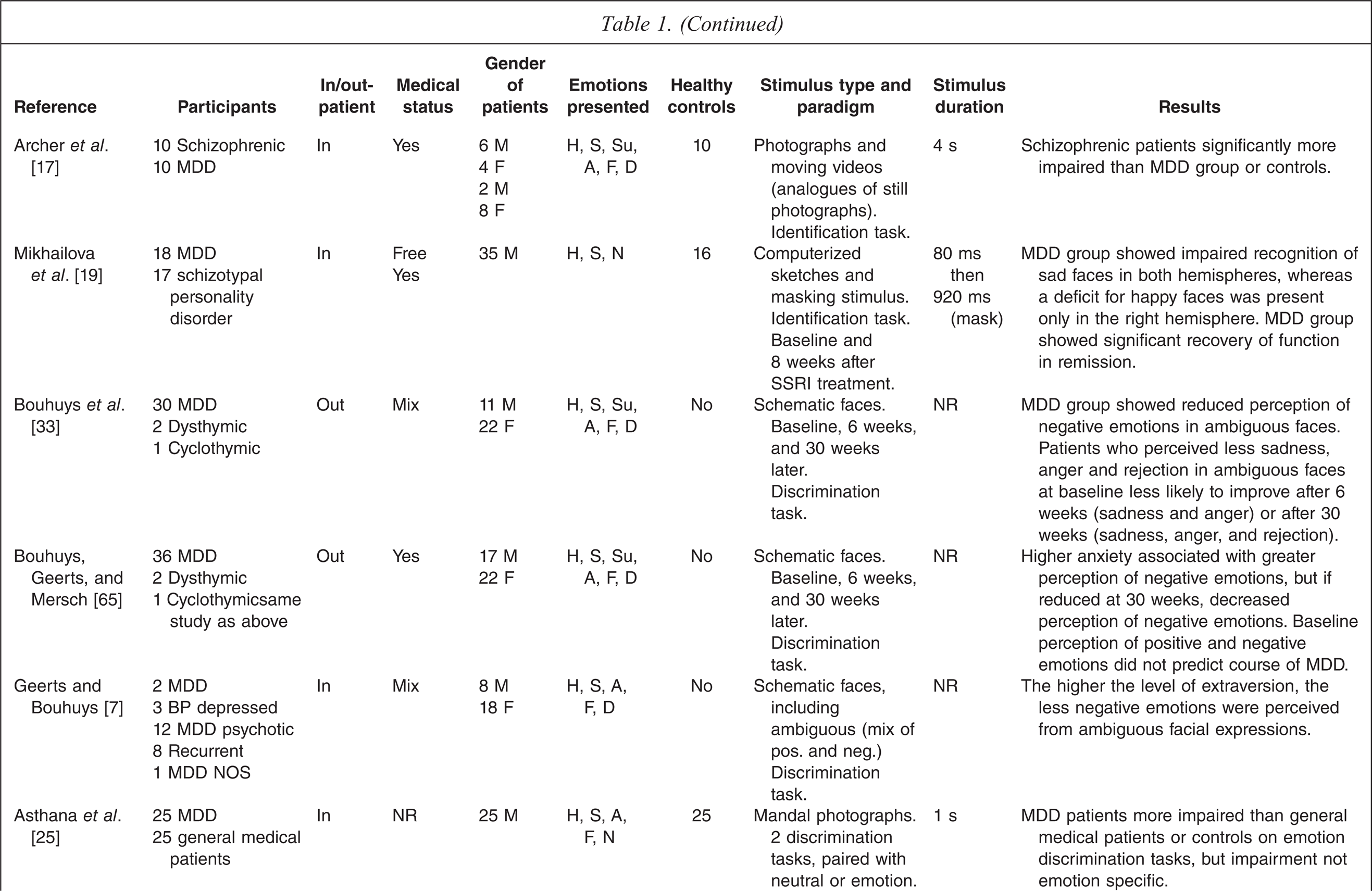
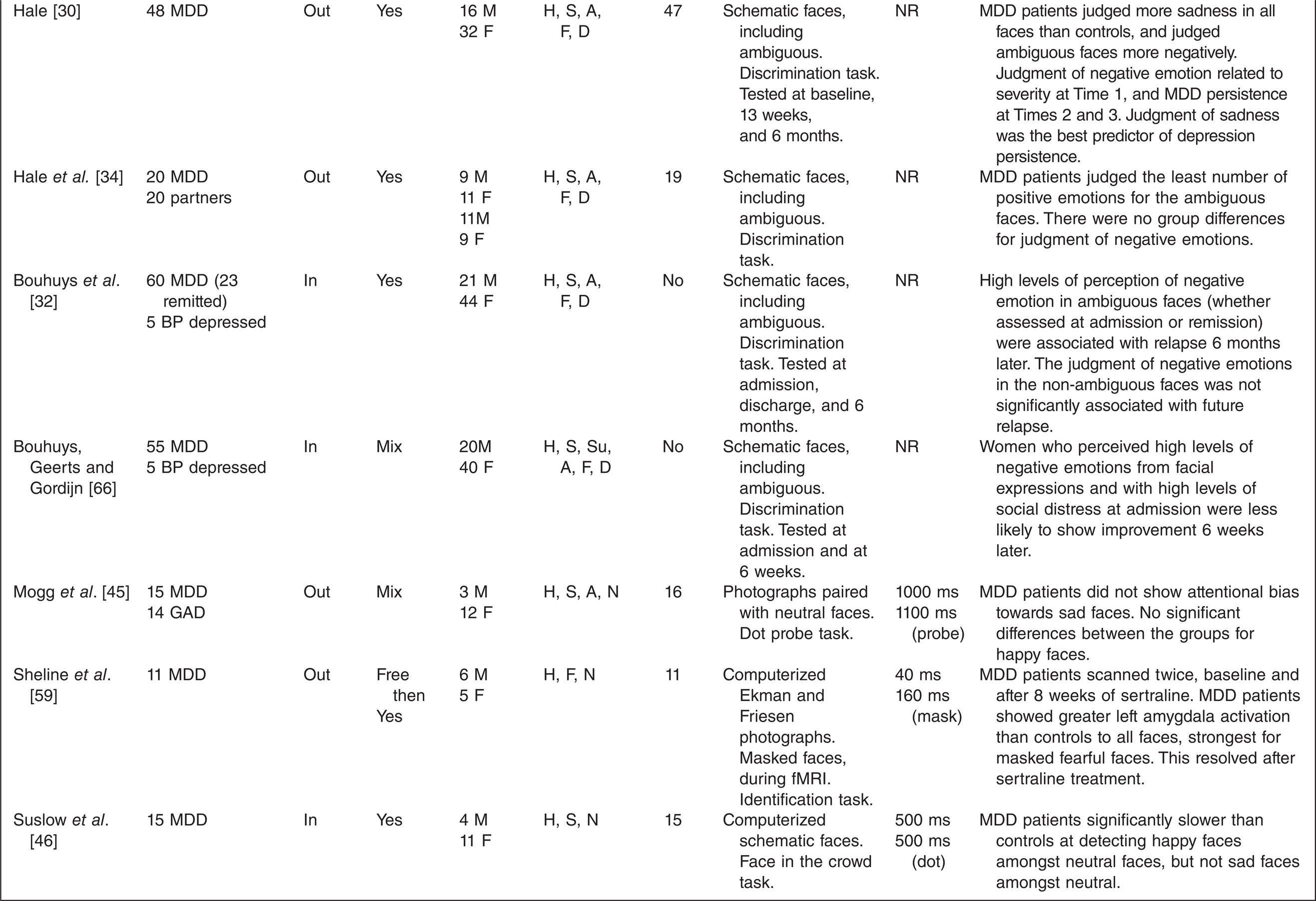
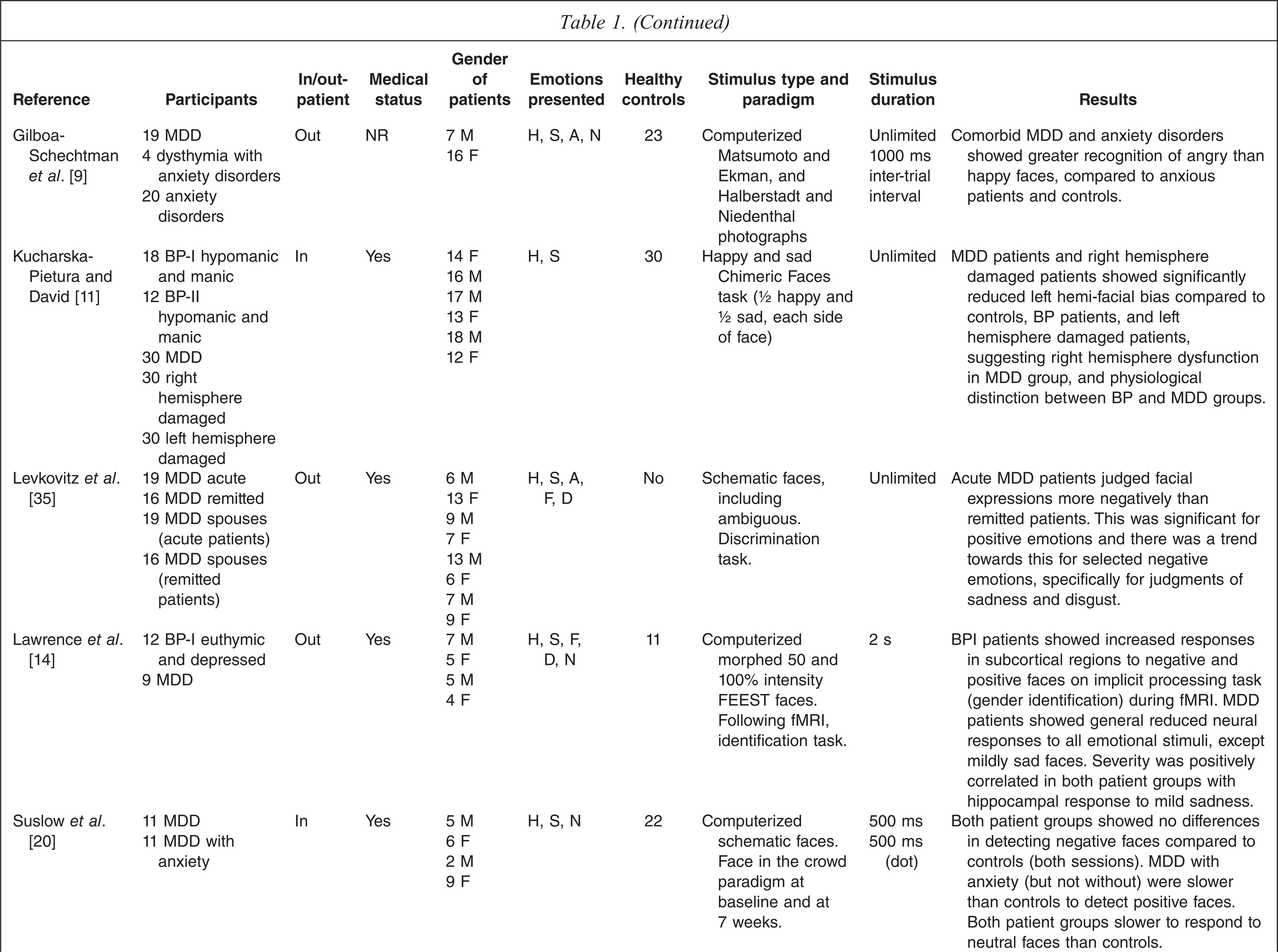
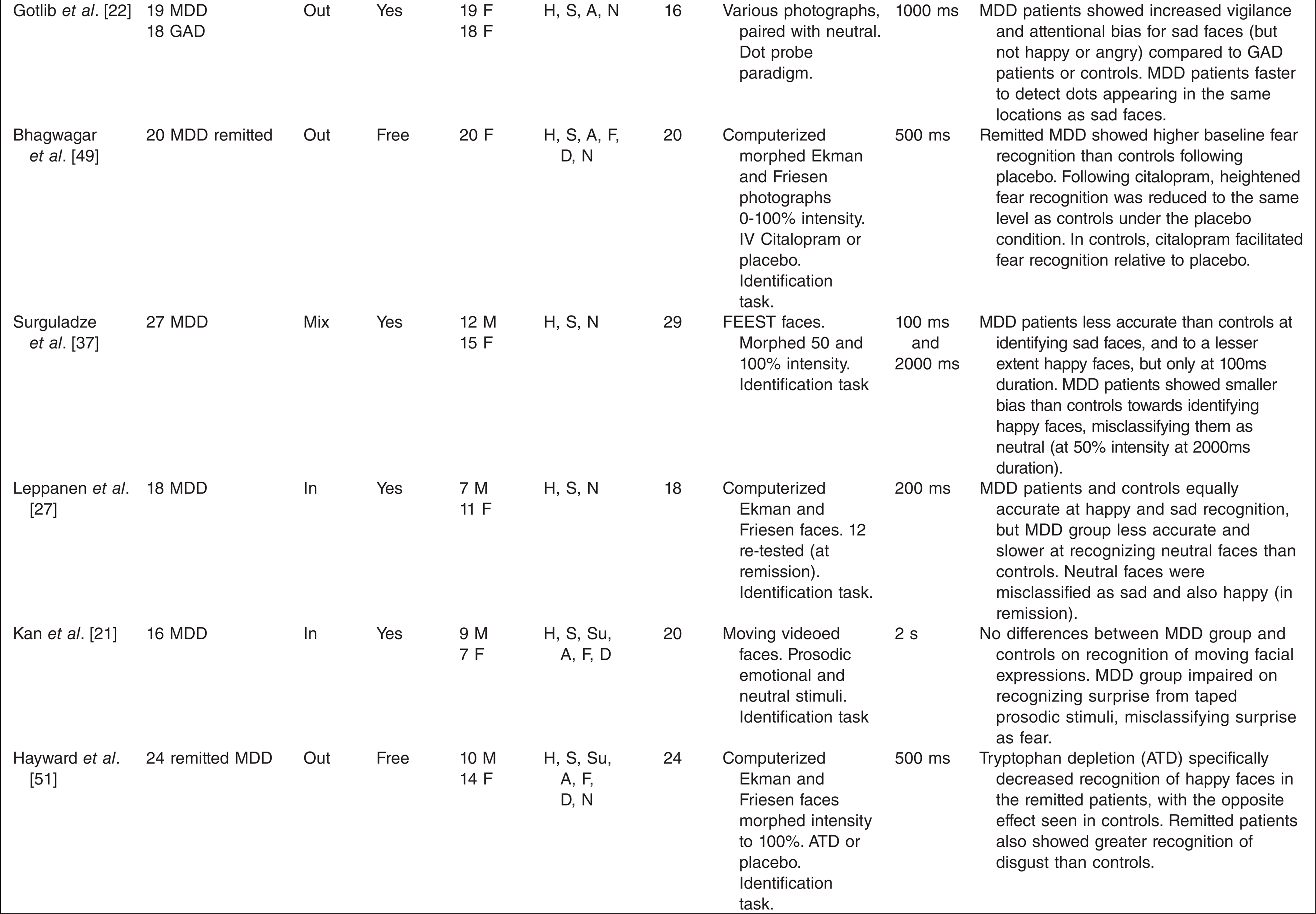
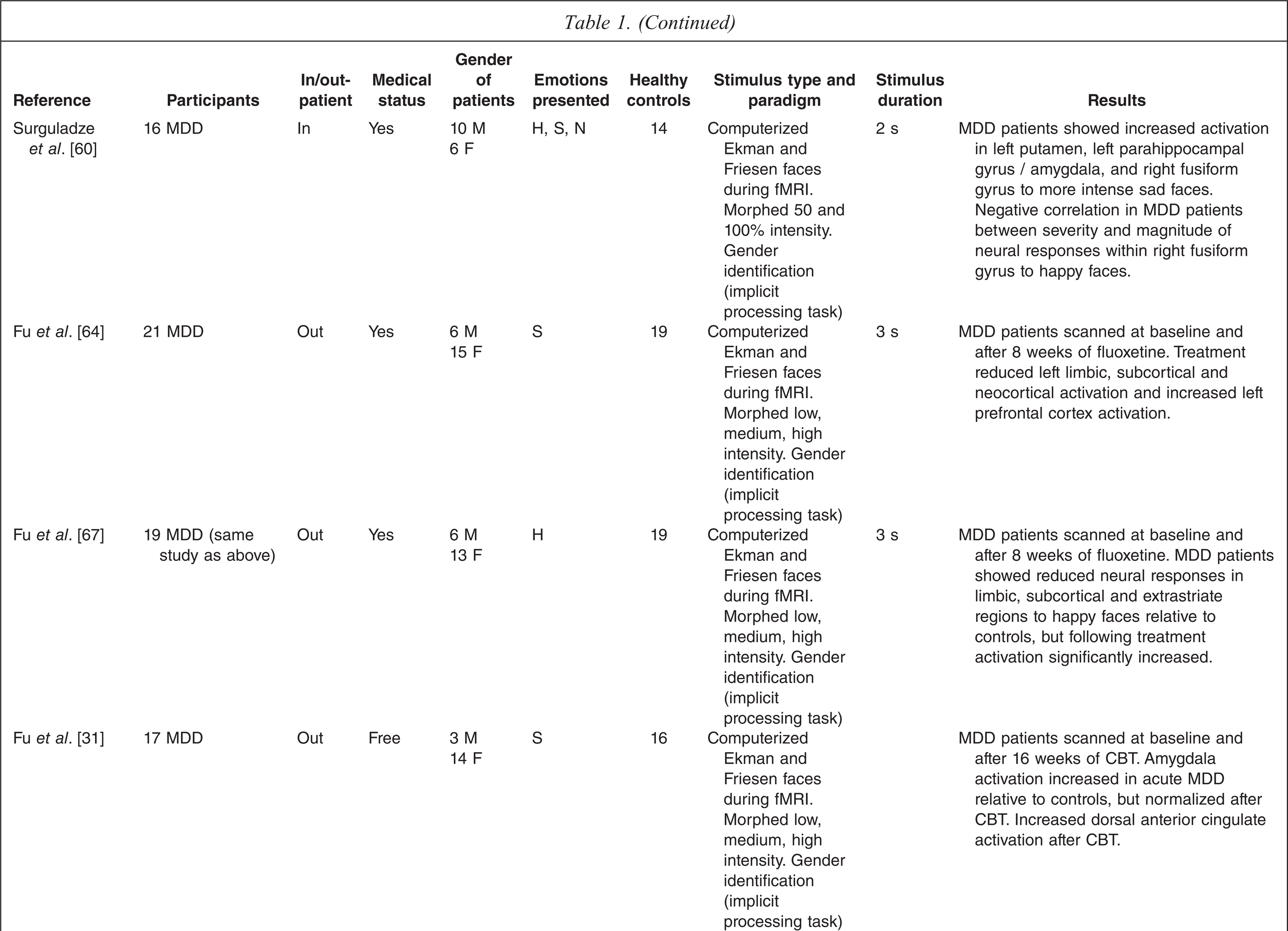
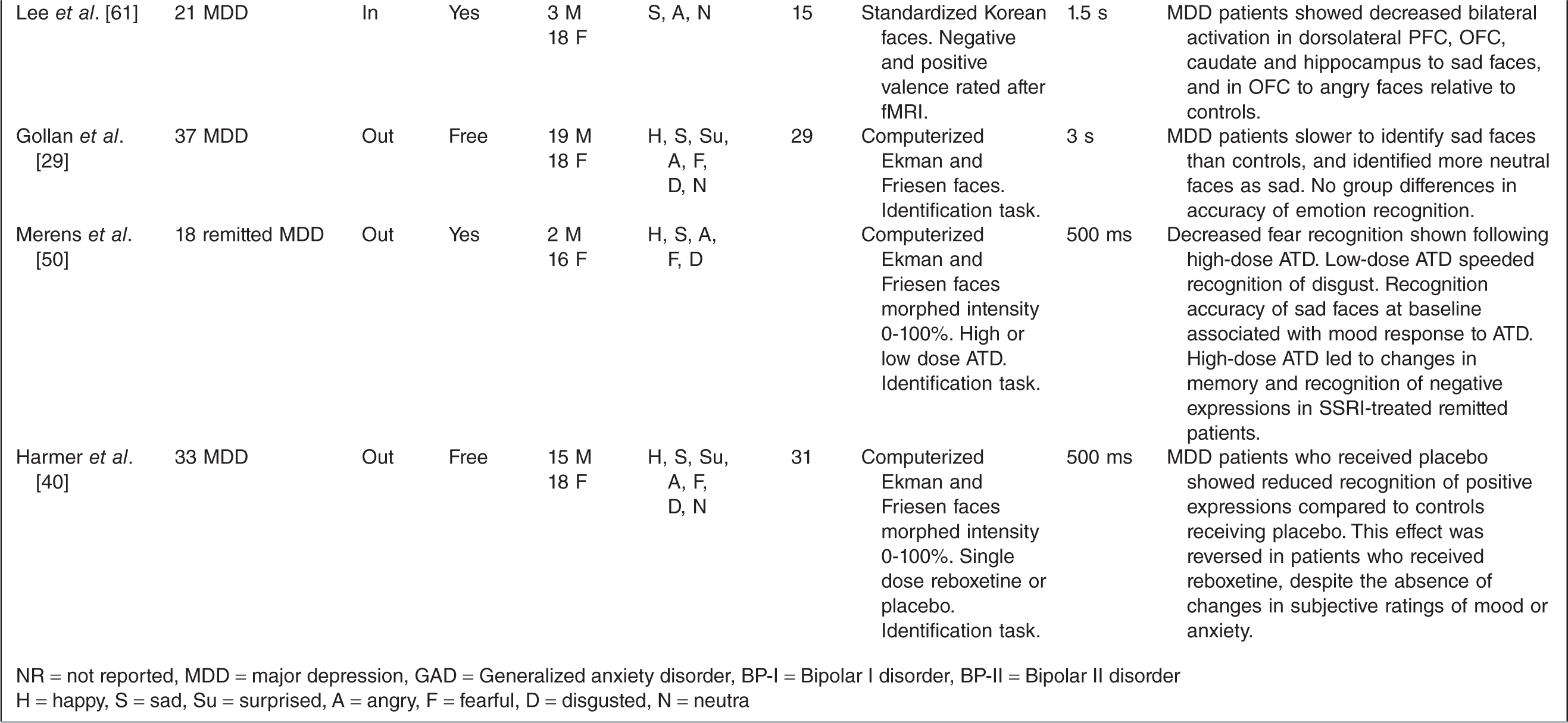
NR = not reported, MDD = major depression, GAD = Generalized anxiety disorder, BP-I = Bipolar I disorder, BP-II = Bipolar II disorder
H = happy, S = sad, Su = surprised, A = angry, F = fearful, D = disgusted, N = neutra
Methodology of studies of facial emotion processing in major depression
The methodology of studies of facial emotion processing impacts crucially on the findings. Clinical aspects of methodology have been previously reviewed in relation to neuropsychological functioning [5] and are likely to have similar implications in studies of facial emotion processing. Studies of facial emotion processing in major depression have used mixed clinical groups [6–8] whereas others have not reported the medication status of clinical groups [9,10], or controlled for medication effects [11]. Several studies have examined facial emotion processing in patients with bipolar disorder; however, most studies have involved manic [12] or euthymic patient groups [13] or combined groups of euthymic and depressed bipolar patients [14]. No studies have separately investigated differences between bipolar and unipolar depression.
There are also important methodological issues regarding the testing paradigms which are used to assess facial emotion processing. For example, there are variations in the emotions portrayed, the type of stimuli used (photographs or schematic representations, static or dynamic images), the length of stimulus presentation, the complexity of the tasks, and the use of control tasks to investigate the separable aspects of facial emotion processing. Statistical methods used to determine specificity of results have also varied between studies, as have sample sizes, with the risk of type II errors being high in most studies. The range of testing paradigms used will be discussed in the separate sections of the review.
Statistical methodology
An important issue in studies of facial emotion processing in major depression is whether abnormalities are specific to individual emotions. Such specificity may have important implications; firstly, indicating particular neuroanatomical abnormalities, and secondly, having effects on the pattern of symptoms seen in a disorder. It is therefore important to use appropriate statistical techniques to determine specificity. The finding of a statistically significant difference between a patient group and a control group in the perception of an emotion implies a group difference in perception of that emotion. However, finding a significant difference in the perception of one emotion but not others does not imply specificity. Specific differences can only be inferred statistically by an interaction between experimental group and emotion in an analysis of variance, which should be the method used to examine such specificity. An alternative approach is to examine the effect sizes of differences between groups on each specific emotion and to compare these without using further statistical analysis.
Even if specificity is confirmed statistically, this does not necessarily have neurobiological implications and may simply be a function of the properties of the task. The perception of different emotions is not equally easy. For instance, healthy individuals are generally better at perceiving happiness than other emotions [15] as the presence of a smile makes happiness easier to detect than other emotions [16]. Therefore, differences between groups in perception of one emotion compared with another may simply be due to a differential sensitivity of the test for that emotion.
A related issue is that of statistical power. Many studies of facial emotion processing in major depression include small numbers of participants [8,10,17–22], giving rise to a high likelihood of type II errors.
Behavioural studies of facial emotion processing in major depression
Most studies of facial emotion processing in major depression have focused on (i) comparisons between accuracy in recognizing sad versus happy expressions; (ii) negative response bias; specifically an increased tendency to interpret neutral, ambiguous or other emotional expressions negatively, or (iii) attentional bias towards or away from the recognition of sad or happy expressions. The following sections will therefore examine these studies, in the same order. Each section will begin with a description of the paradigms used in the studies.
Paradigms used to investigate facial expression recognition accuracy
Emotion identification and discrimination paradigms have been used to investigate recognition accuracy of emotional expressions, specific error biases (misclassification errors), and recognition memory biases. Identification and discrimination paradigms involve randomly ordered presentation of schematic or photographed faces in a booklet or on a computer screen. Duration of presentation may be fixed or unlimited. Identification paradigms involve participants labelling the emotional content of individual facial expressions. Discrimination paradigms involve participants judging whether pairs of facial expressions contain the same or different emotions, or judging the intensity of individual expressions. Identification and discrimination paradigms involve a fixed-response format, in which response keys or cards from a fixed set of emotional labels are selected. Accuracy, type of misclassification errors, and response speed are the main outcome measures in identification and discrimination paradigms.
Recognition accuracy of sad and happy facial expressions in major depression
Cognitive theories of major depression [23] are of relevance to the processing of social stimuli, such as facial expressions of emotion. Such theories suggest that deficits in emotion recognition, specifically of happy expressions, may contribute to an overall negative mood state and more negative social interactions. In a study investigating recognition accuracy only of happy, sad and fearful expressions, depressed patients were as accurate as controls in recognizing sadness but not happiness or fear [24], although a statistical analysis of specificity to happiness and fear was not conducted. Rubinow and Post [8] used a matching task that involved matching a series of photographs of faces with one of seven photographs most closely resembling the same affect. In contrast to the finding by Mandal and Palchoudhury [24], the mixed group of depressed unipolar and bipolar patients in this study made significantly fewer correct matches for sad and interested faces than healthy controls, with depressed patients scoring incorrectly on more than half of the sad face-matching items.
Mikhailova et al. [19] used a masking paradigm to investigate accuracy, as well as the role of the right and left hemispheres in facial emotion processing, in patients with major depression, patients with schizotypal personality disorder and healthy controls. Schematic sad, neutral, and happy faces were presented, followed by a masking stimulus displayed long enough to be consciously perceived (920 ms) to the left or right visual field. Patients with major depression were significantly less accurate at recognizing sad and happy expressions compared with the other two groups. In remission, there was significant improvement in recognition accuracy of sad faces, but only when presented to the left visual field, suggesting an improvement in right hemisphere functioning.
Overall, inaccuracy in the recognition of happy facial expressions has not been consistently established, with some studies suggesting the impairment is in recognizing both emotions (happiness and sadness) and some suggesting a specific deficit for sadness rather than happiness.
Chimeric faces (photographs of open mouthed smiles with neutral facial expressions, joined at the vertical meridian) have been used to investigate hemispheric perceptual biases. These have been shown to elicit a perceptual bias to the left hemisphere, with right-handed individuals perceiving smiles to their left as happier. Kucharska-Pietura and David [11] used a chimeric faces task comprising half-happy, half-sad schematic drawings to investigate lateral hemispheric perceptual bias in groups of patients with major depression, hypomania, right or left hemisphere damage, and healthy controls. Depressed patients showed a significantly weaker left hemispheric bias than the other groups, whereas the hypomanic bipolar patients were similar to controls, suggesting a possible difference in hemispheric activity in major depression.
These studies provide some support for the hypothesis of a mood-congruent impairment in facial emotion processing in major depression, in which impaired processing of emotions involves those most relevant to depression (i.e., happiness and sadness). Other studies, however, have found global deficits of facial emotion processing that are not selective to sadness or happiness [10,25,26] or no accuracy deficits in recognizing sad or happy expressions in major depression [21,27–29]. The data at present are therefore inconsistent. Whether there is a particular abnormality related to specific involvement of right or left hemisphere is likewise unclear.
Negative response bias in interpretation of facial expressions in major depression
A negative bias in facial emotion processing, specifically an increased tendency to interpret ambiguous, neutral, or other emotional expressions negatively, may contribute to impaired interpersonal functioning in major depression [30]. Several studies have reported negative response biases in patients with major depression.
Interpretation of ambiguous facial expressions
Cognitive theories of depression propose that ambiguity may have a causal role in the maintenance of depression because ambiguous events and situations are more likely to be experienced as negative [23,31]. Hence, it has been suggested that judgement of ambiguous facial expressions may be most affected in major depression [32]. Several studies have investigated interpretation of ambiguous facial expressions in major depression using schematic drawings conveying mixed emotional states [7,30,32–35]. All studies have shown that depressed patients (including mixed groups of both unipolar and bipolar depressed patients) tend to judge ambiguous facial expressions negatively. With the exception of the studies by Hale [30] and Hale et al. [34], however, none of these studies included healthy control groups.
Interpretation of neutral facial expressions
Neutral facial expressions may provide another means of evaluating interpretative biases associated with ambiguous social information [36], yet only one study has investigated responses to neutral facial expressions in major depression. Leppanen et al. [27] found that depressed patients did not differ from healthy controls in their ability to accurately recognize sad and happy facial expressions, but they were less accurate at recognizing neutral expressions. Specifically, they misclassified more neutral expressions as sad, suggesting a negative interpretative bias. Other studies have used neutral facial expressions as a control condition for other emotions, and these have also found evidence of a negative interpretative bias in depressed patients [37,38] or found that they are slower to respond to neutral expressions compared with emotional expressions [20,27].
Overall, there is consistent evidence that ambiguous or neutral facial expressions are more likely to be interpreted negatively (i.e. more likely to be interpreted as sad and less likely to be interpreted as happy) in major depression. This fits with findings of enhanced memory for negative material in memory tasks in major depression [39]. It has been suggested that an important effect of successful antidepressant treatment is to reverse this negative bias [40]. Current evidence to support this mainly comes from pharmacological manipulations in healthy individuals [4,41,42]. However, there is little evidence of this in depressed patients apart from one study showing that reboxetine reverses the bias in depression [40] and the functional imaging data reviewed in a later section, which suggests that brain activation in response to facial expressions normalizes with successful treatment of major depression.
Negative interpretation of emotional facial expressions
In addition to the studies that have found a negative interpretative bias for ambiguous and neutral facial expressions in major depression, other studies have reported a negative bias towards interpreting other emotional facial expressions. In an early study, Mandal and Bhattacharya [43] found that patients with major depression were less accurate than healthy controls at recognizing the six basic emotions; however, there was no statistical analysis of specificity in this study. Analysis of the errors suggested that the depressed group were more likely to misclassify the other emotions as sad than as any other emotion. Using a facial emotion discrimination task, Gur et al. [6] found that compared with healthy controls, a mixed group of unipolar and bipolar depressed patients were more likely to misinterpret neutral faces as sad, and happy faces as neutral. Surguladze et al. [37] also reported a response bias away from happy facial expressions in depressed patients relative to healthy controls. In this study, patients demonstrated a tendency to label happy expressions as neutral, but only those of medium intensity (50%) and at longer stimulus presentations of 2000 ms compared with 100 ms presentations. Overall, these studies provide reasonably consistent evidence of misclassification of emotional expressions to more negative emotions in major depression.
Attentional biases towards negative facial expressions in major depression
Even if recognition accuracy of facial emotions in major depression was intact, it could be argued that there are more subtle abnormalities such as attentional biases which could still influence social interactions. Studies using various facial emotion processing paradigms have attempted to investigate this.
Dot probe detection paradigms [44] involve presentation of a fixation cross or a dot on a computer screen, which is replaced by a pair of emotional and neutral faces side by side. Immediately after presentation of the faces, a probe (triangle, dot or arrow) is presented in the position of one of the preceding faces. Participants judge whether the probe appeared on the left or right side of the screen using two response keys. Attentional biases are measured by the direction and latency of the initial eye movement in response to the faces, and by manual reaction time to probes replacing the facial stimuli after their onset. Using a dot probe paradigm in patients with major depression, generalized anxiety disorder and healthy controls, Gotlib et al. [22] found that relative to the other two groups, depressed patients showed an attentional bias towards sad facial expressions compared with happy and fearful expressions, or happy and angry expressions. However, in an earlier study using a similar paradigm and similar groups, Mogg et al. [45] failed to find any differences when comparing responses to sad, happy and angry expressions. Although the sizes of the groups were similar in both these studies, patients in the Gotlib et al. [22] study were all female, compared with patients in the Mogg et al. [45] study who were male and female.
In detection paradigms such as the ‘face in the crowd’ paradigm, participants scan a group of schematic facial expressions and judge whether they are all the same or whether one or more is different. In half of the presentations all faces have the same neutral expression, and in the other half one positive (happy) or one negative (sad or threatening) expression appears amongst neutral faces. Same–different responses are selected using response keys, and response speed for correct responses to emotional valence is measured. Using this paradigm, Suslow et al. [46] found no differences between depressed patients and healthy controls on accuracy of detecting sad expressions, but depressed patients were significantly slower at responding to happy expressions, suggesting an association between depressed mood and reduced attention towards positive expressions. In a more recent study using the same paradigm, Suslow et al. [20] examined the impact of comorbid anxiety disorders on facial emotion processing in major depression. They found that depressed patients with comorbid anxiety disorders (but not major depression only) were slower at responding to happy expressions than healthy controls, suggesting that anxiety may play a role in processing deficits for happy facial expressions.
Overall, two studies directly support the hypothesized attentional bias away from positive and towards negative facial expressions, and one study supports this but only in patients with comorbid anxiety disorders. One study fails to show attentional bias. It should be noted, however, that these are complex paradigms which may be particularly susceptible to variability.
Recognition of other basic emotional expressions in major depression
While the review has focused on studies examining processing of happy, sad, neutral and ambiguous facial expressions, human emotional processing is complex. In major depression, abnormalities may be more complex than a bias towards negative emotional interpretation. For instance, studies have shown activation of the amygdala and hypothalamic-pituitary-adrenal (HPA) axis in major depression, with the suggestion that at least some forms of major depression may involve features of an abnormal stress response [47]. This could then be hypothesized to potentiate identification of, or bias towards threat-related emotions such as anger and fear. Below we review studies examining the other basic emotions.
Fear
Relatively few behavioural studies have examined recognition of facial expressions of fear in major depression. In a study using videotapes of facial expressions, no differences in recognition accuracy of fear (or any other emotion) were found between currently depressed patients and healthy controls [21]. In a study involving groups of individuals at high and low genetic risk of developing depression, those at high genetic risk were significantly faster to recognize fearful facial expressions than those at low genetic risk of developing depression [48].
Other studies have investigated processing of fearful facial expressions in remitted depressed patients following pharmacological manipulation of serotonin levels. Bhagwagar et al. [49] found that remitted, unmedicated depressed females showed increased baseline levels of fear recognition relative to healthy females, but following infusion with citalopram this effect normalized, with a reduction in fear recognition in depressed females. Thus, the increased recognition of fear was concluded to represent a trait marker for MDD that is normalized with antidepressant treatment. Merens et al. [50] reported that high dose acute-tryptophan depletion (ATD) increased depressive symptomatology and reduced the recognition of fear in remitted depressed patients. On the other hand, low dose ATD showed limited effects with only speeded reaction times to the recognition of disgust and no changes in depressive symptoms. An overall analysis examining tryptophan dose differences across all individual emotions was not conducted, meaning that the specificity of the deficit to recognizing fear cannot be firmly concluded. The findings that both a single dose of citalopram [49] and high dose ATD [50] resulted in the reduced recognition of fear in remitted MDD patients is surprising, given that these methods raise and lower serotonin levels respectively. Overall, there is limited preliminary evidence of enhanced fear recognition as a state effect of major depression and some suggestion of an effect of changes in serotonin function on this.
Anger
Several studies have investigated responses to angry facial expressions in major depression amongst other emotional expressions, although only two have reported findings specific to anger. Both studies used dot probe paradigms to investigate attentional biases towards threatening (angry or hostile) expressions in groups of patients with major depression, generalized anxiety disorder, and healthy controls but neither reported the hypothesized bias towards angry expressions in the depressed groups [22,45].
Disgust
Several studies have included expressions of disgust in facial emotion processing paradigms, but most have found no group differences between depressed patients and healthy controls for disgust recognition [21]. Only one study has reported a difference. In this study, remitted depressed patients and healthy controls were administered either tryptophan-free or placebo drinks before completing a facial emotion identification task. The remitted patients showed enhanced recognition of disgust relative to controls, regardless of whether they had received the tryptophan depleting drink or placebo [51]. Harmer et al. [52] reported a similar finding in a group of euthymic medicated patients with bipolar disorder, and although this may indicate a general enhancement of disgust recognition in the euthymic phase of mood disorders, other studies have failed to replicate this with euthymic patients with bipolar disorder [12,13].
Surprise
Fewer studies have included expressions of surprise in facial emotion processing paradigms, and only one study has reported group differences specific to recognition of surprise between patients with depression and healthy controls [40]. This study examined the effects of a single dose (4 mg) of reboxetine on emotional processing in depressed patients and healthy controls. The depressed patients who received placebo (but not reboxetine) showed poorer recognition of surprised and happy facial expressions than HCs who received placebo.
State versus trait effects of facial emotion processing in major depression
Studies investigating the extent to which abnormalities in facial emotion processing in major depression are purely state related or whether they represent trait markers of the illness have produced mixed findings. Interpretation of these findings is difficult, due to the methodological variations between studies.
As noted previously, studies in individuals at high genetic risk for depression [48] and in remitted depressed patients [49] suggest trait-related abnormalities in fear processing. In addition, several other studies have investigated changes in processing of other facial emotions by longitudinally assessing depressed patients in acute and remitted states. Mikhailova et al. [19] found that remitted depressed patients showed significant improvement in recognition of happy and sad facial expressions over time, and Hale [30] found that judgement of sadness in general and in ambiguous schematic faces was predictive of depression persistence at two later time points, with the judgement of sadness in ambiguous faces being the best predictor. In a study investigating associations between relapse of depression and emotion perception, Bouhuys et al. [32] examined whether acute depressed state affected the perception of facial emotions in a group of male inpatients whose depression remitted. Severity of depression at admission was positively correlated with the perception of negative emotions in ambiguous facial expressions, and perception of ambiguous expressions became less negative over time. Bouhuys et al. [32] concluded that bias in the negative perception of ambiguous faces is an enduring vulnerability factor to major depression and that depressed mood amplifies the effect. Taken together, these findings provide some support for a state-dependent bias towards perceiving ambiguous facial expressions as negative in major depression.
Other studies support the view that impaired facial emotion processing is related to trait deficits. Using a prospective longitudinal design, Bouhuys et al. [33] investigated the role of impaired recognition of facial expressions in predicting the persistence of depression. Patients who perceived less sadness, anger and rejection in ambiguous schematic facial expressions at baseline were less likely to improve after 6 weeks and 30 weeks. Non-remitted patients perceived less sadness than remitted patients in ambiguous faces, and the perception of sadness did not change over time for both remitted and non-remitted patients. This finding therefore suggests that the deficit in perceiving sadness in ambiguous facial expressions in depression may be trait related.
The study by Suslow et al. [20] discussed previously used a face in the crowd task to test depressed patients (some of whom had a comorbid anxiety disorder) before and after therapy and found that the patients with a comorbid anxiety were slower to respond to happy facial expressions during remission relative to depressed patients without an anxiety disorder and healthy controls. Both groups of depressed patients were slower to respond to neutral expressions than controls, and this persisted in remission from depression. These findings suggest that even when stabilized, depressed patients experience slowed motor functioning or slowed visual scanning ability, although it is possible this could be due to medication effects as patients in both studies were medicated. Leppanen et al. [27] found that depressed patients and healthy controls were equally accurate in recognizing happy and sad facial expressions at baseline, but depressed patients recognized neutral expressions less accurately and more slowly than either happy or sad expressions. Similar to Suslow et al. [20], impaired processing of neutral expressions was evident after symptom remission. Analysis of errors showed that, relative to healthy controls, depressed patients misclassified neutral expressions as sad, both when acutely depressed and when in remission. They also misclassified neutral expressions as happy, but only when in remission, suggesting that although impaired processing of neutral expressions may reflect a trait effect of major depression, valence attributed to neutral expressions may partly depend on current mood state.
Overall, evidence is ambiguous at present as to whether deficits in facial emotion processing in major depression are state related or whether they represent trait markers of the illness. Some studies have reported an improvement of some aspects of facial emotional processing during successful treatment whereas others have reported impairment of other aspects following treatment, and in a group at high genetic risk for depression.
Neural correlates of facial emotion processing in major depression
Facial emotion processing paradigms have increasingly been used in functional imaging studies to investigate the neural basis of facial emotion processing in healthy individuals and patient groups with various neurological or psychiatric disorders. Studies have generally been small and this may be a limitation in major depression, which is a heterogeneous condition. However, combining knowledge of normal brain activation in response to various aspects of facial emotion processing with behavioural data from much larger scale studies may be very useful in examining the neurobiology of facial emotion processing in major depression.
The neurobiological basis of fear has been studied most extensively. Many studies have investigated the amygdala's role in normal perception of fear, and several have provided evidence for its role in conscious and non-conscious facial emotion processing of fear [53–55]. Morris et al. [56] and Phillips et al. [54] found that neural responses to fearful facial expressions were significantly greater in the left amygdala compared with other emotional expressions in groups of healthy individuals. There is still debate, however, about whether the amygdala is selectively involved in perception of fear, or whether it contributes to perception of a range of emotions. Recent evidence suggests that the amygdala may respond to emotionally salient information, regardless of emotional valence or type of task [57], but that it may have a special role in the accurate recognition of facial emotions that convey imminent threat to survival [58].
Studies investigating the neural correlates of facial emotion processing in major depression have produced mixed findings, and only one study has reported findings specific to processing of fear in major depression. Sheline et al. [59] used a backward masking paradigm to investigate the role of the amygdala in non-conscious responses to fearful, happy, and neutral facial expressions in patients with major depression and healthy controls. Amygdala activation was assessed before and after eight weeks treatment with the SSRI, sertraline. There were no between-group differences for right amygdala activation, but depressed patients showed greater left amygdala activation to all emotional expressions. The greatest effect was shown for the masked fearful faces, suggesting that initial processing of fearful emotional stimuli occurs outside of conscious awareness. Changes in activation associated with treatment in Sheline et al.'s study are discussed in the following section.
Lawrence et al. [14] compared responses within subcortical and prefrontal cortical regions to mild and intense facial expressions of fear, happiness, and sadness in a group of patients with major depression and a mixed group of euthymic and depressed patients with bipolar I disorder. Differential patterns of neural activation were revealed between the two patient groups. The group with major depression showed an overall pattern of diminished neural responses to all emotions except mild sadness. Surguladze et al. [60] reported a pattern of increased neural responses in subcortical areas to sad but not happy expressions in their study of depressed patients compared with healthy controls. Lee et al. [61] found that depressed patients showed decreased activation in the frontal cortex areas and the hippocampus in response to sad facial expressions compared with healthy controls, but in contrast with findings by Surguladze et al. [60], patients in this study did not show increased activation in subcortical regions in response to sad facial expressions. It is likely that sample characteristics, small sample sizes and differences in testing paradigms may account for some of the differences in findings.
A study by Lee et al. [61] examined neural responses to angry facial expressions in major depression. Relative to healthy controls, depressed patients showed reduced bilateral activation in the medial and inferior orbitofrontal cortex. This is consistent with the opposite finding reported in an earlier study of healthy individuals, who showed increased orbitofrontal cortex activation selectively in response to angry, but not sad facial expressions [62].
Overall, the findings could be interpreted as fitting with a model of brain circuitry in major depression which hypothesizes an over-activity of more primitive emotion processing centres or circuits including the amygdala [63], with reduced activation of higher processing prefrontal cortical areas. This may particularly be the case for threat-related emotions such as fear.
Changes in brain activation following treatment for major depression
Several studies have investigated neural responses to emotional facial expressions over the course of treatment for major depression. The study by Sheline et al. [59] discussed earlier, assessed amygdala activation before and after eight weeks of treatment with sertraline in depressed patients. Following successful treatment, the patients in this study showed reduced bilateral amygdala activation to all emotional expressions, including the masked fearful faces, supporting the theory that reduced amygdala activation may be an important effect of antidepressant treatment. Fu et al. [64] showed that at baseline, depressed patients showed increased activation of the left amygdala and subcortical areas in response to sad facial expressions and reduced neural activation in subcortical regions in response to happy expressions relative to healthy controls. Following eight weeks of treatment with fluoxetine, the pattern of activation in response to happy expressions was reversed and the increased activation in response to sad expressions was significantly reduced. One study to date has used a facial emotion processing paradigm to investigate neural changes in patients with major depression following treatment with psychotherapy. Similar to studies involving pharmacological treatments, Fu et al. [31] found that depressed patients showed elevated amygdala–hippocampal activity in response to sad facial expressions relative to healthy controls during acute depression. Following 16 weeks of successful treatment with Cognitive Behavioural Therapy (CBT), the activity normalized. Treatment also appeared to affect dorsal anterior cingulate activity, which increased following CBT, an opposite effect seen for the healthy controls at follow up scanning.
Overall, functional imaging studies suggest abnormal neural activation in major depression and there is consistent evidence of at least a partial reversal of abnormal activation compared with healthy controls when depressed patients are treated with antidepressants or psychotherapy.
Summary of facial emotion processing in major depression
In spite of the methodological problems that complicate interpretation of studies, there appear to be some areas of relative consistency. Relative to healthy controls, patients with major depression show:
a negative response bias towards sadness, so that neutral and ambiguous expressions tend to be evaluated as more intensely sad or less happy;
increased vigilance and selective attention towards sad facial expressions and away from happy expressions;
reduced general accuracy of recognition of sad and happy facial expressions, although the evidence of specificity to these emotions is limited.
The findings suggest that aspects of the pattern of impairment may vary according to clinical state and response to treatments, but there may also be trait abnormalities. Studies of regional brain function have begun to reveal the relationships between these impairments and the specific brain structures and neural pathways involved in facial emotion processing in major depression. Many questions remain unanswered, however, and future research will need to address the methodological shortcomings discussed, relating to depression heterogeneity, testing paradigms and procedures, and the statistical methods used to analyse results.
Future research
In a condition which is clearly relatively heterogeneous, it is important that studies are large enough and patients well characterized to take into account and to investigate variations in the depression phenotype, such as severity, psychosis and current treatment.
Clearly different research groups have views regarding the best paradigms to investigate aspects of facial emotion processing. In the area of accuracy and misclassification errors, however, the field would benefit from studies using similar stimuli, for example, the Ekman and Friesen stimuli. This would enable data to be directly compared and even pooled.
Larger longitudinal studies of major depression would increase data on the effects of treatments on facial emotion processing, and thereby neurobiological changes which occur with treatment. This would provide important information as to whether such changes may provide a sensitive marker of improvement in depressive symptoms. In particular, the most consistent finding has been of a negative response bias towards sadness in depression. Future studies should examine the course of this bias during treatment for and recovery from depression.
Footnotes
Acknowledgements