
Abstract
Keywords
Australia's recently released Fourth National Mental Health Plan [1] recognizes the pivotal role that carers play in the lives of people with mental disorders, and that carers have a range of needs. It explicitly recommends an expansion of the level and range of support for families and carers.
There have been several previous population-based Australian studies of carers of people with physical and/or mental disorders. These have differed in the way they have recruited and/or defined carers. In 1997, the Victorian Carers Project (VCP) conducted a longitudinal study of randomly selected householders of all ages, determining whether the selected individual qualified as a carer by asking ‘Does you or anyone else in your household take the main responsibility in caring for someone who is aged or who has a long-term illness, disability or other problem?’ [2] In 2003, the Australian Bureau of Statistics conducted the cross-sectional Survey of Disability, Ageing and Carers (SDAC), and defined a carer as ‘A person of any age who provides any informal assistance, in terms of help or supervision, to persons with disabilities or long-term conditions, or older persons (i.e. aged 60 years and over)’ [3]. In 2006, the Australian Institute of Family Studies conducted a one-off survey of a random sample of adults who received government carer payments. In 2007, Australian Unity and Deakin University joined forces with Carers Australia to conduct a special carers survey as part of the Australian Wellbeing Unity Index programme, and recruited carers from the membership lists of state and territory carers associations [4]. These studies have generated varying estimates of the proportion of Australians who care for someone with a physical and/or mental disorder. For example, SDAC, which is often taken as the ‘gold standard’ puts the figure at 13% [3], but it is not easy to disaggregate these estimates to calculate the proportion who care for someone with a mental disorder, at least from the published data. Without this information it is also difficult to profile those who care for someone with a mental disorder, to determine whether they have particular characteristics in common, what sort of mental disorders are experienced by those for whom carers provide care, and what the relationship is between the carer and the recipient of care.
There have been several more specific studies of selected samples of people who are caring for someone with a mental disorder, but these also need augmenting if our understanding of the experiences of carers of people with mental disorders is to be strengthened. The Mental Health Council of Australia recently conducted nationwide consultations with 1514 carers of people with mental disorders and found that they experienced a general lack of respect by others for their caring role and a particular unwillingness on the part of services to involve them in treatment planning despite their intimate knowledge of and close relationships with those they care for [5]. Other smaller scale Australian studies have focused on the problems experienced by carers of people with psychiatric diagnoses (most commonly schizophrenia), typically finding these to be greatest when their relatives have acute and/or severe symptoms, unmet needs or are at key points in an episode of care (e.g. discharge from an acute inpatient setting into the community), and alleviated by genuine involvement in treatment planning [6–11]. These studies point to the importance of particular issues for carers of people with mental disorders, but the representativeness of their samples limits the extent to which their findings can be generalized.
The current study drew on data from a nationally representative sample of Australian adults who took part in the National Survey of Mental Health and Wellbeing (NSMHWB), which was conducted by the Australian Bureau of Statistics (ABS) in 2007. The current study aimed to update existing knowledge by answering the following research questions: How many Australian adults are caring for a relative with a mental disorder? Are there particular socio-demographic and clinical characteristics that are associated with being a carer? What are the mental disorders experienced by relatives of carers, and what is the relationship of carers to these relatives? How do carers experience their care-giving role?
Method
Sampling and procedure
The NSMHWB was conducted in the latter part of 2007 by trained interviewers from the ABS. Survey respondents were identified from a stratified multistage probability sample of households generated by the ABS. Interviewers approached each household and used a set of household composition questions to identify all eligible residents (adults aged 16–85). They then applied a pre-determined algorithm to select one individual from the pool of eligible adults and invite him or her to participate. The algorithm was designed to recruit as representative as possible a sample of Australian adults. Individuals who agreed to take part were interviewed (in English) for an average of 90 minutes, and responded to questions from a structured survey instrument (see below). No further attempt was made to recruit from households of individuals who chose not to participate. This sampling strategy resulted in 8841 fully responding households (a response rate of 60%), representing a projected Australian adult resident population of 16 015 300. Further detail on the sampling and procedure is available elsewhere [12].
Survey instrument
The survey instrument was based on a modified version of the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI) and has also been described in detail elsewhere [12]. The survey was structured around a series of modules, one of which sought information about whether the respondent had any immediate family members who suffered a range of physical and mental disorders, and, if so, the degree to which their disorders affected the respondent's life (taking into consideration his or her time, energy, emotions, finances and daily activities). Those who stated that they had at least one relative with a mental disorder (with or without a physical disorder) and who indicated that this affected their lives ‘a lot’ or ‘some’ (as opposed to ‘a little’ or ‘not at all’) were deemed to be carers of people with mental disorders. Carers were asked a range of additional questions about the mental disorders experienced by the relative(s) for whom they were providing care, and about their experiences of acting as a care-giver.
A separate module elicited various types of socio-demographic information from respondents, enabling them to be profiled in terms of their sex, age, marital status, country of birth, and level of socio-economic disadvantage. Most of these variables are self-explanatory, with the possible exception of the last one. The level of socio- economic disadvantage was gauged using the Index of Relative Socioeconomic Disadvantage (IRSED), which classifies individuals into deciles reflecting comparative levels of disadvantage (low values) and advantage (high values), based on characteristics of the geographic location of their household [13].
Further modules examined issues to do with respondents’ general mental health, well-being and functioning. The presence or absence of lifetime diagnoses of affective disorders, anxiety disorders and substance use disorders were assessed using International Classification of Diseases (ICD-10) [14] criteria, and additional questions were used to gauge the presence or absence of symptoms in the past 12 months. Total and partial days out of (usual) role in the previous 30 were assessed by two questions which examined the number of days on which respondents were totally unable to perform their normal activities and/or had to cut down what did they did because of health problems. Psychological distress during the past 30 days was assessed via the Kessler Psychological Distress Scale (K10) [15].
Data analysis
The ABS provided us with data in the form of a confidentialized unit record file, and we conducted all analyses using STATA version 10.1 [16]. The majority of the analyses were descriptive. We conducted a binomial logistic regression analysis to compare carers and non-carers in terms of their socio-demographic and clinical characteristics. Prior to this analysis, candidate variables were assessed for multicollinearity by inspecting correlations between variables and other diagnostics including tolerance, variance inflation factors, and the condition index. All candidate variables meeting these criteria were simultaneously entered into a multivariate logistic regression analysis. Standard errors and 95% confidence intervals (CIs) were calculated using jack-knife repeated replication which provides unbiased estimates of the sampling error arising from complex sample selection procedures.
Results
How many Australian adults are caring for a relative with a mental disorder?
Figure 1 shows the data flows used to determine whether respondents identified themselves as having a role in caring for a relative with a mental disorder. Of the total sample, 3434 respondents (39.5%, 95% confidence interval (CI) = 37.9%–41%) stated that at least one of their relatives had a mental disorder. Of these, 1309 (38%, 95%CI = 35.2%–40.6%) indicated that they were caring for this relative (or these relatives) according to the definition presented above. This equates to 15% (95%CI = 13.8%–16.1%) of Australian adults being carers of people with mental disorders.
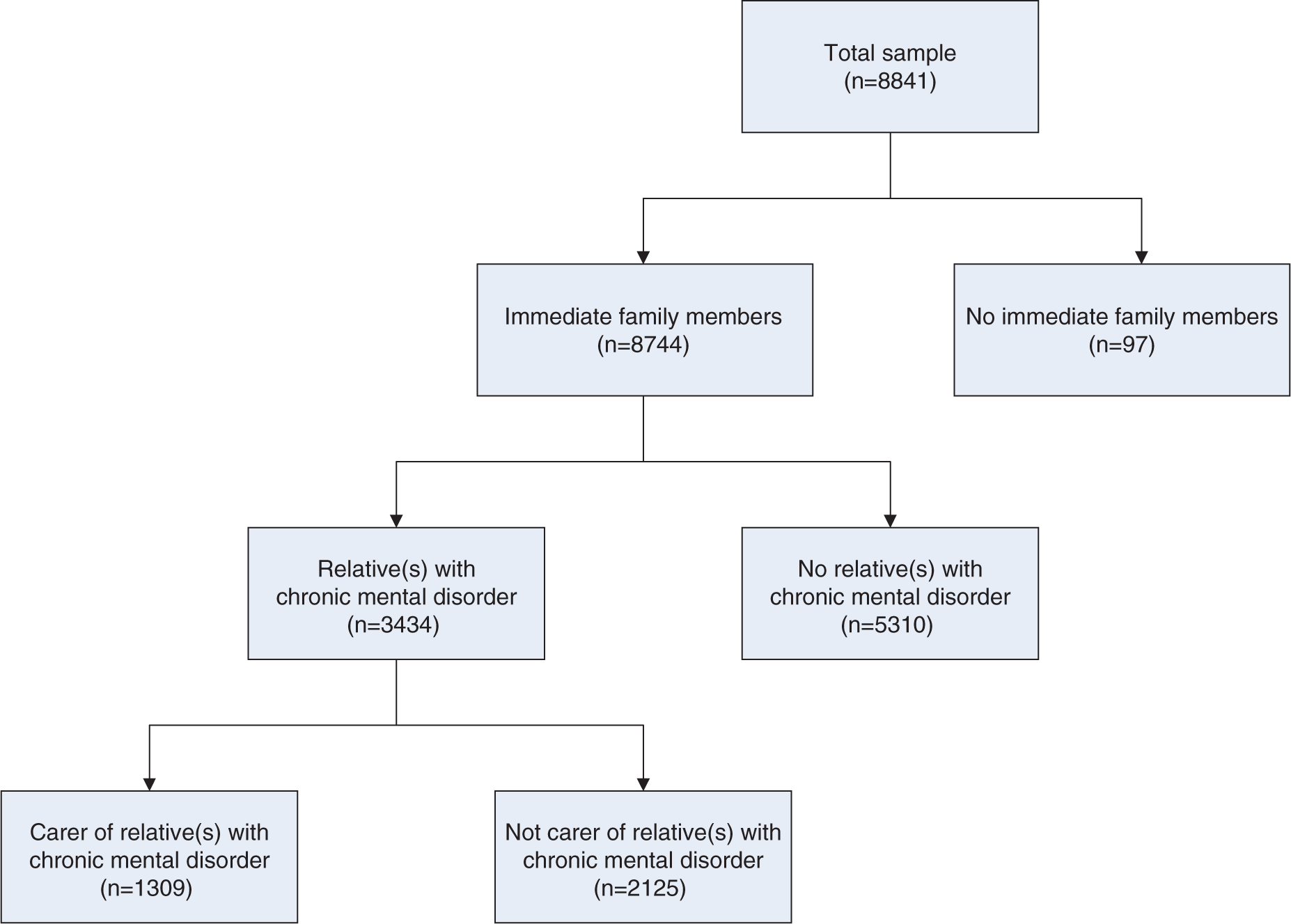
Flowchart used to determine respondents’ status as a carer of relative(s) with a mental disorder.
Are there particular socio-demographic and clinical characteristics that are associated with being a carer?
Table 1 profiles the 1309 people who identified as carers on a range of socio-demographic and clinical variables. Around two thirds of carers were female, and half were accounted for by those in the 16–34 and 35–44 age groups. Most commonly, carers were married and born in Australia. They were relatively evenly spread with respect to levels of advantage and disadvantage. Roughly two thirds of carers had experienced an affective, anxiety or substance use disorder at some point in their lifetime, and over half of these had experienced symptoms in the previous twelve months. Just under half had experienced at least one day out of role in the last 30 as a result of health problems, and the same proportion had experienced at least moderate distress levels during the same period.
Socio-demographic and clinical characteristics of carers of relative(s) with a mental disorder
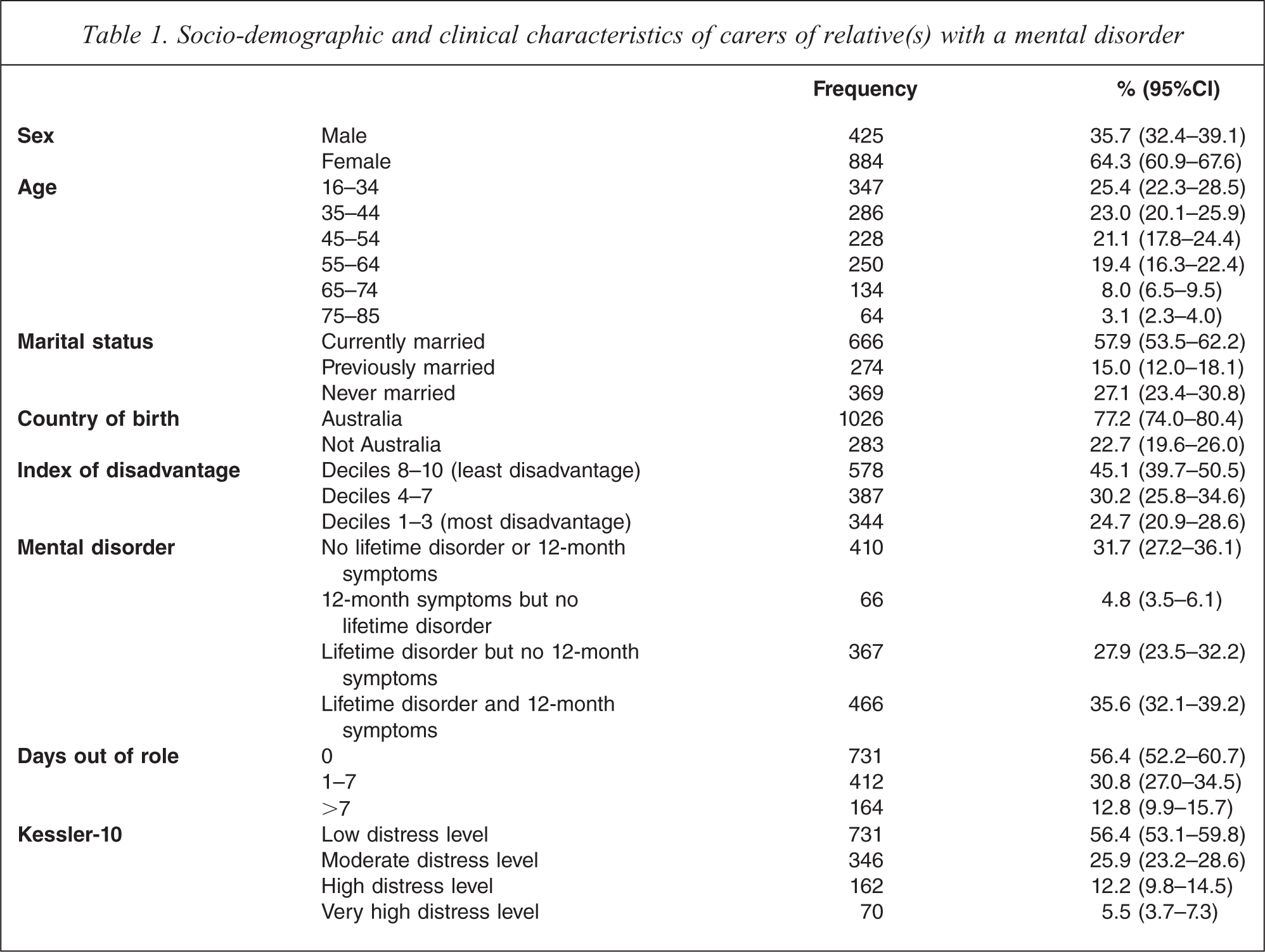
Table 2 shows the results of the multivariate logistic regression analysis, which considered whether particular socio-demographic and clinical factors were predictive of reported carer status. In terms of socio-demographic variables, after adjusting for all other variables in the model, females were significantly more likely to be performing a carer role than males (adjusted odds ratio (AOR) = 1.90, 95%CI = 1.57–2.29). Age was also associated with care-giving: compared with 16–34 year olds, 35–44 year olds were significantly more likely to be carers (AOR = 1.64, 95%CI = 1.29–2.10), as were 45–54 year olds (AOR = 1.66, 95%CI = 1.24–2.21) and 55–64 year olds (AOR = 2.24, 95%CI = 1.59–3.18). Having been previously married (as opposed to being currently married) and having been born outside Australia (as opposed to being born in Australia) were associated with decreased odds of performing a care-giving role (AOR = 0.76, 95%CI = 0.58–0.99; AOR = 0.77, 95%CI = 0.61–0.96), although these relationships were not as strong as those found for sex and age. Level of advantage or disadvantage was not predictive of carer status.
Predictors of carer status
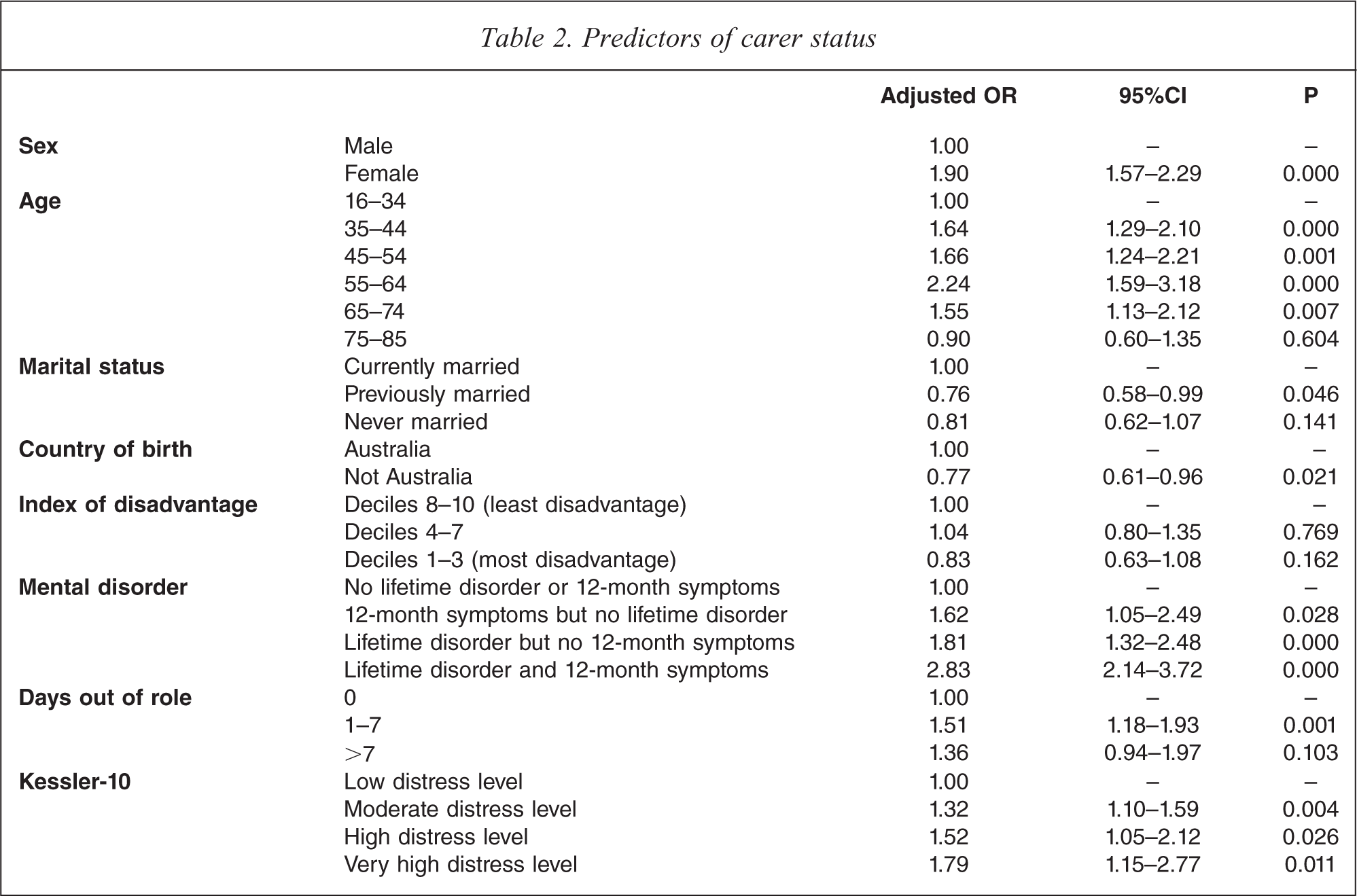
With respect to clinical characteristics, those who had experienced a mental disorder at some point in their lives and/or had experienced symptoms in the previous 12 months were significantly more likely than those with no history of mental disorder to be carers, with the combination of recent symptoms and past diagnosis conferring the greatest odds (AOR = 2.83, 95%CI = 2.14–3.72). People who had experienced 1–7 days out of role were significantly more likely to be acting as carers than people who had experienced no days out of role (AOR = 1.51, 95%CI = 1.18–1.93). Moderate, high and very high levels of distress were also significantly associated with care-giving (AOR = 1.32, 95%CI = 1.10–1.59; AOR = 1.52, 95%CI = 1.05–2.12; AOR = 1.79, 95%CI = 1.15–2.77).
What are the mental disorders experienced by relatives of carers, and what is the relationship of carers to these relatives?
Table 3 presents a cross-tabulation of the mental disorders experienced by relatives of carers. The table should be interpreted with some caution, because multiple responses were permissible. Not only could an individual have more than one relative with the same mental disorder (e.g. two sisters with an alcohol or drug problem), he or she could have one relative with several mental disorders (e.g. one sister with an alcohol or drug problem and depression). In addition, although each respondent was caring for at least one relative with a mental disorder, those with more than one relative with a mental disorder may or may not have been performing the role of care-giver for all of them.
Mental disorders experienced by relative(s) of carers
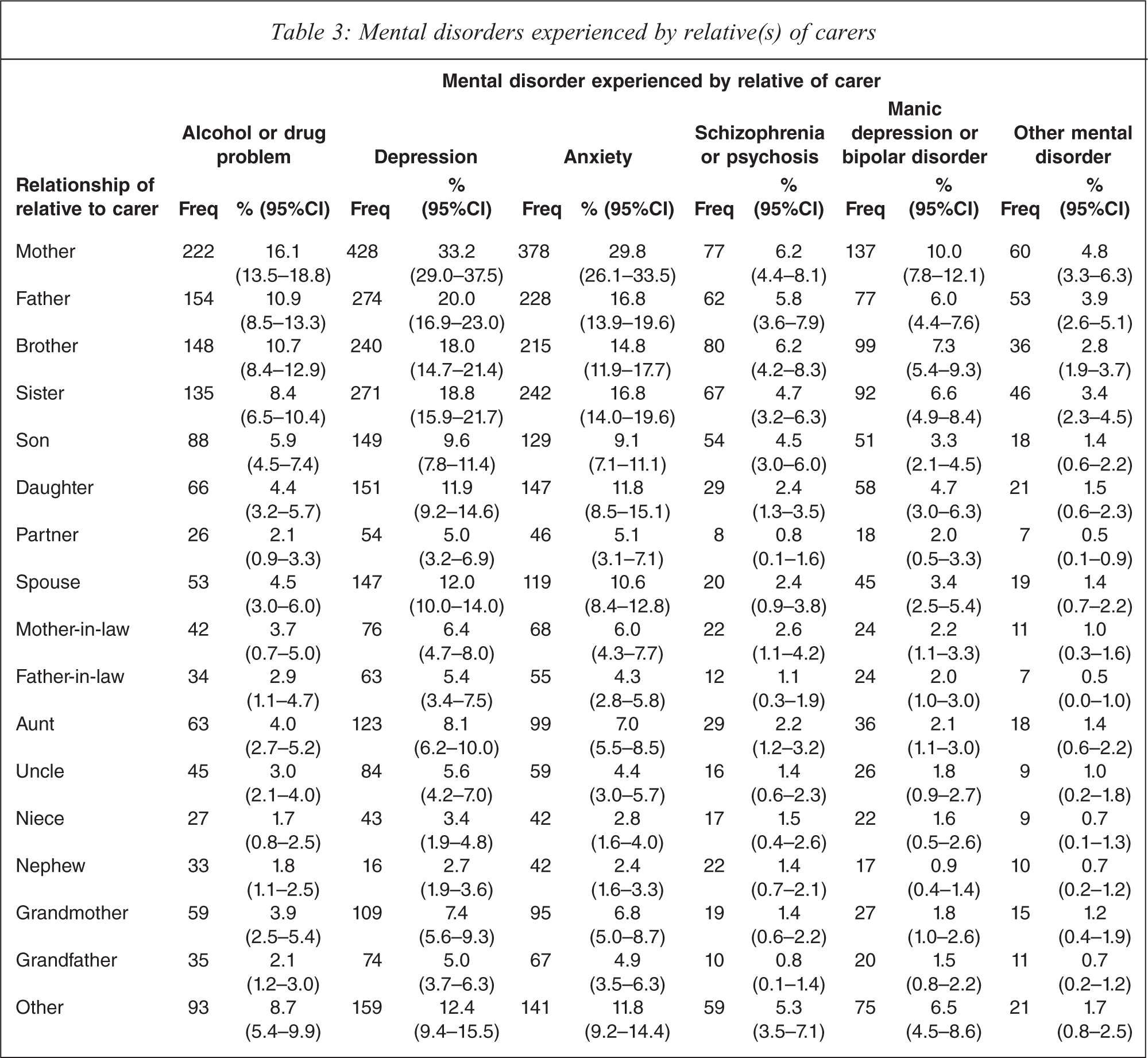
These caveats aside, Table 3 provides some indicative patterns. It suggests that the relatives of carers most commonly had depression, followed by anxiety and then by alcohol or drug problems. Not surprisingly, these relatives were closely related to the identified carers, usually being members of their nuclear family. Carers most commonly had mothers and fathers with mental disorders, particularly mothers. These were followed by brothers and sisters, and then sons and daughters. Spouses also featured relatively prominently among the relatives with mental disorders.
How do carers experience their care-giving role?
Carers were asked about the types of activities they performed in the course of caring for their relatives with mental disorders. Most commonly, carers indicated that their role involved keeping their relatives company or giving them emotional support (60.4%, 95%CI = 56%–64.8%). Many also spent time helping them with practical things like paper work, getting around, housework or taking medications (37.8%, 95%CI = 33.8%–41.8%). Much less common was the provision of help with things like washing, dressing or eating (11.7%, 95%CI = 9.1%–14.4%).
Carers were also asked about the degree of impact that the health problems of their relatives had on them. Feelings of embarrassment were uncommon, with 74.4% (95%CI = 71.2%–77.7%) experiencing no embarrassment, 13.1% (95%CI = 10.4%–15.9%) experiencing a little, 7.6% (95%CI = 6.1%–9.1%) experiencing some and 4.8% (95%CI = 3.4%–6.2%) experiencing none. Feelings of worry, anxiety or depression were far more common, with 23.6% (95%CI = 20.4%–26.8%) reporting a lot of these feelings, 36.4% (95%CI = 32.1%–40.6%) reporting some, 28.2% (95%CI = 24.4%–32%) reporting a little, and 11.8% (95%CI = 9.9%–13.8%) reporting none.
Carers were also asked whether the health problems of their relatives were associated with any financial cost to them, either in terms of money they spent or earnings they forfeited as part of their carer role. In total, 377 (29.4%, 95%CI = 25%–33.9%) indicated that caring for their relatives was associated with a financial cost. Of this 377 351 estimated the average monthly cost. The range was broad: for 15.5% (95%CI = 9.9%–21.1%) the average monthly cost was under $50, for 21.9% (95%CI = 16.4%–27.3%) it was between $50 and $149, for 19.8% (95%CI = 10.6%–29.1%) it was between $150 and $299, for 19.8% (95%CI = 13.6%–26.1%) it was between $300 and $999, and for 23% (95%CI = 14.1%–31.8%) it was over $999.
Discussion
The current study underscores the vital importance of carers in supporting people with mental disorders. Many people act as carers: 15% of the Australian adult population equates to nearly 2.4 million individuals. These carers provide a range of emotional and practical supports to close relatives with a range of mental disorders, most notably high prevalence disorders. People with mental disorders may be unable to access these sorts of supports from elsewhere, and they may make a crucial difference to their well-being, ability to cope and likelihood of recovery.
The 2007 NSMHWB had certain limitations which should be taken into account before interpreting the study's findings and considering their implications for policy and practice:
The response rate of 60% was sound but not optimal.
Certain selection biases may have affected the results (e.g., carers may have been under-represented because their care-giving role meant they were too busy to participate, or they may have been over-represented because their care-giving role gave them a particular interest in mental health issues).
The operational definition of carers was study- specific. On the one hand, it was somewhat restrictive, because it excluded those caring for a friend, those caring for a same-sex partner, child carers, non-English speaking carers, carers of people with disorders not considered by the survey because they were of low prevalence or difficult to assess (e.g. dementia), and people who were performing a caring role but did not view themselves as carers. On the other hand it was more inclusive than definitions that have been used in studies of broader groups of carers because it was based on the extent to which their relative's disorder affected their lives. By this definition, a carer's role may have extended to several people with a mental disorder, and a person with a mental disorder might have had a number of carers.
The survey relied on self-report and carers may have selectively remembered particular experiences and/or provided ‘socially desirable’ responses. They may also have incorrectly identified the disorder that their relative was experiencing.
Because the carer module constituted only one component of the survey it was necessarily fairly short. Had it been longer and more detailed, additional information about the carer experience might have been available, including information on potential benefits of care-giving.
The issue of attributing causality to associations identified through a cross-sectional survey cannot be ignored.
It is worth considering how the current findings compare with those from previous surveys. At 15%, the proportion of Australians caring for someone with a mental disorder is higher than the proportion of Australians caring for someone with a mental disorder and/or a physical disorder in other studies (e.g., 13% in SDAC). This discrepancy may be explained by the fact that our definition of a carer (of a person with a mental disorder) was more inclusive than that of SDAC, in that it was based on the degree to which the person's relative's mental disorder affected his or her life, rather than the activities that the care-giving role entailed. It should be noted that the care-giving activities were broader too: people who provided emotional support would not have qualified as carers in SDAC unless they also provided practical assistance of some sort, whereas emotional support was the most common activity associated with the care-giving role in the current study. We acknowledge that the definition of a carer used in SDAC is commonly accepted, but would argue that it is perhaps more relevant to carers of people with physical health problems. Emotional support is crucial for people with mental disorders; practical assistance is often less necessary because people with mental disorders are often capable contributors to the communities in which they live.
The study's findings offer some guidance as to the direction that policy efforts might usefully take if the Fourth National Mental Health Plan is to fulfil its promise of expanding the level and range of support for carers. Specifically, it points to some of the areas that may be associated with ‘carer burden’. Commentators use this term in various ways, often using it to refer to the emotional and psychological impact that care-giving has on carers [17]. The current study is informative in this regard. It suggests that care-giving is associated with a relatively high degree of emotional and psychological burden, in the sense that mental disorders and psychological stress were found to be linked to being a carer. Normally we would be cautious interpreting this association as a causal relationship because of the cross-sectional nature of the survey data, but the interpretation is strengthened in this case by the fact that three fifths of respondent carers indicated that their relatives’ disorders caused them at least some worry, anxiety or depression. It is also relevant that three quarters of respondent carers experienced no embarrassment about their relative's disorder, given that carers in the Mental Health Council of Australia's consultations indicated that they experienced a lack of respect by others of their caring role. This suggests that external factors, rather than internal ones, may often be key contributors to the emotional burden experienced by carers.
An alternative use of the term ‘carer burden’ refers to the financial cost of caring for individuals and for society [17]. The study provides support for the notion that there may be financial burdens associated with providing care to people with mental disorders. At an individual level, one third of respondents indicated that caring for their relatives was associated with direct or indirect costs. The magnitude of these costs varied, and it was not possible to determine the proportion of carers’ total income that was accounted for by these costs, but it is fair to say that for some carers these costs were considerable. At a societal level there were also suggestions that the economic costs associated with care-giving might be high: those in their prime years of productivity were particularly likely to be carers, and care-giving was associated with a moderate number of days out of role.
Together, these findings suggest that carers of relatives with mental disorders would benefit from strategies designed to alleviate some of the emotional pressures associated with care-giving, and that these strategies might have flow-on societal benefits. There would be merit in developing and evaluating a range of interventions designed to reduce the emotional and psychological burden carers experience, with a view to ‘rolling out’ successful interventions in mental health services across Australia. Such interventions would need to identify carers, consider the nature and extent of the impact of their relatives’ mental disorders, and assess their varying needs in an individualized manner. The Department of Health and Ageing has taken some steps in this regard, funding a project to develop good practice guidelines for identifying carers, and information packs to support carers in their role. There are international precedents to draw on with respect to the kinds of initiatives which might be promising as well. For example, Froggat et al. have recently produced a guidebook for working with families as partners in mental health which suggests a range of approaches to engaging carers and addressing their needs, and provides a number of case studies [18].
The study's findings also suggest that strategies designed to address the financial burden of caring for people with mental disorders would be helpful. The formal recognition given to carers in Australian health and social policies has grown over the past 30+ years, and Australia is regarded as well ahead of many other countries where support programmes are far less systematic. However, the existing carer allowance and carer payment may favour those caring for people with physical disorders, and not be sufficiently targeted towards carers of people with mental illness. This may be particularly the case for those who predominantly provide emotional support, rather than practical assistance. Such emotional support may consume considerable time and energy on the part of the carer, and may have an impact on their earning capacity.
The study also points to further research that would augment the current findings and help us to more fully understand the experiences of people caring for relatives with mental disorders. In particular, a purpose-designed longitudinal study of carers (and the people with mental disorders for whom they provide care) would be desirable. This could be modelled on the VCP [2], which was a landmark study in its time but is now somewhat dated, and which, as noted above, did not focus specifically on carers of people with a mental illness. Such a study should attempt to identify a larger and more inclusive cohort of carers, and should follow their experiences over time, gauging their responses across the course of their relative or friend's illness. The longitudinal design would permit a more detailed examination of associations between caring and the various socio-demographic and clinical factors identified here, and would help to clarify the causal direction of these associations. It would also allow the longer term impacts of caring to be examined. The larger scale would enable more detailed questions to be asked (e.g. Which carers experience the greatest emotional or financial burden? Is the profile of carers of people with mental disorders different from that of carers of people with physical disorders? Does the profile of carers vary with the type of mental disorder experienced by those for whom they are providing care? Are the experiences of carers associated with their coping styles and the level of support they receive?).
To conclude, the current study suggests that carers are significant stakeholders in the mental health system. Providing support for carers is crucial, particularly because their own mental health and well-being may be affected by their care-giving role. The nature of this support should take into account their large numbers, their profile and the role they perform. These conclusions echo those of previous studies, but are strengthened by the scale and representativeness of the current study.
Footnotes
Acknowledgements
The authors would like to thank the 2007 NSMHWB Reference Group for their input into the survey's design. The authors would also like to thank those who participated in the survey. The 2007 NSMHWB was funded by the Australian Government Department of Health and Ageing, and conducted by the Australian Bureau of Statistics.