
Abstract
Australian state governments have over the last decade pursued policies that have rapidly increased the number of people in prison. The escalation in incarceration has been particularly marked for women. In Victoria the daily average female prison population doubled from 123 in 1993–1994 [1] to 251 in 2003–2004 [2].
Compared to the general community, prisoners are reported to have higher rates of physical illness, educational disadvantage, social deprivation, and most particularly mental disorders [3–4]. The profiles of female prisoners have been reported to show even more dramatic levels of certain disorders than their male counterparts [5]. The mental health profile of women prisoners that emerges from the literature is of high rates of depressive disorders, anxiety disorders, drug and alcohol-related disorders, and personality disorder [3–11]. While the discrepancy may not be as marked, rates of a current1 psychotic disorder have been reported at between 1.6% and 10.9% [5, 3, 6, 12], placing them well above the rates in the general community.
Most women who are imprisoned serve only brief sentences lasting for weeks or months rather than years [13]. This time in prison presents a rare opportunity for many of these, often disadvantaged, women to receive mental health assessment and treatment. As noted by Davies and Cook [14], this opportunity is rarely taken and women are released to the community with their mental health issues not only untreated, but all too often exacerbated. If the culture of prisons is to change to one where sufficient quality mental health treatment is available to those who need it, then the actual rate of mental disorder in this population, relative to the general population, needs to be documented.
There have been several studies of rates of mental disorder among female prisoners in Australasia [7–11,15, 16]. These studies have been consistent with the international literature cited above in describing a populationwith high levels of depression, anxiety, personality disorder and substance-related disorder. However, there have been few studies to date in Australasia [7, 8, 15] that have compared rates of mental disorder among female prisoners with those for women in the community. Such comparison is essential to provide an index of the level of need for mental health services of women in prison relative to their community counterparts.
Method
The study involved a clinical interview and demographics questionnaire, administered to 103 female prisoners in Victoria's two women's prisons.
Ethics approval
Ethics approval was granted by all three Ethics committees approached. These were Monash University, the Victorian Department of Human Services and the Department of Justice. Two key ethical issues were given particular importance in the informed consent process of the procedure. These were the issues of voluntary participation and confidentially. Subjects were informed that their participation was voluntary and they would not receive payment for participation. Subjects were also advised that their responses were confidential unless there was an indication of risk to self or others, in which case the health team would be advised.
Design
A midnight census design was used where a list was drawn up of all of the women in prison on midnight at the start of the study. The aim was to interview as many of these women as possible thus providing a snapshot of the prison population at one point in time.
Exclusion criteria
There were three groups of women who were excluded from participation:
Those who did not understand sufficient English to complete the interview (n=5). This group was excluded due to insufficient resources for interpreter services. Those who were in management cells (for disciplinary reasons) at the time of the interview (n=7). This group was excluded as prison authorities denied us access to this group. Thosewho were transferred to hospital (n=5), and thosewho were released/transferred prior to interview (n=32) were not followed up, and therefore not interviewed.
Sample
A midnight census at H.M.P. Tarrengower on 22 March 2000, yielded 28 names, and at the Metropolitan Women's Correctional Centre (MWCC)2 on 28 June 2000 yielded 153 names. This resulted in a total population of 181 of whom 49 were excluded. Of the available population of 132, 103 women agreed to take part in the study.
The data from the prison sample are compared with data from the Australian Bureau of Statistics' (ABS) Australian National Mental Health Study [17–18]. This comparison group was chosen as it constitutes a large (n=10 660), representative sample of the Australian population. For the purposes of comparison with the prison sample, females were selected from the ABS database. The ABS raw data were made available for the study and the data for all females in the sample were entered directly into our database for statistical comparison with the female prison sample.
Interview process
Interviews were conducted by experienced forensic mental health professionals, seconded from Thomas Embling Hospital, who were given 3 full days training in the administration of the interviews by the principal author. Participants who provided consent were given a written and verbal explanation of the nature of the study, and of the limits of confidentiality. The interview contained, in addition to enquiries about demographic and family background, the Composite International Diagnostic Interview (CIDI) [18–19] and the PDQ-4+ [15, 20].
Instruments
Three major instruments were used in the present study:
The Demographics Questionnaire: This interview was based on the questionnaire developed by Mullen and Martin [21] and comprises questions about demographic details, experiences of abuse in childhood and adulthood, history of mental health treatment (both in prison and prior to imprisonment) and screener questions for grief and gambling issues. The Survey of Mental Health and Wellbeing (SMHWB) [17–18] is a version of the CIDI that was modified for the Australian National Mental Health Study, conducted by the ABS [17]. The computerised, 12-month prevalence version was used, assessing whether the subject met the diagnostic criteria for a mental disorder in the 12 months prior to the interview. The SMHWB provides DSM-IV and ICD-10 diagnoses. In the present study ICD-10 diagnoses were used for consistency with the ABS results. The personality disorder measure was a version of the Personality Disorder Questionnaire 4+ (PDQ-4+) [20], which was adapted for the national study of psychiatric morbidity in New Zealand prisons [15]. The PDQ-4+ was programmed in the same format as the computer-administered CIDI and provides DSM-IV diagnoses. This instrument is recommended as a screen for personality disorders [22].
Data analysis
Data analyses were conducted using SPSS (Version 9.0.1). Prevalence rates of disorder for the prison sample and community sample were compared using
Results
Interviews were completed with 103 female prisoners out of a possible 132, yielding a participation rate of 78%.
Demographic characteristics
The female prisoners had a mean age of 29.6 years (SD=8.6) and a median age of 27 years.
An Aboriginal backgroundwas indicated by 9.7%, compared to 0.5% of women in the Victorian community [23] (odds ratio=21.7; 95% CI=11.3–41.6; p<.001). When compared with women in the community, women in the prison sample were significantly less likely to have completed secondary school (odds ratio=0.2; 95% CI=0.09–0.26; p<.001), and were significantly more likely to have been unemployed prior to imprisonment (odds ratio=19.4; 95% CI=12.75–29.43; p<.001). In the prison sample 47% of the women interviewed had at least one dependent child.
Criminological characteristics
Seventy-four women were sentenced prisoners and 28 women were remandees. The median number of days spent in custody during the current period of imprisonment was 144.0 days (standard deviation= 569.1), with amedian of 122.0 days (standard deviation=771.7) still to serve. The mean number of previous periods of incarceration was 2.2 times (standard deviation=3.2).
Mental disorder
Table 1 presents the 12-month prevalence rates for the selected ICD-10 mental disorders for the female prison and community samples. Women in the prison sample had a significantly higher likelihood of meeting the criteria for a mental disorder in the past 12 months, compared to women in the community sample. This pattern held when the definition of mental disorder included drug and alcohol disorders, and also when the definition excluded substance use disorders. There were significant differences in the rates of personality disorder between the two samples, with female prisoners having a significantly higher likelihood of meeting diagnostic criteria. These differences were particularly marked for paranoid and borderline personality disorders.
12–Month prevalence rates of mental disorder among women in prison compared with community rates
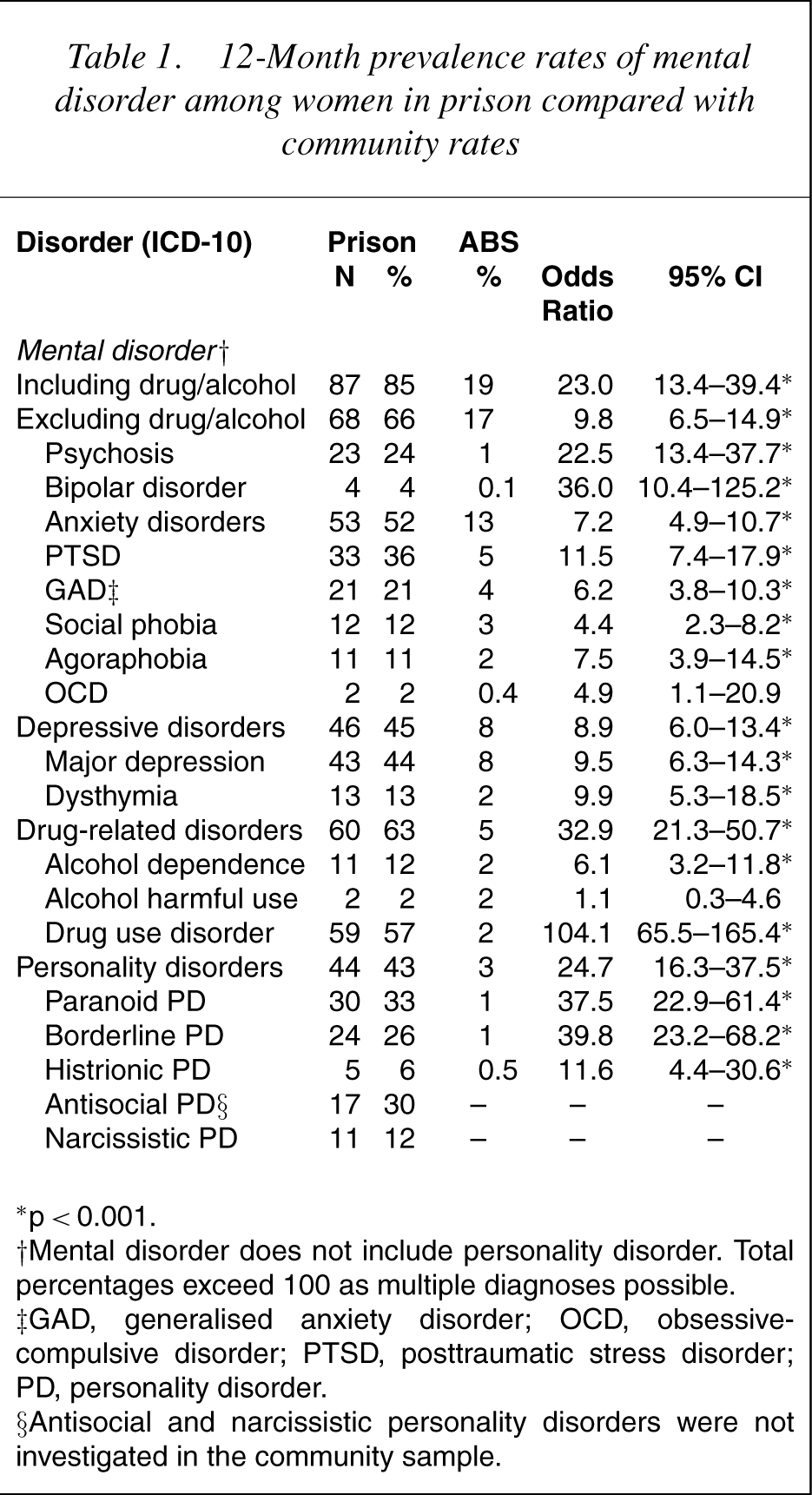
∗ p<0.001.
†Mental disorder does not include personality disorder. Total percentages exceed 100 as multiple diagnoses possible.
‡GAD, generalised anxiety disorder; OCD, obsessive–compulsive disorder; PTSD, posttraumatic stress disorder; PD, personality disorder.
§Antisocial and narcissistic personality disorders were not investigated in the community sample.
When individual mental disorders were considered, the rates were significantly elevated in the prison sample relative to the community sample, with the exceptions of obsessive-compulsive disorder and alcohol-related disorder. A relatively high percentage of women in prison (24%) were classified as a ‘case’ on the psychosis screener, compared to 1% of women in the community.
Co-morbidity in the female prison sample
A total of 41 women (63%) who met the criteria for a mental disorder in the last 12 months, also met the criteria for a drug-related disorder. A high percentage (71%) of female prisoners who met the criteria for a personality disorder also met the criteria for a drug-related disorder in the previous year.
Based on the high rates of psychosis reported in the female prison population, it was hypothesised that these high rates could be explained by the presence of co-morbid personality disorder or drug-related disorder. Table 2 presents co-morbidity rates for psychosis and drug-related disorder and psychosis and personality disorder among the female prison sample. As indicated in Table 2, a diagnosis of drug-related disorder did not significantly increase the probability of being identified as a case on the psychosis screen. Female prisoners with personality disorder were significantly more likely to have been identified as a case on the psychosis screen compared to those with no personality disorder. When individual personality disorders were considered, paranoid and antisocial personality disorder diagnoses were associated with an increased likelihood of psychosis screen ‘caseness’, while borderline histrionic and narcissistic personality disorder diagnoses were not.
Co-morbidity rates: psychosis by drug-related disorder and personality disorder
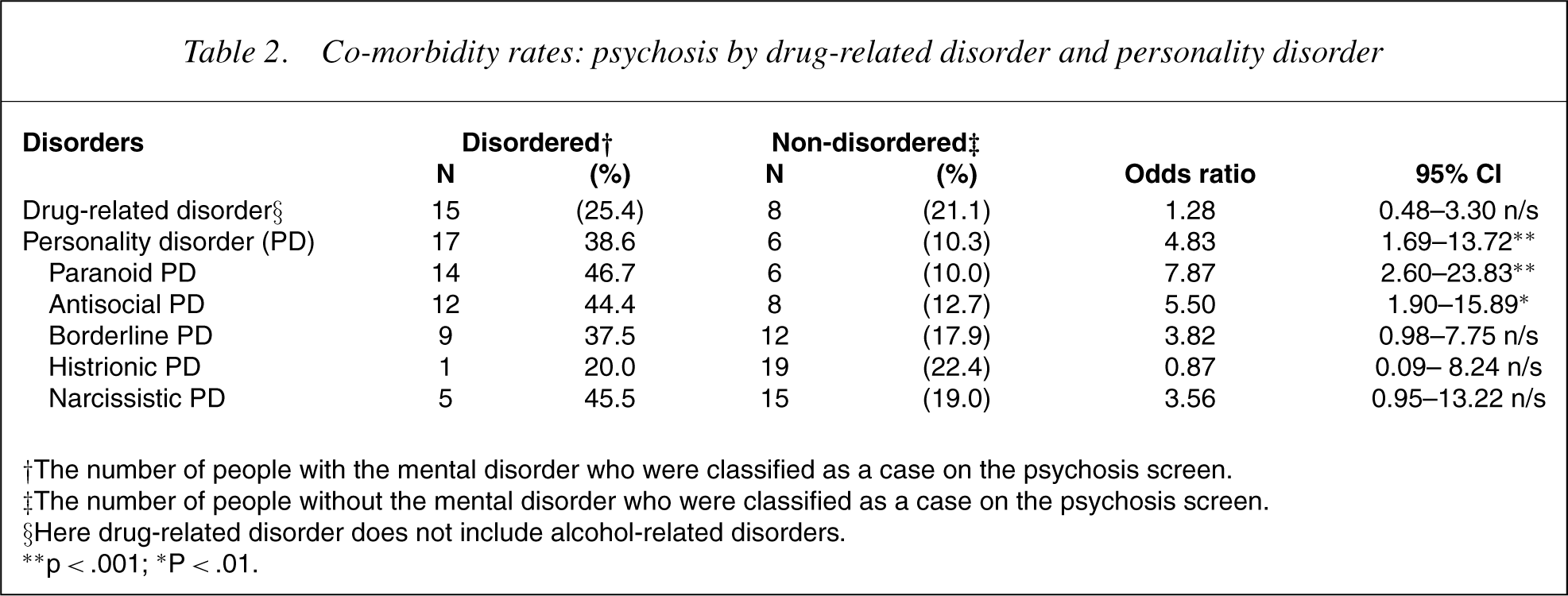
†The number of people with the mental disorder who were classified as a case on the psychosis screen.
‡The number of people without the mental disorder who were classified as a case on the psychosis screen.
§Here drug–related disorder does not include alcohol–related disorders.
∗∗ p<.001; ∗P<.01.
The impact of imprisonment on mental health
Analyses were conducted to determine whether factors such as number of previous periods of incarceration, legal status or number of days in custody (current period of imprisonment) impacted upon rates of mental disorder.
There were no significant differences in rates of mental disorder according to whether the current period of imprisonment was the subjects first period of imprisonment or not (odds ratio=0.79; 95% CI= 0.26–2.45). In addition, women on remand did not differ significantly from those serving a sentence in terms of rates of overall mental disorder (odds ratio=1.83; 95% CI=0.69–4.85). Finally, there were
Discussion
The present study represents the first Australian study to statistically compare rates of mental disorder among a female prison sample with a community sample using the same assessment instrument. It was found that women in prison had significantly higher rates of most mental disorders investigated when compared to a community sample. This is consistent with studies from the USA [3–4] that have considered this question. The greatest discrepancies between the two groups were found for drug-use disorder and paranoid and borderline personality disorders. The female prison sample interviewed represented a particularly disadvantaged group with high rates of unemployment, low education levels and overrepresentation of indigenous women, relative to the community sample. These factors may in part explain the elevated rates of mental disorder relative to the community sample. If subjects had been matched to controls based on demographic factors such as unemployment, years of education, age and ethnicity this may have allowed for a more meaningful comparison of the two groups.
Consideration of the pattern of disorder among the female prison population offers another hypothesis about the discrepancy between the prison and community samples. The most prevalent disorders in the female prison populationwere drug-use disorder, major depression, personality disorder and post-traumatic stress disorder. This constellation of mental disorders is markedly similar to that found in the literature on child abuse and the development of mental disorders in adulthood [21,24–25]. A hypothesis is that higher rates of abuse and neglect among the female prison population may contribute to higher rates of mental disorder relative to a community sample. This hypothesis will be the subject of a separate paper.
An unexpected finding was the high rates of positive responses to the psychosis screen. Most studies that have investigated the prevalence of psychotic disorder among women in prison have used a narrower definition, reporting only rates of schizophrenia [3, 8, 11]. This could partly explainwhy these studies found considerably lower rates of psychotic disorder compared to the present study. However, even studies with a broader focus have reported rates of ‘psychosis’ [5] and ‘schizophrenia and related disorders’ [6] at a lower prevalence than the present study. This discrepancy appears to be at least partly explained by the use of a psychosis screening measure in the present study. It would be expected that a screening measure would, by definition, identify more ‘cases’ than a comprehensive psychiatric interview. It is noteworthy that the psychosis screen did not identify particularly high rates of psychosis ‘caseness’ among women in the community sample [17].
Together this suggests that the psychosis screen tapped into experiences that are prevalent among the female prison population, but are not common among women in a community sample. The results were not explained by co-morbid drug-related disorder thereby largely ruling out the influence of substance intoxication/withdrawal. Rates of psychosis ‘caseness’ were higher among those with a paranoid or antisocial personality disorder, when compared to those without these personality disorders. The meaning and magnitude of this association is unclear; however, it is hypothesized that female prisoners with these personality disorders may be more vulnerable to developing a stress-related reactive psychosis in prison or upon release. These results represent a shift from the ‘schizophrenia’/‘not schizophrenia’ dichotomy, to a more complex model of psychosis among women in prison, where an individuals personality may increase their vulnerability to developing psychotic symptoms in the face of extreme stressors. Another hypothesis is that the high number of positive responses to the screen is a non-specific indicator of high levels of distress in this population.
In the present study it was found that neither legal status, number of previous imprisonments, nor the number of days spent in custody had a statistically significant impact upon rates of mental disorder. It was particularly surprising that women on remand did not have a greater likelihood of having a current mental disorder than sentenced women, given that past research has found greater levels of disturbance among women on remand due to the associated uncertainty and stress [10].
There are several methodological issues that may have influenced the results of this study. First, for various reasons, three important groups of female prisoners were not interviewed. Women in management cells may have had high levels of emotional disturbance due to long hours of solitary confinement in a low-stimulus environment and related to behavioural problems that may have led to their management status. Women who were not fluent in English may have had distinct mental health issues, perhaps related to their immigration to Australia and associated stressors. Those individuals transferred to Thomas Embling Hospital by definition had serious mental health issues. In summary, it is hypothesized that the results of the present study are an under-representation of actual rates.
Second, at the time of data collection, the Metropolitan Women's Correctional Centre was in a state of disorganization and flux and was taken back into government control shortly before the end of data collection. It is likely that the palpable sense of unease in the prison at that time influenced the women imprisoned there and contributed to the rates of mental disorder to at least some extent.
Third, it is important to highlight the issues in conducting research with women in prison. As noted by Grimwade [26] in the academic literature on female prisoners, these issues tend to be minimised or ignored in the discussion and methodology, leaving prospective researchers ill-equipped to do the work that needs to be done. Women in prison are used to taking part in research that serves someone else's purpose but does not change anything for female prisoners. This, combined with the fact that many women in prison have been taken advantage of and let down throughout their lives, means that the usual process of recruiting participants (advertise, get names, start) does not apply in prison. In the present study we tried that and we recruited two participants.
Gaining participants was a lengthy and difficult process of building the women's trust in the researcher and the study itself. This involved being seen around the prison for several months and gaining the support ofwellrespected and trusted female prisoners by explaining the study in detail and taking the time to answer their questions honestly. A common (and reasonable) question was ‘what's in it for you?’ Two staff at the education centre, who have worked in the area for many years supported the study, which led to many women agreeing to take part as they trusted these individuals implicitly. For those who want to conduct research in this area, it is necessary to put aside the ‘experts hat’ and to be humble, honest and flexible.
In conclusion, this study suggests that women imprisoned in Victoria come to prison with high levels of multiple mental disorders relative to the general community. It does not appear that their mental health issues can be solely attributed to the stress of imprisonment; however, it is likely that their pre-existing disorders are exacerbated within the prison environment. For many women, their prison sentence offers an opportunity to receive psychiatric and clinical psychological assessment and treatment that they may not have access to outside prison. Sadly, due to lack of resources, this opportunity is often missed. Recent studies have addressed the area of screening and assessing mental disorder among the female prison population [6, 27]. Now the challenge remains: for governments, policy-makers and prison operators to provide the therapeutic services needed to address the welldocumented needs of female prisoners.
Footnotes
1Definitions of ‘current’ mental disorder in the literature vary from one month to 12 month prevalence rates.
2Note: The Metropolitan Womens Correctional Centre (MWCC) was renamed Dame Phyllis Frost Centre shortly before the conclusion of data collection.