
Abstract
The majority of the psychological research on combat and operational trauma has focused on consequences directly experienced by combat veterans themselves, such as depression, anxiety and post-traumatic stress disorder (PTSD) [1–5]. Only recently has research considered the stressors and mental health outcomes experienced by partners and carers of veterans [6,7]. The current study extends this research by introducing a new scale to assess distress experienced by partners of veterans with operational service.
Combat trauma has a clear potential for negative outcomes in dyadic relationships [8–15]. Combat veterans often face the challenge of returning home as changed individuals trying to adapt to family situations that are quite different from when they initially departed [1]. Thus, not only do veterans’ families have to adjust to the possible changes in the veteran, the veteran also must adjust to changes in the family that may have occurred in his or her absence.
Manguno-Mire and colleagues [16] found that partners of veterans diagnosed with PTSD are often highly distressed and receive limited support for their mental health issues. Lack of recognition of the unique stresses experienced by partners, and the absence of effective interventions, can result in a negative feedback loop in which the physical and psychological problems experienced by veterans produce a stressful family environment which, in turn, further undermines the veteran's physical and mental health [17]. Several studies suggest that stress of war on soldiers’ marriages/dyadic relationships may increase the probability of suicide amongst veterans [18–20].
Guest and colleagues refer to any persistent psychological difficulty resulting from operational duties as operational stress injury [21]. This term incorporates diagnosed conditions such as PTSD, anxiety, and depression, as well as a range of less severe conditions. This terminology, and the range of functioning it encompasses, captures those who present with sub-clinical symptoms that do not qualify for a specific diagnosis. To date, much of the research on carer distress has focused on partners of veterans with PTSD. Although partners of PTSD-diagnosed veterans are clearly a population at risk, it is important to recognize that returning veterans unaffected by PTSD may also experience non-trivial adjustment problems and reduced psychosocial functioning, often creating significant challenges for carers and other family members [22]. Given the mutually supportive functions of intimate dyadic relationships, it follows that the psychological health of combat veterans are likely to have a direct impact on the outcomes for their partner, carer, and other members of their family. Similarly, as noted earlier, partner and carer distress can impact on the psychological health and functioning of veterans, creating a potentially destructive feedback loop within households.
A wide variety of scales have been used to assess the nature, degree, and type of distress, as well as the psychosocial and physiological consequences associated with caring for veterans [23]. However, there is currently no scale that exclusively measures the unique stressors that are common to partners of veterans, nor the degree of distress that each of these stressors may cause. Furthermore, other existing measures of caregiver distress were developed for use with other populations, such as familial carers of people with dementia, cancer, and acquired brain injury [24]. These existing measures cannot be assumed to be applicable to partners of combat veterans, given that the underlying factors causing distress may differ substantially for this latter group. The primary aim of this study was to address these gaps by developing and evaluating a new multidimensional measure to assess the specific sources of distress experienced by partners of military veterans with operational service.
Method
Participants
Participants were 665 female NSW members of the Partners of Veterans Association of Australia (PVA), representing a 57.82% response rate of those 1150 questionnaires initially distributed. Membership in this association is open to any person whose current or former partner served in a theatre of war or campaign, or is currently serving in any peacekeeping/peacemaking duties or any other military operational service. Ages ranged from 33–90 years (M = 57.79, SD = 6.46). The vast majority of respondents, 93%, were married at the time of completing the questionnaire, with the remaining 7% being widowed, divorced or separated. For those currently married, the average length of marriage was 31.5 years (SD =10.74, range =1–62 years). Most respondents (84%) were ‘official’ carers for their veteran partner (i.e. they received a government allowance as payment for their caring role), and 72% belonged to carer-related support groups. Eighty-four per cent of respondents had partners who served in the Army, 8% from the Air Force and 8% from the Navy. Over half (55%) were partners of long-term service personnel, with 45% being partners of National Conscripts. The majority of the veterans served in Vietnam (83%). Others served in the Malayan Confrontation (5%), World War II, the Korean War and POW (3.5%), Sinai and Somalia (2.5%), and remaining 6% served in East Timor, Gulf War I or current Middle-East operations (Afghanistan and Iraq).
Measures
Partners of Veterans Distress Scale
An initial item set was generated from focus groups of partners of Australian veterans with operational service [25], in which respondents discussed common stressors and problems that resulted from caring for, and living with, combat veterans. This resulted in the generation of 72 items that covered 12 themes: financial difficulties, social problems with family, social problems with friends, difficulty in coping with veterans’ changes in mood and behaviour, worrying about the future, problems associated with their children, despair at the lack of support from outside the veteran community, emotional and psychological problems, lack of intimacy, sense of isolation, feeling overwhelmed, and physical health problems.
Two registered psychologists, who worked exclusively with veterans and their families, reviewed the initial item pool and provided comments on the wording, relevance, and comprehensiveness of the items. Based on the feedback from these two expert reviewers, five items were re-worded and no items were added or eliminated from the initial pool.
Participants were asked if each potential stressor applied to them; (yes/no) and, if so, how much personal distress it causes. Degree of distress was assessed using a five-point Likert-type response scale of 0 (does not cause me distress), 1 (mild distress), 2 (moderate distress), 3 (severe distress), and 4 (extremely severe distress). Respondents who indicated that a stressor did not apply to them were also assigned a distress score of 0 for that item. Feedback indicated that many participants found the meaning of one item to be difficult to interpret. Therefore, this item was removed from all subsequent analyses.
Validation measures
Concurrent validity data were obtained from the administration of three self-report questionnaires with established reliability and validity. The RAND 36-Item Health Survey 1.0 [26] is a measure of general health status. In the present study, the two summary scores of the Physical Component Summary (PCS) and Mental Component Summary (MCS) were utilized [26]. Ware [27] found Cronbach's α for the PCS and MCS 0.84 and 0.88 respectively. The corresponding values for the current study were 0.85 and 0.82. The Satisfaction with Life Scale (SWLS) is a 5-item scale that assesses the cognitive–judgemental component of subjective well-being known as global life satisfaction [28]. Cronbach's α for the SWLS is reported as 0.87 [29]. For the current study, α was 0.9.
Procedure
This study received approval from the University of New England's Human Research Ethics Committee. The questionnaires, with reply paid envelopes, were distributed to female partners of veterans via the PVA newsletter. The questionnaire took approximately 20 min to complete. Seventy-six respondents completed the questionnaire package twice to assess test-retest reliability for the Partners of Veterans Distress Scale (POV-DS). The retest questionnaires were completed two to four weeks after the initial responses.
Results
Exploratory factor analysis
The 71 items from the POV-DS were subjected to principal-axis factoring using 300 randomly selected participants from the total sample. To determine the number of factors to retain, we applied Cattell's scree test [30], Kaiser's Eigenvalues greater-than-one rule [31], and Horn's parallel analysis [32] to the unrotated solution. Kaiser's rule [31] indicated that 11 factors should be retained, whereas the scree test suggested four and the parallel analysis suggested eight. Solutions between 4 and 11 factors were subjected to Promax rotations (kappa = 4) and assessed for interpretability. A seven-factor solution was deemed to be most interpretable. This solution explained 65.36% of the variance in the original item set.
The factors were named Sleep problems, Hyper-vigilance, Social isolation, Financial stress, Intimacy problems, Exhaustion, and Negative affect. Of the original 71 items, 45 items with pattern matrix loadings greater than 0.5 and no cross-loadings greater than 0.3 were retained for a subsequent confirmatory factor analysis, and to compute subscale scores. Table 1 provides the factor loadings for retained items. A complete set of POV-DS items can be obtained by contacting the corresponding author.
Promax (kappa = 4) rotated factor loadings for the POV-DS items
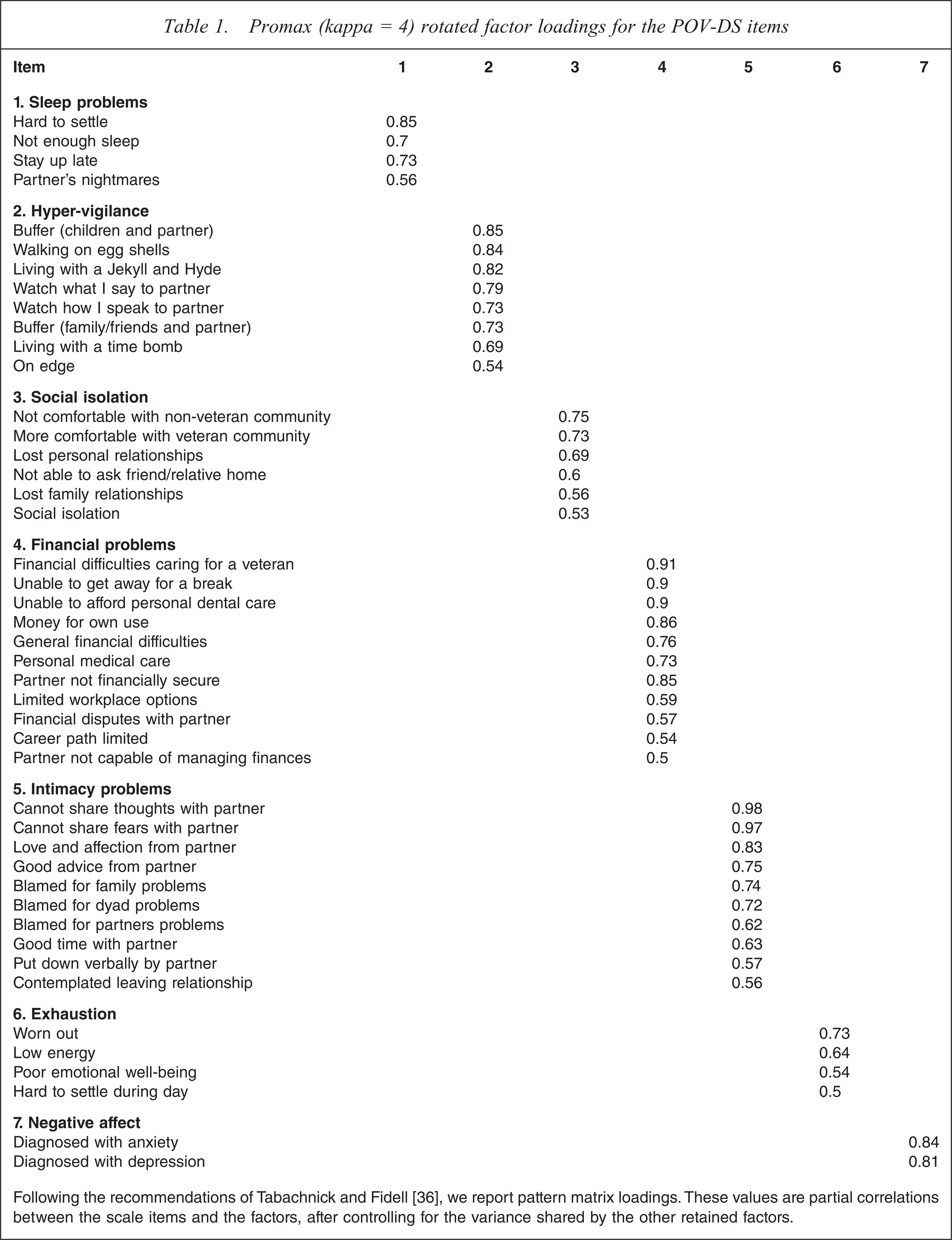
Following the recommendations of Tabachnick and Fidell [36], we report pattern matrix loadings. These values are partial correlations between the scale items and the factors, after controlling for the variance shared by the other retained factors.
Confirmatory factor analysis
Confirmatory factor analysis (CFA), using MPlus [33] on a hold-out sample of 365 participants, was conducted on 45 items retained from the initial exploratory factor analysis (EFA). Initially two models were assessed, a single factor model and a seven-factor model based on the solution from the EFA. Fit indices for the two models are presented in Table 2. Although the seven-factor model fitted the data significantly better than the single factor model, χ2differnece(21) = 3014.66, p < 0.001, overall fit was inadequate with normed chi-squared (χ2/df), root-mean-square error of approximation (RMSEA), and comparative fit index (CFI) values all falling outside the standard criteria for acceptable fit recommended by Kline [34] (see note at the bottom of Table 2 for a description of these criteria). Examination of modification indices revealed that fit could be substantially improved by correlating the errors of nine pairs of very similarly worded items (e.g., ‘walking on egg shells’ and ‘living with a Jekyll and Hyde’, ‘more comfortable with veteran community’ and ‘not comfortable with non-veteran community’, and ‘career path limited’ and ‘workplace options limited’). In all cases, items with correlated errors loaded on the same latent variable (factor). Furthermore, none of the modification indices suggested that any of the POV-DS items should cross load on multiple factors. The revised model with correlated errors fitted the data significantly better than the original seven-factor model, χ2differnece(9)= 1586.56, p < 0.001, and also met or exceeded the criteria for good fit recommended by Kline [34].
Goodness-of-fit indices for the confirmatory factor analyses
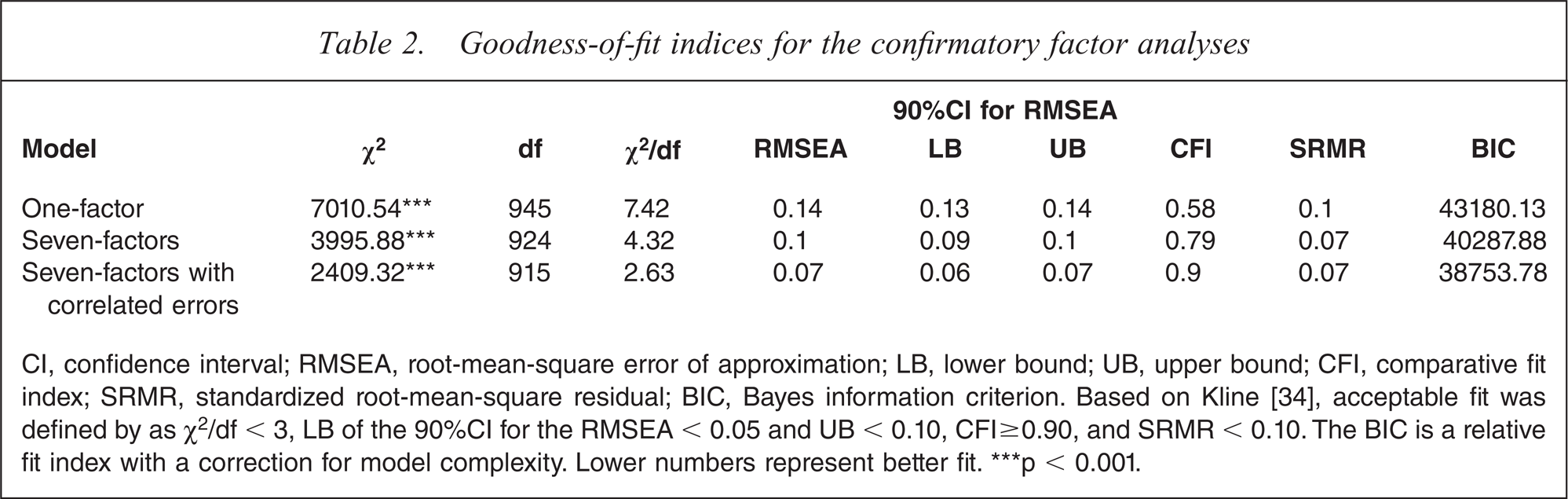
CI, confidence interval; RMSEA, root-mean-square error of approximation; LB, lower bound; UB, upper bound; CFI, comparative fit index; SRMR, standardized root-mean-square residual; BIC, Bayes information criterion. Based on Kline [34], acceptable fit was defined by as χ2/df < 3, LB of the 90%CI for the RMSEA < 0.05 and UB < 0.10, CFI ≥ 0.90, and SRMR < 0.10. The BIC is a relative fit index with a correction for model complexity. Lower numbers represent better fit. ∗∗∗p < 0.001.
Scale construction
Using the entire sample, we computed POV-DS subscale scores for the derived seven factors by averaging the scores on items that loaded on each factor. Table 3 presents descriptive statistics, intercorrelations, internal consistencies, and test-retest reliabilities. The POV-DS exhibited excellent internal consistency (Cronbach's α for the subscales ranged between 0.85–0.95) and good to excellent test-retest reliability (range = 0.62–0.82).
Means, staxndard deviations, intercorrelations, Cronbach's a, and test-retest reliabilities for the seven POV-DS subscales
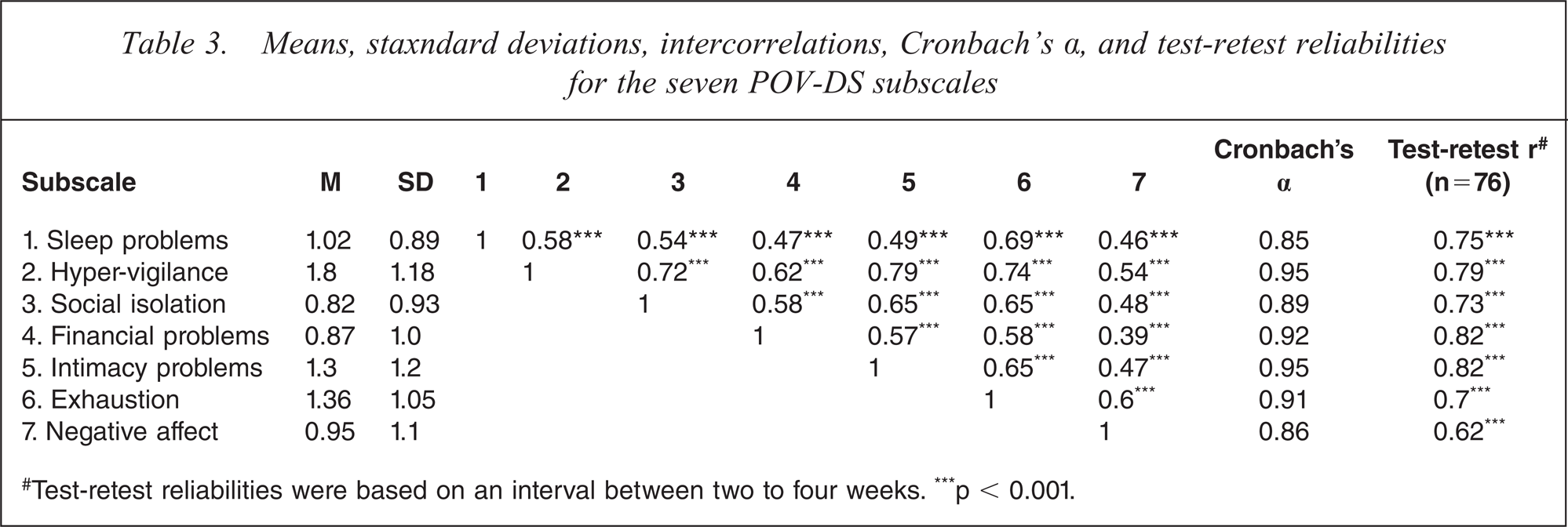
#Test-retest reliabilities were based on an interval between two to four weeks. ∗∗∗p < 0.001.
Concurrent validity of the POV-DS
Descriptive statistics for the validation measures
A one-sample t-test was conducted to compare the physical health (PCS) scores for the current sample with a normative sample from the Medical Outcomes Study (MOS) [28]. Partners of veterans in the current sample produced significantly lower PCS scores (M = 210.18, SD = 98.26) than the normative sample (M = 251.34; t (659) = −10.76, p < 0.001). A similar pattern was evident for Mental Health (MCS) scores, with respondents in the present study scoring significantly lower (M = 194.12, SD = 92.63) than members of the MOS sample (M =267.08; t (659) = −20.24, p < 0.001).
In terms of satisfaction with life, 25% of partners in the current sample indicated they were extremely dissatisfied with life, 27% were dissatisfied, 18% were slightly dissatisfied, 3% were neutral, 13% were slightly satisfied, 10% were satisfied, and 4% were extremely satisfied. Comparative mean norms for an equivalent population were not available for this measure.
Regression analyses
Three regression analyses were conducted to assess the concurrent criterion validity of the POV-DS, in which the seven distress subscales were used to predict physical health (PCS), mental health (MCS), and satisfaction with life. A summary of these analyses is presented in Table 4. The POV-DS subscales explained 31% of the variance in physical health, 45% in mental health, and 43% in life satisfaction. In terms of contributions of individual subscales, Exhaustion (3%), Sleep problems (2%) and Hyper-vigilance (1%) all explained significant unique variance in physical health. Exhaustion (3%) and Negative affect (1%) explained unique variance in mental health. Relationship problems (3%), Exhaustion (2%), and Hyper-vigilance (1%) significantly predicted life satisfaction. As expected, higher distress scores were associated with lower levels of physical health, mental health, and satisfaction with life.
Summary of Multiple Regressions using POV-DS Subscales to Predict Physical Health, Mental Health, and Satisfaction with Life
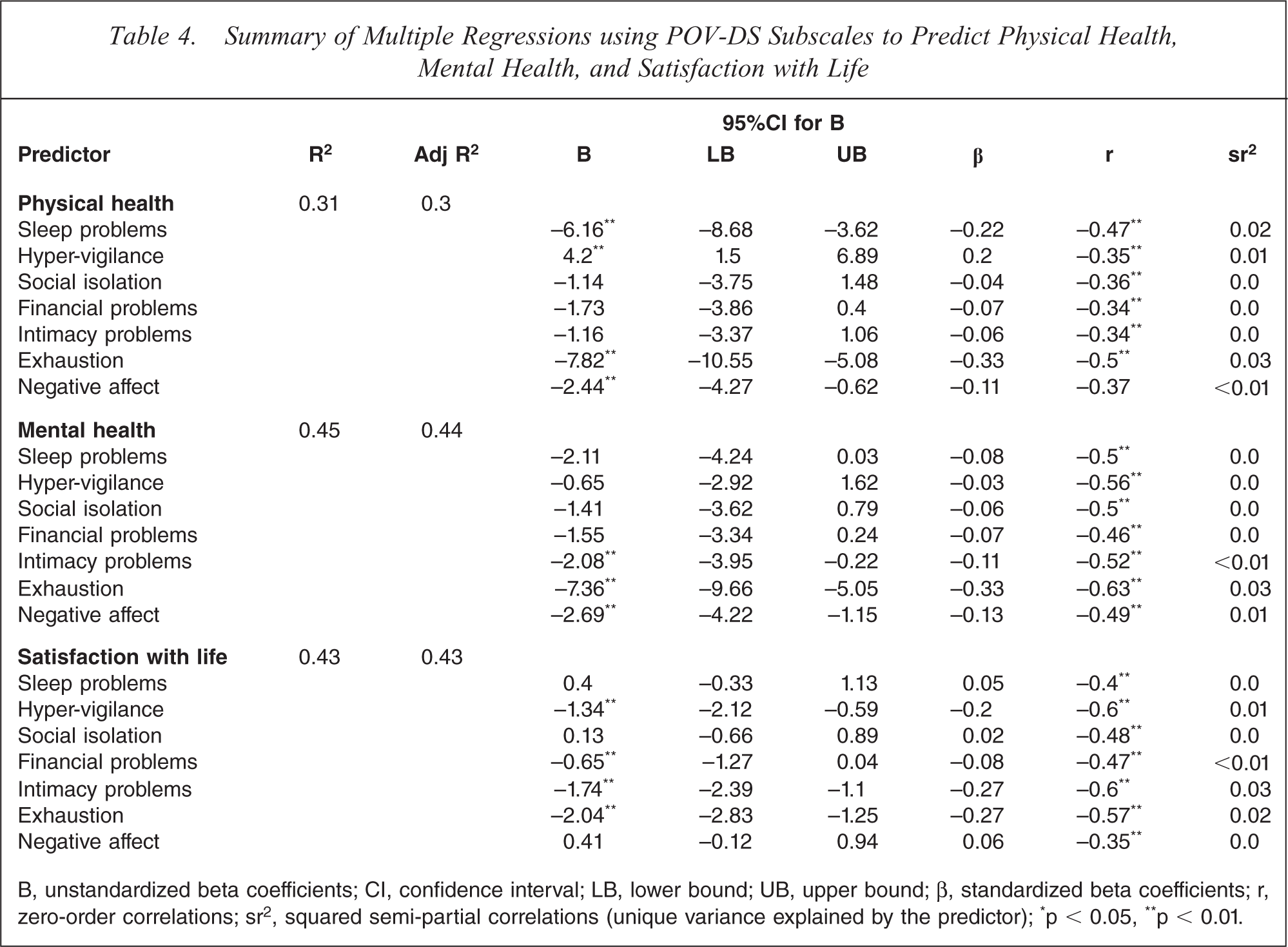
B, unstandardized beta coefficients; CI, confidence interval; LB, lower bound; UB, upper bound; β, standardized beta coefficients; r, zero-order correlations; sr2, squared semi-partial correlations (unique variance explained by the predictor); ∗p < 0.05, ∗∗p < 0.01.
Discussion
The purpose of the present study was to develop and evaluate a measure of distress experienced by partners of Australian combat veterans. Although several studies have established that caring for a veteran can have adverse effects on partners [9,23], the precise nature of these effects has not been investigated in detail. The item pool for the measure was derived from focus groups with members of the population of interest, coupled with expert evaluation of individual items. EFA revealed that the POV-DS assessed seven distinct domains of partner distress: Sleep problems, Hyper-vigilance, Social isolation, Financial problems, Intimacy problems, Exhaustion, and Negative affect. Further support for the seven-factor model was provided by a CFA on a hold-out sample. Cronbach's αs for the individual subscales ranged from 0.85 to 0.95, reflecting excellent internal consistency. Test-retest correlations, ranging from 0.62 to 0.82, suggested sound temporal stability.
Evidence for concurrent validity of the POV-DS subscales also was encouraging. The correlations between the subscales and three validation measures were all statistically significant and in the expected direction. That is, the higher scores on the seven partner distress dimensions were significantly associated with poor physical and mental health, and lower satisfaction with life. Taken as a group, the subscales explained substantial amounts of variance (≥ 30%) in physical health, mental health and satisfaction with life. Distress related to exhaustion appeared to be a particularly important predictor, explaining unique variance in physical health, mental health and satisfaction with life. This result could be explained by the arduous task of continually interpreting the needs of their veteran and in many cases feeling fully responsible for all family matters [9,23,35,36].
There are several limitations that should be taken into account when interpreting the findings from the present study. First, this study used a correlational design, thus causal relationships between partner distress and physical and mental health outcomes should not be assumed. Further longitudinal research using the POV-DS is needed to more adequately examine such relationships. A second limitation is that our sample is not representative of the whole age range of partners of Australian combat veterans. Future research should examine the validity of the POV-DS with younger partners, given that only 9% of the participants were under the age of 50 in the current study, as well as with partners of current serving members of Australian defence services.
In conclusion, the POV-DS is a new multidimensional measure of distress experienced by the partners of combat veterans. The measure has excellent psychometric properties, and we believe that it will be a useful tool for researchers and practitioners interested in examining factors underlying distress of partners and/or caregivers of combat veterans. By identifying key sources of distress, it may also prove useful in developing targeted interventions to increase the quality of life in specific areas of both veterans and their partners.
Footnotes
Acknowledgements
The authors wish to thank the Partners of Veterans Association of Australia Inc. for their assistance with recruitment. This paper is based on research conducted for a Doctor of Philosophy (Psychology) thesis by the first author. Thanks to Robert who hung in there.