
Abstract
Body dysmorphic disorder (BDD) is characterized by severe dissatisfaction with one's appearance, which involves a preoccupation with ‘imagined’ or minor bodily defects. Clinically, it results in significant distress and impairment in many aspects of everyday functioning, including quality of life and neurocognition [1,2]. There is an estimated 1.7% prevalence of BDD in the general population [3], indicating that it is not uncommon. It is equally evident in both genders and has an age of onset ranging from 14–20 years [3].
The aetiology of BDD is not yet known, but a range of distinctive cognitive styles have been reported. These include excessive self-focused attention [4], low levels of self-esteem [5,6,7], high levels of social anxiety [8,9], atypical internal aesthetic standards due to a strong discrepancy between actual self and ideal self [9] and poor levels of insight and ideas of reference [10]. In addition, patients with BDD hold strong ‘abnormal’ beliefs about their physical ‘impairment’, which varies in terms of delusional conviction. For example, Phillips and colleagues [10] found that 50% of the BDD individuals in their sample had beliefs that could be classified as delusional. Thus, two potential variants of the disorder have been identified: delusional and non-delusional BDD [10,11,12]. It has been argued that the two variants constitute the same disorder as they have many more similarities (i.e. demographics, symptoms, comorbidity and treatment response) than differences and that the delusional type simply reflects greater severity and less insight [10,11,13]. These findings suggest that delusional thinking varies on a continuum rather than being categorical [14], although no empirical data have been collected to support this proposition.
The DSM-IV currently classifies BDD under somatoform disorders. If delusions are present an extra diagnosis as delusional disorder, somatic type (DDST) [15] is given. This classification of BDD has been recently been disputed. Fontenelle et al. [16] highlighted the difficulty involved in the classification of BDD, with arguments for and against the diagnostic limitations of the subtypes. Those authors concluded that there is insufficient evidence to draw any definitive conclusion regarding the nosological status of ‘delusional’ BDD/DDST. The delusions held in BDD individuals are not bizarre, but rather generally accepted, albeit exaggerated, thoughts about their physical appearance. However, the high levels of conviction held about the particular body part(s) result in extreme distress and preoccupation [17]. The level of conviction with which these beliefs are held, as well as the degree of preoccupation and amount of distress, vary over time and across individuals, but can have significant adverse effects on a person's life and emotional well-being [18]. It is therefore of importance to elucidate the underlying etiology and pathophysiology of delusional thinking in BDD, to facilitate accurate diagnostic classification.
The current study aimed to further our understanding of delusional thinking and cognitive styles in BDD. At present there is no established measure of delusional thinking specifically for BDD. We employed the Peters’ Delusional Inventory (PDI) [18], a measure of delusional ideation which incorporates the dimensions of belief strength, preoccupation and distress. The PDI was not designed to identify fully blown clinical psychotic delusions, but rather to examine unusual beliefs in delusion prone populations. We believe this questionnaire is therefore ideal for the present study. First, the questionnaire assesses the type of delusional belief most commonly expressed by people with BDD (i.e. beliefs that are more consistent with cultural norms than psychotic delusions). Second, the PDI obtains levels of conviction, preoccupation and distress, characteristics that may be able to differentiate whether or not the degree of delusional thinking varies on a continuum or falls into two separate delusional and non-delusional variants. This study predicted that the current BDD sample would show levels of delusional thinking that vary on a continuum. Further, it was hypothesized that the BDD sample would be more impaired than healthy controls on measures of cognitive style [10,11], including creative experiences, self-esteem, self-ambivalence and depressive ideation. Within the BDD sample, it was hypothesized that correlational analyses would show that impaired cognitive styles are associated with greater delusional thinking, greater illness severity and lower levels of insight.
Method
Participants
Subjects were 14 patients with BDD diagnosed according to DSM-IV-TR criteria, recruited from a local BDD clinic in Melbourne, Australia. Exclusion criteria for the BDD patients included current or previous major medical and/or neurological disorders, head injury and current or previous alcohol and/or substance abuse. BDD patients with comorbid Axis I disorders were not excluded if the primary diagnosis was BDD, as BDD shows very high rates of psychiatric comorbidity. Diagnosis was confirmed using the Body Dysmorphic Disorder Diagnostic Module (BDD-DM) [19]. Severity was rated using the clinician-rated Yale-Brown Obsessive-Compulsive Scale modified for BDD (BDD-YBOCS) [17,20]. The current BDD group of patients were classified as having moderate to severe BDD (average BDD-YBOCS score = 25, range = 5–37). The level of insight in the BDD group was ascertained from scores given on three questions from the BDD-YBOCS. The scores ranged from 0–4 (0 = excellent insight, 1 = good insight, 2 = fair insight, 3 = poor insight, 4 = lacks insight, delusional). The current BDD group had a mean insight level score of 2 (range of 0–4), suggesting a ‘fair insight’ level and that the BDD patients reluctantly admitted that thoughts seemed unreasonable but wavered. At the time of clinical presentation, the current BDD group had, on average, two body-specific concerns (range of 1–5). The most common types of body-specific concerns involved the face and skin; however other types of body concerns were also evident, see Table 1.
Body parts of concern for the BDD patients
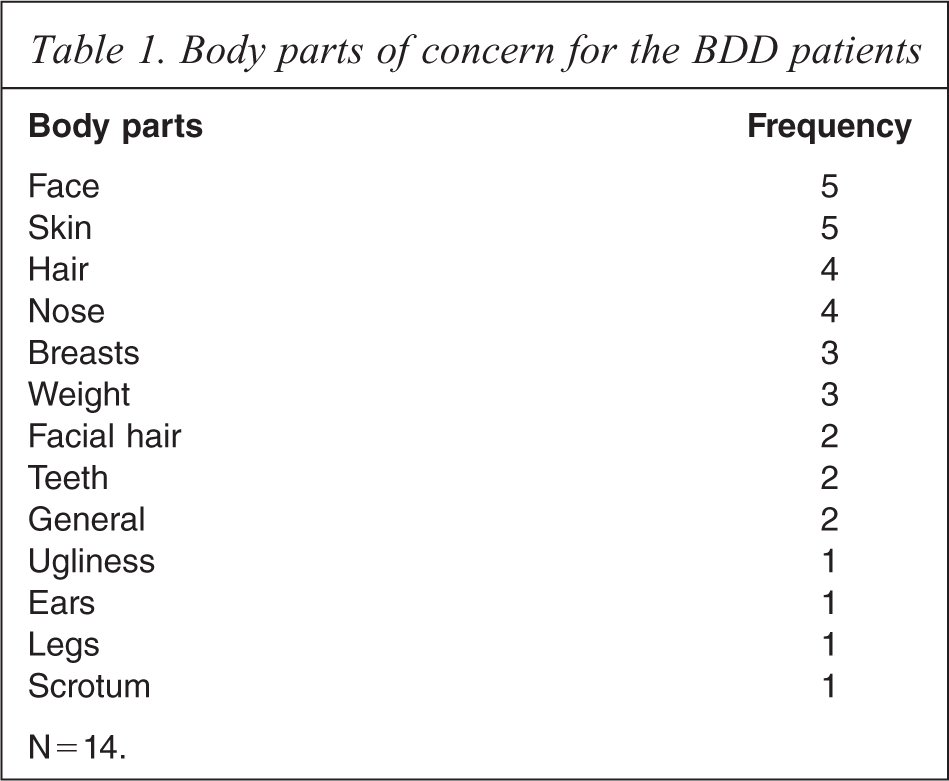
N = 14.
A comparison group of 14 healthy controls, matched on gender, age and education, were recruited via newspaper advertisements and posters at local universities. The same exclusion criteria used for BDD patients were applied. In addition, healthy controls had no history of an Axis 1 diagnosis as assessed by the control screen of the Structured Clinical Interview for DSM Disorders (SCID) [21]. All participants were between the ages of 18 and 55 years and had an estimated pre-morbid IQ of >70 as scored by the National Adult Reading Test (NART) [22], to ensure no-one was intellectually disabled and could understand task instructions. Depression and anxiety were measured in both groups using the Beck Depression Inventory (BDI-II) [23] and the Beck Anxiety Inventory (BAI) [24]. They are both 21-item self-report measures, which were administered to investigate the intensity of depression and anxiety, respectively. A total score on each measure was calculated separately for analysis. Demographic and clinical information of the participant groups is presented in Table 2.
Demographic and clinical information for the two participant groups
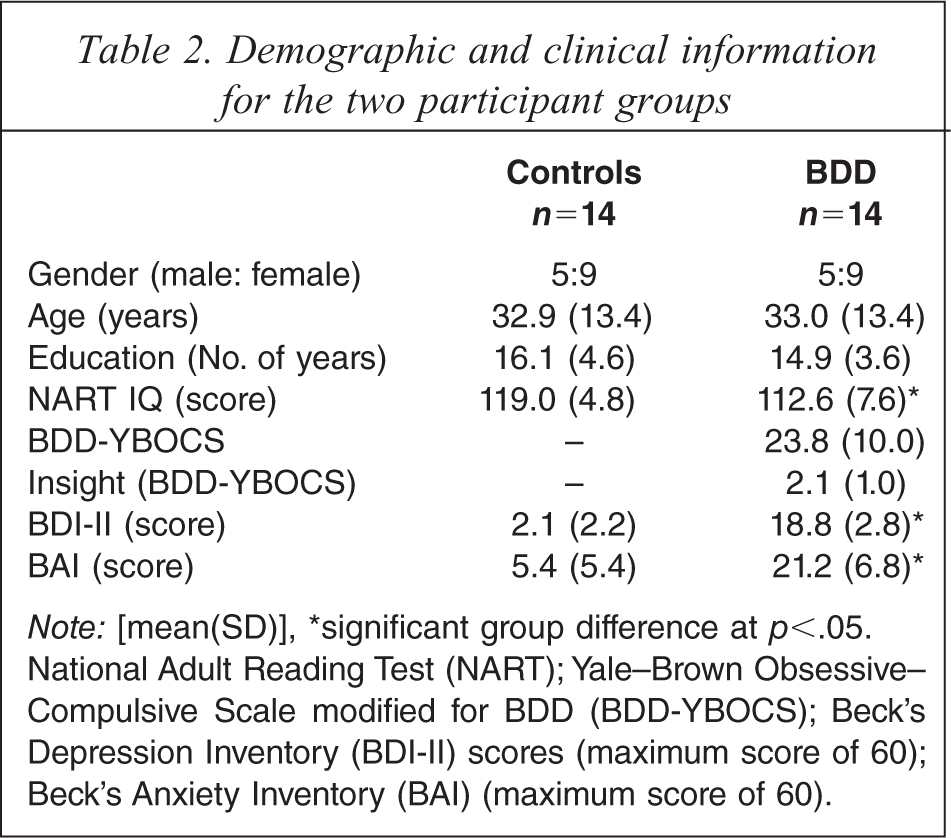
Note: [mean(SD)], ∗significant group difference at p<.05. National Adult Reading Test (NART); Yale-Brown Obsessive-Compulsive Scale modified for BDD (BDD-YBOCS); Beck's Depression Inventory (BDI-II) scores (maximum score of 60); Beck's Anxiety Inventory (BAI) (maximum score of 60).
Procedure/design
All participants were assessed during a single visit of approximately 3 h duration. Written informed consent was obtained after the procedures had been fully explained. A test battery consisting of a clinical interview (for demographic and clinical information) and a number of self-rated questionnaires (for delusional thinking and cognitive style assessment), was administered to each participant individually. Anonymity was preserved for individuals. Participants were financially compensated for their time commitment and travel expenses. The University of Melbourne Human Research Ethics Committee approved the study, the work was undertaken and that it conforms to the provisions of the Declaration of Helsinki (1995).
Delusional thinking assessment
The Peters Delusional Inventory (PDI) [18] is a 21-item questionnaire, which examines the multidimensionality of delusions by examining the dimensions of distress, preoccupation and conviction. A number of scoring variables were extracted from the questionnaire: (i) the total percentage of ‘yes’ items endorsed; (ii) the mean distress, preoccupation and conviction of endorsed beliefs and (iii) an item analysis to examine which were the most commonly endorsed unusual beliefs. In addition, normal distributions were constructed to illustrate the frequency of items endorsed across the two samples.
Cognitive styles assessment
The Creative Experiences Questionnaire (CEQ) [25] is a 25-item self-report instrument that measures fantasy proneness. Some CEQ items allude to the developmental antecedents of fantasy proneness. Other items are related to intense elaboration of and profound involvement in fantasy and daydreaming. Still others pertain to associations and consequences of fantasizing. Items (e.g. ‘Many of my fantasies have a realistic intensity’) are rated as either true or false. The number of true answers is summed to obtain a total score out of 25; higher scores indicate higher levels of fantasy proneness.
The Rosenberg Self-Esteem Scale (RSES) [26] is a 10-item measure which assesses global self-esteem. The items (e.g. ‘I feel that I have a number of good qualities’) were rated on a four-point Likert scale (i.e. 1 = strongly agree, 4 = strongly disagree, with some items reverse scored), with a maximum score of 40; higher total scores indicate higher self-esteem.
The Self-Ambivalence Measure (SAM-19) [27] is a 19-item self-report instrument that measures the extent to which beliefs about self-worth are uncertain, conflicting and a source of anxious introspection. The items (e.g. ‘I doubt whether others really like me’) were rated on a five-point Likert scale (0 = not at all, 4 = agree totally), with a maximum score of 76; higher scores indicate higher self-ambivalence.
Statistical analysis
Group data from all the measures were compared using a one-way analysis of variance (ANOVA) or t test, alpha level of 0.05. First, the demographic data (gender, age and education) were analysed to confirm that the participant groups were appropriately matched. Second, the PDI and cognitive styles assessment data were analysed in separate ANOVAs. Third, the normal distributions were constructed illustrating the number of delusional ideas endorsed in each group. Fourth, an item analysis was performed to examine which were the most commonly endorsed unusual beliefs (this analysis was Bonferroni corrected at p <0.05/21 = p <0.002). Last, correlational analyses of the BDD data were performed to measure the strength of any relationships between levels of delusional thinking (i.e. PDI total percentage), illness severity and insight (i.e. from BDD-YBOCS) and the remaining cognitive styles and level of depression. To reduce type 1 error, probability was set at an alpha of 0.01 for the correlational analyses.
Results
Demographics
The two participant groups did not differ on age (F(1,27) = 0.001, p = 0.98) or years of education (F(1,27) = 0.57, p = 0.47), but compared to the healthy control (HC) group, the BDD group had significantly lower NART IQ scores (F(1,27) = 6.99 p = 0.01) (see Table 2). Due to the latter, it was initially decided to enter NART IQ as a covariate in all analyses of delusional thinking and cognitive styles data. However, the assumptions of homogeneity of regression and linearity were not met, thus the NART IQ was not used as a covariate. Levels of depression (BDI-II) and anxiety (BAI) were greater in the BDD group; entering these clinical characteristics as covariates did not change the significance of the results presented below.
Delusional thinking data
All statistical details are presented in Table 3. A simple one-way ANOVA showed that the BDD group differed significantly from the HC group on the total number of items endorsed on the PDI (total percentage of yes answers) as well as on PDI dimensions of Distress and Preoccupation, but not on Conviction. Unequal variances were obtained for Distress and Preoccupation, but additional t tests showed that with ‘equal variance not assumed’ the significance for these did not change. A normal distribution was plotted using the PDI (total percentage) to investigate the distribution of delusional thinking within the BDD sample. Figure 1 shows the distribution in both samples was normal, with the BDD sample showing a greater distribution.
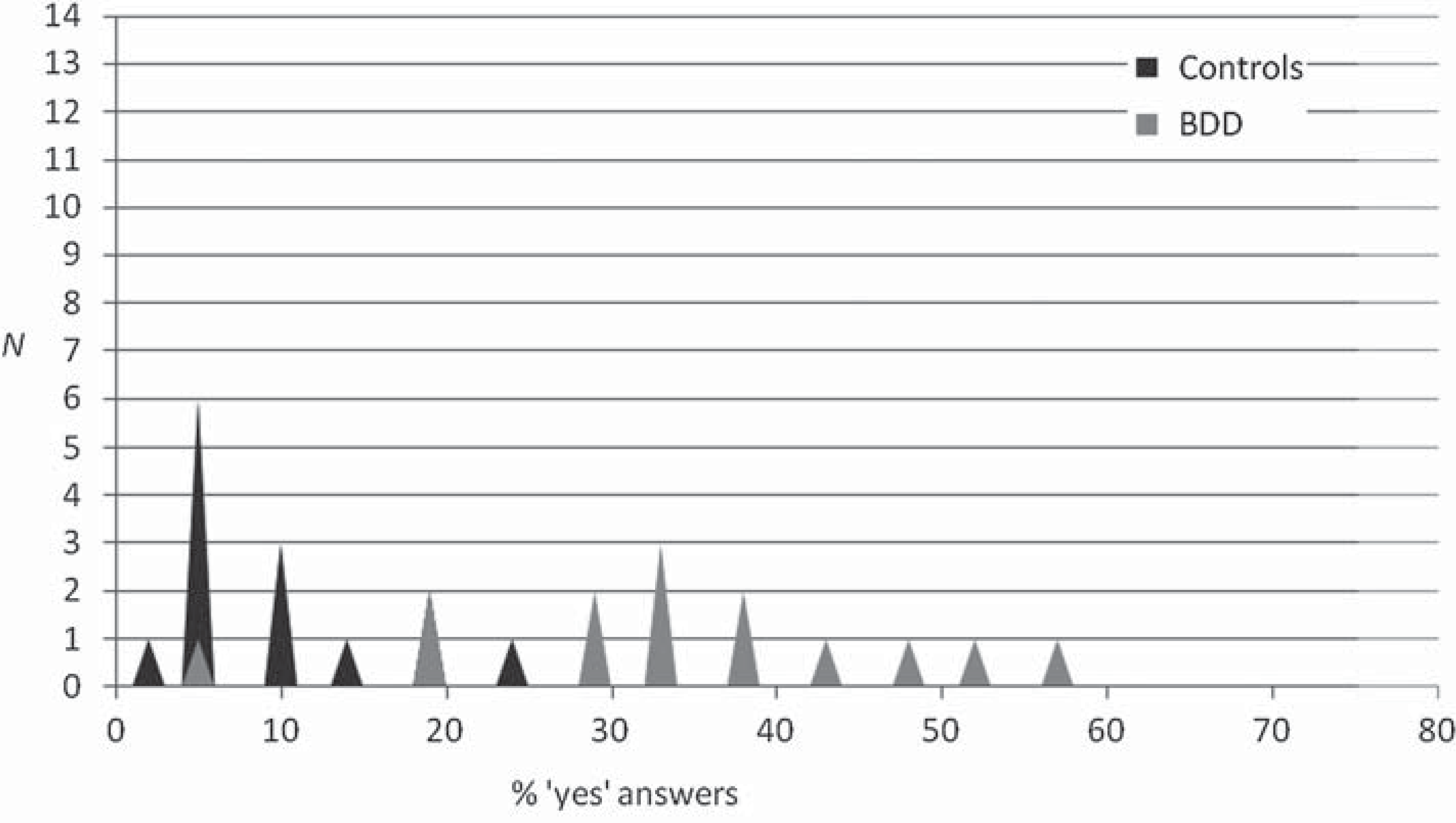
The number of participants in each group and their percentage ‘yes’ answered (out of 21 items) on the PDI.
Delusional thinking and cognitive styles assessment
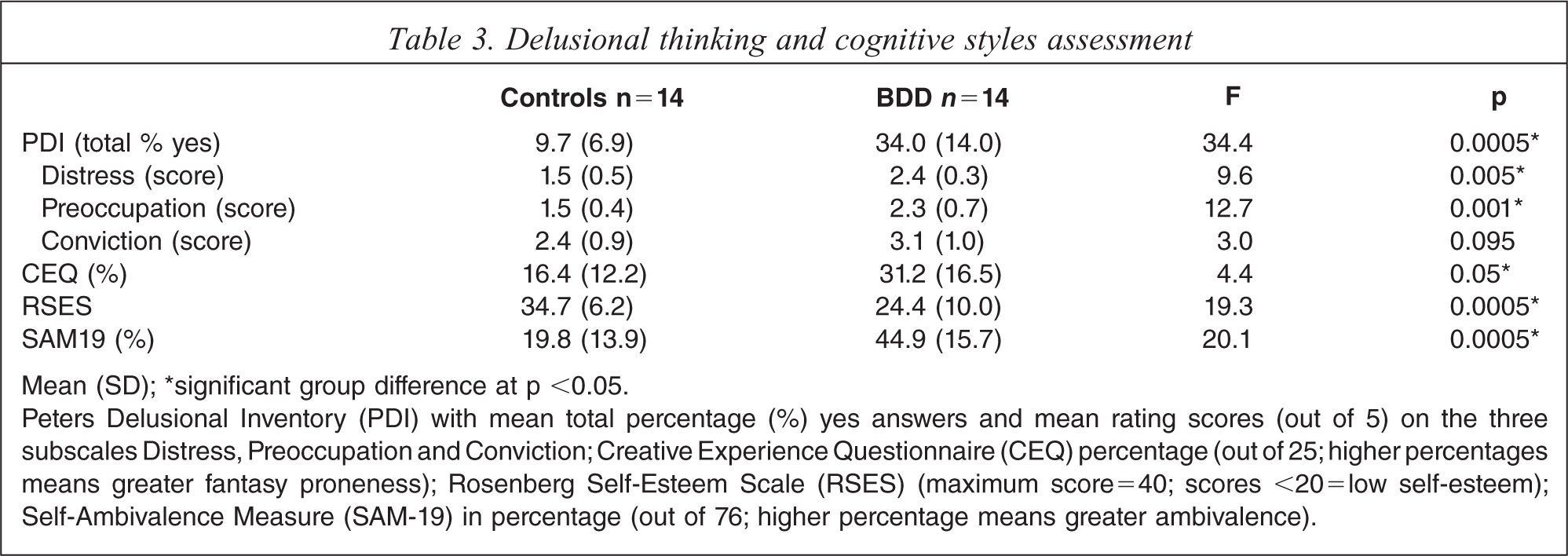
Mean (SD); ∗significant group difference at p <0.05.
Peters Delusional Inventory (PDI) with mean total percentage (%) yes answers and mean rating scores (out of 5) on the three subscales Distress, Preoccupation and Conviction; Creative Experience Questionnaire (CEQ) percentage (out of 25; higher percentages means greater fantasy proneness); Rosenberg Self-Esteem Scale (RSES) (maximum score=40; scores <20 = low self-esteem); Self-Ambivalence Measure (SAM-19) in percentage (out of 76; higher percentage means greater ambivalence).
Using simple t tests (2-tailed), the PDI measure was further analysed for group differences on the individual items. The BDD group differed significantly from the HC group on 6 out of 21 items. Item 15, a somatic delusion, survived Bonferroni correction at p <0.002; ‘Do you ever feel that people look at you oddly because of your appearance?’ (p <0.0005). Two further items showed a trend towards surviving correction, i.e. item 7 ‘Do you ever feel that you are a very special or unusual person?’ (p <0.007), classified as a grandiose delusion (see discussion); and item 1 ‘Do you ever feel as if people seem to drop hints about you or say things with a double meaning?’ (p <0.007), classified as a delusion of reference.
Cognitive styles data
In addition, simple one-way ANOVAs showed that compared to the HC group, the BDD group differed significantly on all other cognitive style measures including fantasy proneness (CEQ), self-esteem (RSES) and self-ambivalence (SAM19) (see Table 3).
Correlational analyses (BDD sample only)
There were no significant correlations between measures of delusional thinking, insight or illness severity and levels of depression and anxiety or other cogntive style using alpha = 0.01 correction.
Discussion
This study demonstrated that BDD patients have a greater number of delusional beliefs and different cognitive styles in comparison to age, education and sex-matched healthy controls. These included higher fantasy proneness, lower self-esteem and higher self-ambivalence. In addition, delusional thinking in BDD was associated with greater levels of distress and preoccupation than in controls. The data did not support a relationship between specific cognitive styles in BDD and symptom severity, level of insight or level of delusional thinking.
Previous studies utilizing the PDI in general population samples has found means for total item endorsement between 6.5 and 7.7 (out of 21) [18,28], which is slightly lower than the mean for control group (who endorsed an average of 9.7 items). Despite this, our BDD patients still endorsed three times as many delusional beliefs as healthy controls. An examination of the normal distribution of the two groups established that the BDD patients’ delusional ideas were indeed on a continuum, with some patients endorsing no or few delusional ideas and others up to thirteen different delusional beliefs. Thus, the lack of a bimodal distribution indicates there were not two discrete groups, supporting the notion that BDD should not be dichotomized on the basis of delusional thinking, as it currently is in the DSM-IV-TR.
The data presented here corresponds with studies that have examined dysfunctional beliefs or impaired thinking in obssessive–compulsive disorder (OCD). Clinical observations suggest that some OCD patients have prominent dysfunctional beliefs associated with their obsessions and compulsions, while other patients do not show this pattern. Empirical data has shown that dysfunctional beliefs do indeed lie on a continuum in OCD [29]. This similarity between BDD and OCD supports arguments for the inclusion of BDD within the obsessive–compulsive spectrum disorders (OCSDs) [1].
After somatic delusions, the most commonly endorsed delusions were delusions of reference and grandiosity. Delusions of reference have been noted in other studies of BDD [10]. The authors are not aware of other reports of high grandiosity in BDD. Importantly, when one examines the item used to classify grandiosity in the PDI it must be noted here that the wording may have not been interpreted in a positive manner by the BDD patients. Indeed, BDD patients probably interpret being an unusual person as relating to their perceived appearance flaw. In our clinical experience BDD patients are usually self-denigratory rather than grandiose. Interestingly, however, the level of conviction with which unusual beliefs are held in BDD, was no different from that found in the healthy controls. However, the groups differed on distress and preoccupation, with unusual beliefs being more distressing for the clinical group. This finding suggests that levels of distress should be the target of any psychological intervention.
Compared to the healthy controls, the BDD group showed higher levels of fantasy proneness. Whereas the PDI measures delusional ideation, the CEQ measures fantasy proneness, which is used as a label for individuals who exhibit a deep, profound and longstanding involvement in healthy fantasy and imagery. Fantasy proneness is closely associated with the concept of absorption and both are often interpreted as manifestations of the higher order trait ‘openness to experience’. Whereas absorption is essentially interactive and triggered by external events, one might consider fantasy proneness to be more ‘self-involved’ and stimulated by internal as well as external sources. Research by Lynn and Rhue [30] demonstrated that fantasy proneness is a benign trait and that most fantasizers are relatively well adjusted people. Alternatively, it has been argued that fantasizing can serve as a coping mechanism for traumatized individuals [31,32]. In the current study the data suggested that the BDD group showed higher levels of imagination compared to the healthy controls and perhaps more self involvement. As with the PDI, the spread of scores (i.e. percentage yes) on the CEQ varied on a continuum. The scores ranging from 8–60% in the BDD group, compared to 0–52% in the control group.
This study confirmed low self-esteem in BDD and also illustrated high self-ambivalence. Low self-esteem in BDD has been associated with their impossible standards of perfection resulting in self-critical judgements of parts of their bodies as ugly. Higher self-ambivalence in BDD suggests that BDD individuals may have difficulty synthesizing self-views and may perceive their self-concepts in terms of dichotomies. Self-ambivalence relates to one's description or evaluation of one's self, which can fluctuate from one extreme to another (positive to negative) such that sequential self-descriptions are felt to be contradictory. It is possible that the perfectionist and obsessive–compulsive behaviours reported in BDD are compensatory mechanisms that restore self-esteem in the face of such contradictory self-descriptions. In addition, self-ambivalence does not necessarily refer to whether the self is regarded as positive and/or negative. Having high self-ambivalence may result in BDD individuals continuously redefining their self-concepts as their self-evaluations fluctuate from one extreme to another and are felt to be contradictory. A focus on excessive personal preoccupation may also influence self-processing increasing self-ambivalence in the same way that checking increases doubt in OCD.
Depression and anxiety levels were found to be higher in BDD compared to healthy controls. The level of depression in BDD (mean score = 19) was shown to be mild-to-moderate (maximum score being 60). Similarly, anxiety in BDD (mean score = 21) was shown to be low-to-moderate (maximum score being 60). Interestingly, neither depression nor anxiety interacted or correlated with our other measures, suggesting that group differences on these measures are not due to changes in mood.
The data presented here have a number of implications with regard to the treatment of BDD [33]. First, our finding of a greater number of delusional beliefs in BDD suggests that adapting techniques from cognitive behavioural models of delusional thinking may be useful in BDD. Further, the finding of high self-ambivalence in BDD provides a basis for including self-ambivalent perceptions as a cognitive style within cognitive behavioural models of BDD.
The major limitation of this study was the small sample size. However, given the paucity of literature in the field and the large effects reported here, the significance of the data cannot be overlooked. Another limitation is the marginally lower NART IQ scores in BDD patients, which raise the possibility that group differences were related to IQ rather than the presence of BDD. NART IQ was not significantly correlated with any of the experimental measures, suggesting that group differences were not the result of lower IQ in the BDD group.
Conclusion
Our finding that delusional beliefs in BDD vary on a continuum from none to many rather than being either present or absent suggest that BDD should not be dichotomized in the DSM-IV-TR on the basis of delusional thinking. Delusional thinking in BDD was associated with greater levels of distress and preoccupation than in controls, with somatic delusions being the most commonly endorsed theme in BDD. BDD was also associated with higher fantasy proneness, lower self-esteem, higher self-ambivalence and higher levels of anxiety and depression, although these cognitive styles and mood factors were not correlated with delusional thinking.
Footnotes
Acknowledgements
This research was funded by the Mental Health Research Institute of Victoria. There are no conflicts of interest.