
Abstract
Keywords
Aggression is associated with many maladaptive outcomes for young people, their families and their social networks, making it a major public health concern. It is a core feature of disruptive behaviour disorders, and its negative impact, especially as violence, can be devastating. Indeed, physical aggression throughout childhood and adolescence is one of the most important predictors of criminal offending in later adult years [1,2]. When aggression occurs within the context of a disruptive behaviour disorder such as attention deficit hyperactivity disorder (ADHD), with which it has a greater than chance association [3], it predicts poorer outcomes compared to individuals with ADHD alone [4,5]. According to Barkley [6], emotional dysregulation in ADHD results from a primary deficit in behavioural response inhibition that drives further deficits in self-regulatory domains. Consequently, he states, children with ADHD have stronger emotional reactions to emotionally charged events as well as less ability to regulate emotion and arousal states in the service of goal directed behaviour, which can often develop into aggressive behaviour [7].
As well as being associated with conditions such as ADHD, aggression as a symptom is a criterion for the diagnosis of oppositional defiant disorder (ODD) and conduct disorder (CD), which are characterized by oppositional, hostile and rule breaking behaviours [8]. During the course of ADHD, oppositional and aggressive behaviours may begin to appear during primary school (6–12 years) in 40–70% of cases, with 25–45% receiving a comorbid diagnosis of CD towards later years of primary school (8–12 years) [9]. This comorbidity has a substantial negative impact on the functioning of children with ADHD. Greater social dysfunction [5], greater impairment on tasks measuring memory and visuomotor skills, more behaviour problems as well as a greater general impairment in daily functioning [10] are often exhibited in individuals with ADHD who are highly aggressive compared to those who are not.
Comorbidity of ADHD with aggression or ODD/CD has been associated with greater psychosocial adversity compared to those with ADHD alone [11]. Parental psychopathology, family functioning and parenting style, parental relationship and peer interactions [12,13] are some of the main adverse psychosocial factors associated with the development of aggression. High rates of antisocial personality disorder, depressive disorders and substance abuse/dependence disorders have been found in parents of children with aggression [14]. However, the presence of any psychiatric disorder experienced by the parent is potentially a risk factor for the development of aggressive behaviour in children, via interfering with and diminishing the quality of the relationship between the child and parent [13,15].
Family dysfunction has been shown to predict higher levels of childhood aggression [16] and higher rates of disruptive behaviour disorders such as ODD [17,18]. Further, hostile and aggressive interactions in families tend to amplify themselves, leading to greater and more intense conflict within these families [17,19,20]. Parental discord and poor parental relationship quality are additional factors that disrupt a child's familial environment [17,21,22]. Persistent marital conflict between parents has been associated with more behavioural problems in children, including antisocial behaviours and/or ODD [23].
Impaired peer interactions are also apparent for the aggressive child: children with aggression and/or ODD symptoms show greater levels of social impairment and social difficulties in peer interactions [18]. These problems in social interactions are usually associated with a hostile attribution bias [24] that leads to more rejection of aggressive children by their peers [25,26], resulting in fewer and poorer quality friendships.
For aggressive behaviour to be considered clinically pervasive in an individual's life, it must occur in more than one context [8]. Therefore, it is important to consider the factors contributing to aggressive behaviour in both school and home contexts. There are typically three types of informant used in studies of aggression: child, parent and teacher. Of the three, self-report by the child or adolescent is the least used, with the lowest valid reporting of their own disruptive behaviour (when compared to adult sources), and under-reporting of symptoms is generally the norm [27,28]. Additionally, the child's expression of symptoms through observation may also be reduced in the structured clinical interview setting [29].
It is generally agreed that parent and teacher reports provide a more valid picture of disruptive and rule breaking behaviours; however, agreement on presence and type of diagnosis (e.g. ADHD subtype) between these two types of reports is often quite poor [30,31]. Both informant types are subject to their different standards; opportunities to observe the behaviour as well as the impact of their own interaction with the child [31]. Use of only one of these sources also under-identifies those children with disruptive behaviour symptoms [27]. The information provided by each is therefore unique and complementary, and both should be considered to achieve a more complete account of behaviour.
The present study therefore sought to investigate the relative associations of a selection of key psychosocial factors to reports of aggression in the home and school contexts. Accordingly, both parent and teacher ratings of aggressive behaviour were examined. Our aim was also to focus on the aggressive behaviour exhibited by children and adolescents with ADHD, as the presence of aggressive behaviour has been shown to contribute to a worsened prognosis for individuals with ADHD. Accordingly, a large sample of children and adolescents diagnosed with ADHD (aged 6–16) was obtained. Several psychosocial factors were assessed, including measures of parental psychopathology, family dysfunction and parental relationship and child/adolescent interpersonal relationships. It was hypothesized that those children with parents who have higher levels of psychopathology, higher family dysfunction, greater parental relationship difficulties and who themselves have more problems in interpersonal relationships would exhibit higher levels of aggression as rated by both parents and teachers.
Method
Participants
Information was collected over a 5 year period from children and adolescents consecutively referred by school support staff from primary and secondary school settings for clinical assessment in the Academic Child Psychiatry Unit (ACPU) at the Royal Children's Hospital in Melbourne. Children and adolescents who met criteria for an ADHD diagnosis (722) were identified and selected for inclusion in the investigation. ADHD diagnosis was determined using the parent version of the Anxiety Disorders Interview Schedule for Children (A-DISC) [32], and included all three DSM-IV-TR subtypes. The A-DISC is a semi-structured interview designed to diagnose psychiatric disorders in children and adolescents in accordance with DSM-IV criteria. It is a reliable and clinically valid instrument for determining child and adolescent diagnoses (kappa coefficients from 0.62 to 0.92) [33]. To receive a diagnosis of ADHD, parents had to positively respond to a series of questions relating to hyperactivity–impulsivity, inattention, or both, and provide an overall rating of impairment or interference caused by the symptoms as 4 or greater on a 0 (no problem) to 8 (extremely severe/disturbing/disabling problem) visual analogue scale. From this group, those with a full scale IQ (FSIQ) score lower than 70, as derived from the Wechsler Intelligence Scale for Children, third edition (WISC-III) or fourth edition (WISC-IV), were excluded from the study. The WISC-III and WISC-IV are standardized clinician administered measures of general intellectual ability for children aged six to sixteen years [34,35]. Both are psychometrically sound instruments, although the properties of WISC-IV are more robust than previous editions [36].
In total there were 676 children and adolescents (mean age = 10.26, SD = 2.88) in the final sample, consisting of 531 males (mean age = 9.97 years, SD = 2.8) and 145 females (mean age = 11.30, SD = 2.94). Rates of the ADHD subtypes present in the sample of children and adolescents were: 464 (68.6%) diagnosed with ADHD-CT, 166 (24.6%) diagnosed with ADHD-IA and 46 (6.8%) with ADHD-HI, although these were not differentiated for the purposes of the study. Comorbidity rates of other diagnosed psychiatric disorders, as determined using the A-DISC, were: 521 (77.1%) ODD; 54 (8.0%) CD; 106 (15.7%) major depressive disorder (MDD); and 298 (44.1%) dysthymic disorder (DD).
Measures
Child Behaviour Checklist (CBCL) and Teacher's Report Form (TRF)
These measures [37,38] consist of 118 statements regarding possible emotions and behaviours exhibited by a child, and are rated by the parent and teacher respectively on a three-point scale (0 = not true, 1 = somewhat or sometimes true, 2 = very or often true). Both provide dimensional subscales for a range of externalizing and internalizing symptoms. A subscale raw score and T score for aggressive symptoms are derived from each form, based on responses to aggression-related items. Subscale T scores greater than 69 on this scale are considered to be in the clinical range. Both forms have good reliability and validity [38].
The Hopkins Symptom Checklist (HSCL)
The HSCL [39] is a self-report measure of psychopathology completed by parents. It consists of 58 items, rated on a four-point scale, concerning the thoughts, feelings and behaviours representative of symptom configurations observed in psychiatric outpatient populations. It provides symptom subscale scores that include depression, anxiety, interpersonal relationships and obsessive–compulsive behaviours. A total HSCL score, the sum of all subscales, provides an indication of overall psychopathology with scores greater than 90 representative of measurable emotional distress [40]. All subscale scores are standardized, and higher scores equate to greater levels of symptom manifestation, based on data from normative clinical and non-clinical samples. It has demonstrated validity and reliability, with internal consistency reliabilities ranging from 0.84–0.87 and one week test–retest reliabilities of 0.75–0.84 for the five symptom domains [39].
Family Assessment Device
The Family Assessment Device (FAD) [41] questionnaire measures an individual's perception of their family. Completed by a parent, it requires them to rate how well each of the 53 items describes their family on a scale from one (healthy functioning) to four (unhealthy functioning). Items relate to one of six areas of family functioning which include problem solving, communication, affective responsiveness, affective involvement, role definition and behaviour control. An overall measure of family psychopathology is given by the general functioning score. Higher scores suggest greater family dysfunction. All seven scores are standardized. Construct and criterion validity have been demonstrated in clinical and non-clinical families, and subscale reliabilities range from 0.72 to 0.92 [41].
Spanier Dyadic Adjustment Scale (DAS) Relationship Questionnaire
An abbreviated seven item form of the original Dyadic Adjustment Scale (DAS) [42] was used, which assesses the quality of marriage and similar dyads. Parents indicate their level of agreement or disagreement on a six-point scale. Items relate to degree of consensus, cohesion and satisfaction within the dyadic relationship. It has been found to differentiate persons dissatisfied with their marriage and those who remain living together, with lower scores indicative of poorer dyadic adjustment. Scores on each of the seven items were standardized and added to form a total DAS score. Good reliability (alpha coefficient 0.76) and good content, criterion-related and construct validity have been established in married and divorced samples using the abbreviated form [42,43].
Child interpersonal relationships
The interpersonal relationships measure from the A-DISC [32] was used to indicate whether each child or adolescent experiences difficulties in forming and maintaining peer relationships. It is based on responses by parents to two questions asking whether the child has trouble making friends and, once they have made friends, whether they have trouble keeping them.
Procedure
This investigation was conducted as part of a larger study exploring the relationship between behavioural features, genes and ADHD, and in accordance with ethical guidelines of the RCH and The University of Melbourne. Participants and their parents or carers were brought into the RCH for two 1.5 h sessions. Written informed consent was obtained at the beginning of the session after tests were clearly explained to participants and their parents. All measures were administered by a registered psychologist or clinically trained psychology student during these sessions, in a semi-structured interview. Tests and questionnaires were scored, and then entered onto the computer database.
Results
Descriptive statistics
All statistical analyses were conducted using SPSS 16.0 [44]. Mean scores obtained on aggression and the psychosocial measures, and the number of cases in the sample with valid information for each of the measures are shown in Table 1.
Sample size (n), mean and standard deviation (SD) for age, aggression measures and psychosocial measures
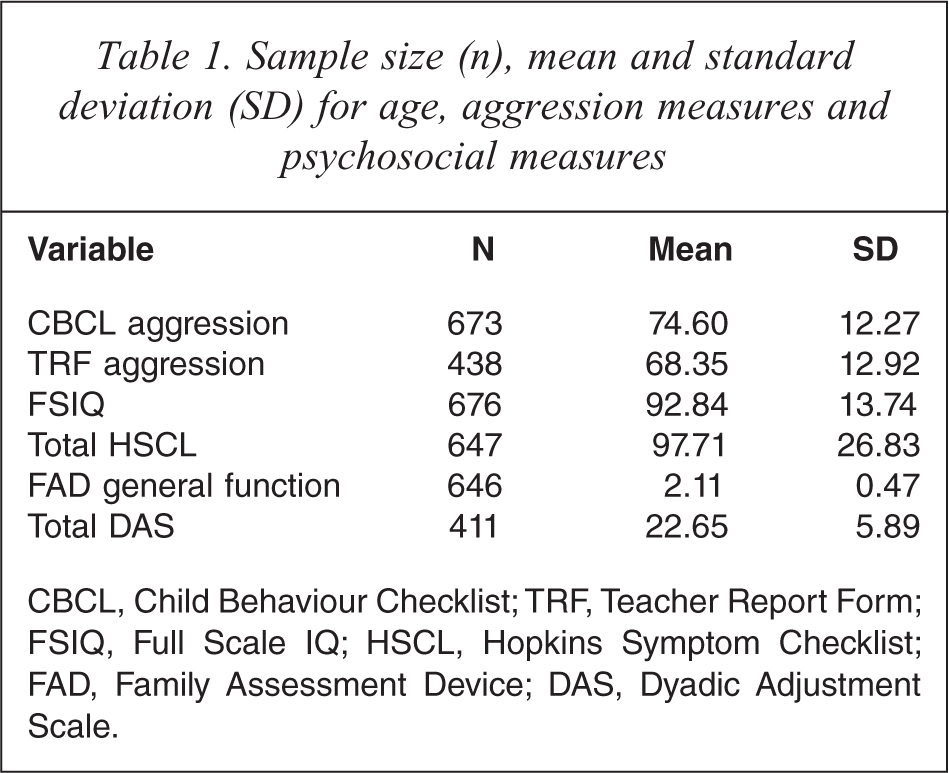
CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; FSIQ, Full Scale IQ; HSCL, Hopkins Symptom Checklist; FAD, Family Assessment Device; DAS, Dyadic Adjustment Scale.
Correlation between aggression measures
A Pearson product–moment correlation revealed parent and teacher measures of aggression were significantly correlated to a moderate extent, r = 0.29, p < 0.01 [45].
Gender differences
Given the majority of the sample consisted of males, any systematic differences between males and females in their scores on each measure could potentially bias the results. To explore this issue, a series of independent sample t-tests were performed comparing males and females on the aggression measures and each of the factors. The complete results of these t-tests are presented in Table 2. No significant differences in scores for males and females on either aggression measure were found. After Bonferroni adjustment, no significant differences in scores for males and females on the FAD, DAS, and HSCL scales were found. A Chi-square test for independence (with Yates Continuity Correction) indicated a significant association between gender and child interpersonal relationships, χ2 (1, n = 674) = 4.87, p = 0.027. In order to control for the differences between males and females on this latter psychosocial measure, gender was entered into the subsequent analyses of child interpersonal relationships for parent-rated and teacher-rated aggression.
Independent sample t-tests comparing males and females for aggression and psychosocial measures
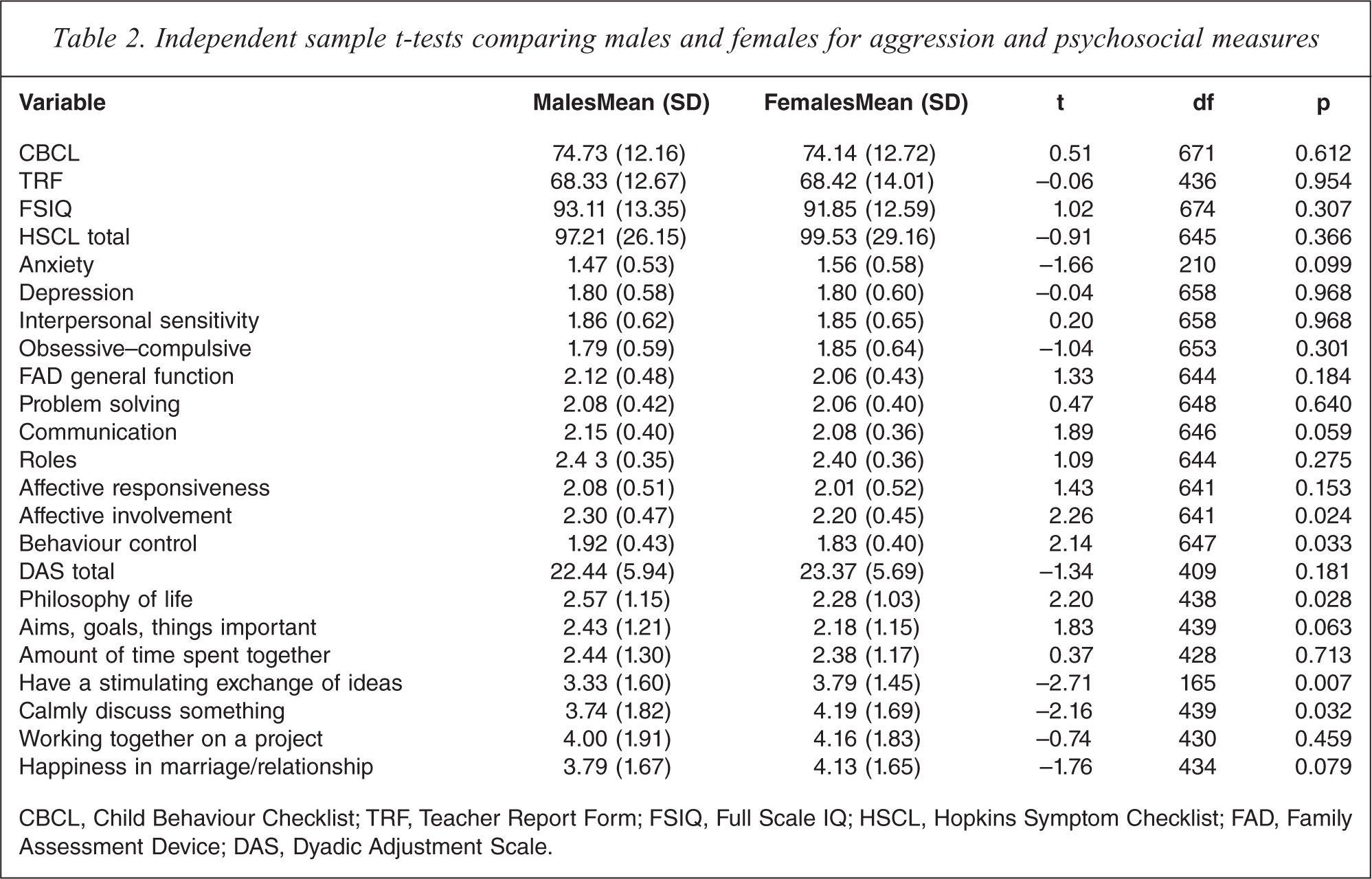
CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; FSIQ, Full Scale IQ; HSCL, Hopkins Symptom Checklist; FAD, Family Assessment Device; DAS, Dyadic Adjustment Scale.
Parent ratings of aggression
The relationship between parent-rated aggression and psychosocial factors was investigated in two stages of analyses. First, Pearson product–moment correlations were performed to determine the bivariate associations between parent-rated aggression and psychosocial measures, as reported in Table 3. Mild to moderate positive significant correlations were found for HSCL total and FAD general functioning, with high scores on each associated with higher levels of parent-rated aggression. In the second stage, separate multiple regression analyses were carried out for each psychosocial measure represented by multiple predictors. Only those subscales for which the overall measure for that factor was significantly correlated with parent-rated aggression in the first stage were further explored, to determine the associations between the specific components for each overall significant factor and aggression. As a result, the DAS (marital relationship quality) subscales were excluded. The results of these analyses are shown in Table 4. Bonferroni adjustment of the 0.05 alpha level was made for the number of related predictors in each of these analyses. The depression and interpersonal sensitivity subscales of the HSCL measure of parental psychopathology significantly predicted parent-rated aggression (1.3% and 1.7% variance respectively). Altogether 10.8% of variance in parent-rated aggression was accounted for by scores on the HSCL subscales. Of the FAD subscales, roles (2%) and affective involvement (1.2%) significantly predicted parent-rated aggression. In total, the six FAD subscales accounted for 6.9% of the variance in aggression. Finally, regression of parent-rated aggression onto the dichotomous variables interpersonal relationships and gender was carried out. Together they accounted for 3.5% of the variance in parent-rated aggression. Child interpersonal relationships also significantly predicted parent-rated aggression, accounting for 3.4% of the variance. As the number of children with problems making/keeping friends increased, so did the level of parent-rated aggression.
Pearson correlations between single psychosocial predictors and parent-rated and teacher-rated aggression
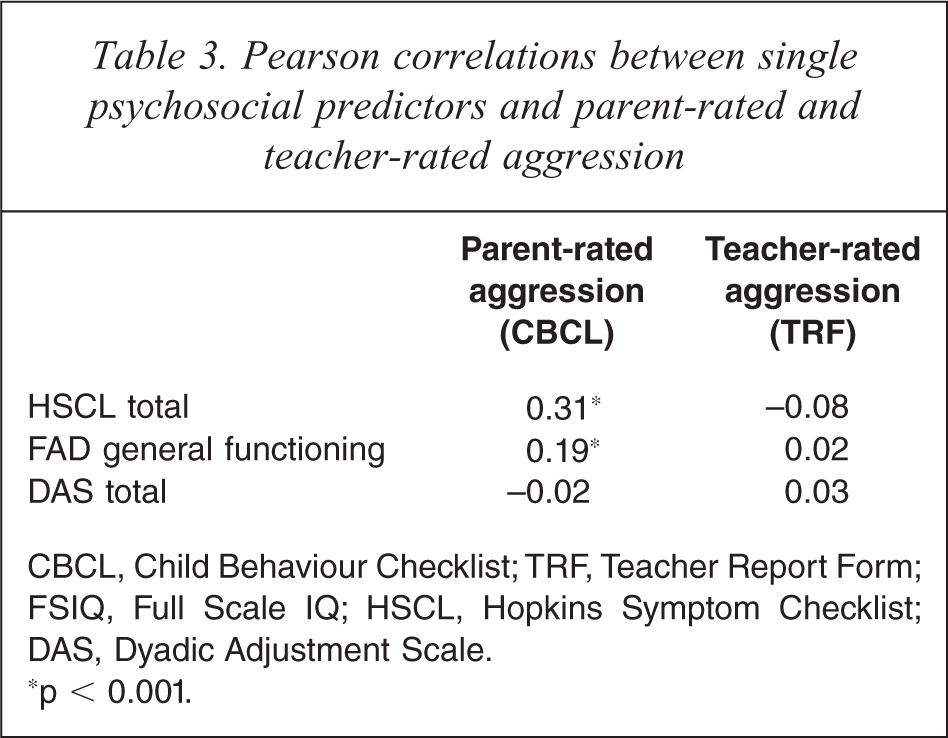
CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; FSIQ, Full Scale IQ; HSCL, Hopkins Symptom Checklist; DAS, Dyadic Adjustment Scale.
∗p < 0.001.
Separate standard multiple regression of Parent ratings of aggression (CBCL) on multiple psychosocial predictors
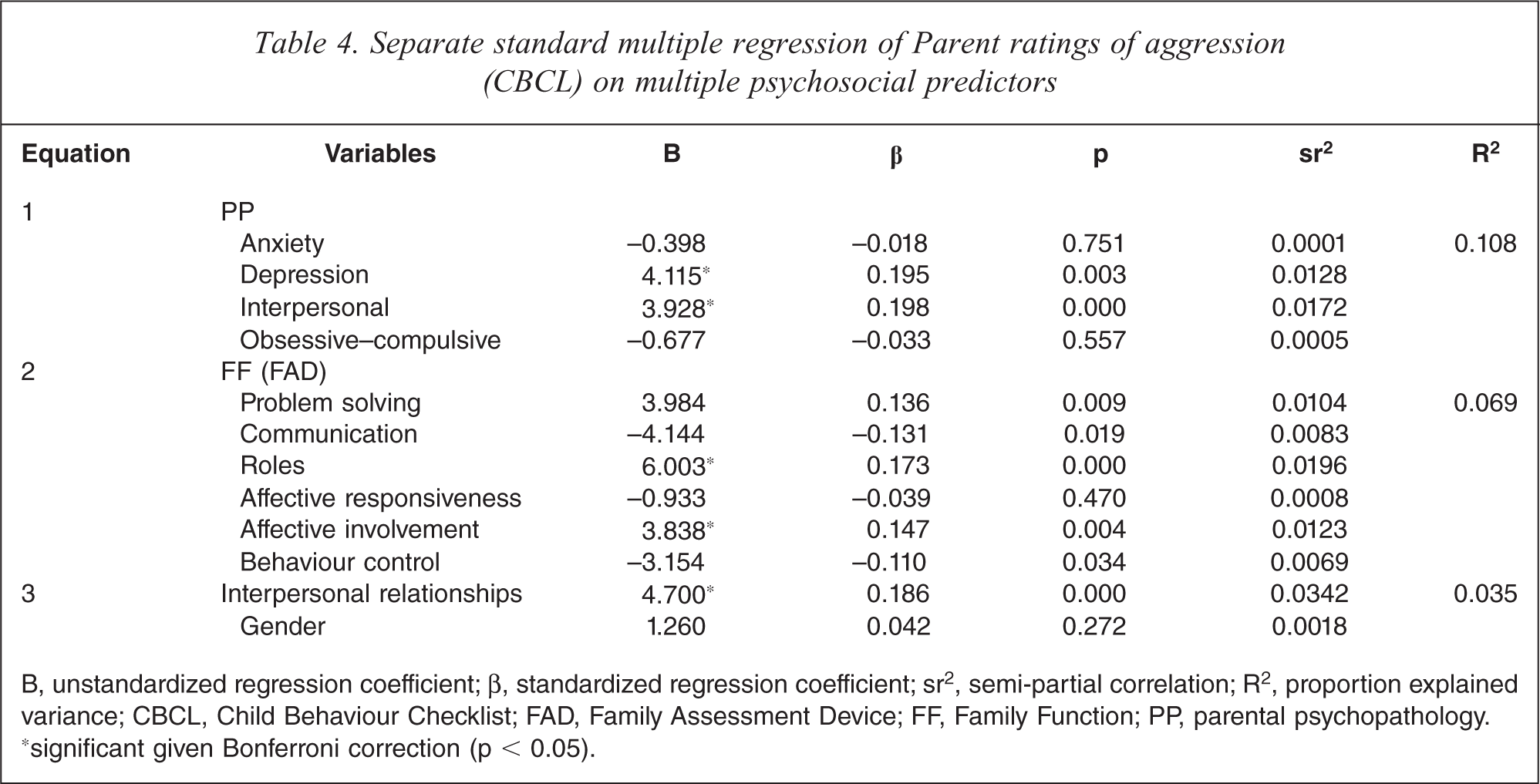
B, unstandardized regression coefficient; β, standardized regression coefficient; sr2, semi-partial correlation; R2, proportion explained variance; CBCL, Child Behaviour Checklist; FAD, Family Assessment Device; FF, Family Function; PP, parental psychopathology. ‘significant given Bonferroni correction (p < 0.05).
Teacher ratings of aggression
The relationship between teacher-rated aggression and each of the factors was investigated following the same procedure as the parent-rated aggression analyses. Total scores on the HSCL, FAD and DAS measures were not found to be correlated with teacher-rated aggression; however, standard multiple regression revealed child interpersonal relationship problems significantly predicted it (Table 5). It accounted for 1.3% of variance in teacher-rated aggression (the total model with gender included accounted for 0.8% of the variance in teacher-rated aggression). Higher numbers of children/adolescents with problems making or keeping friends predicted higher ratings of aggression by teachers.
Separate standard multiple regression of Teacher ratings of aggression (TRF) on multiple psychosocial predictors
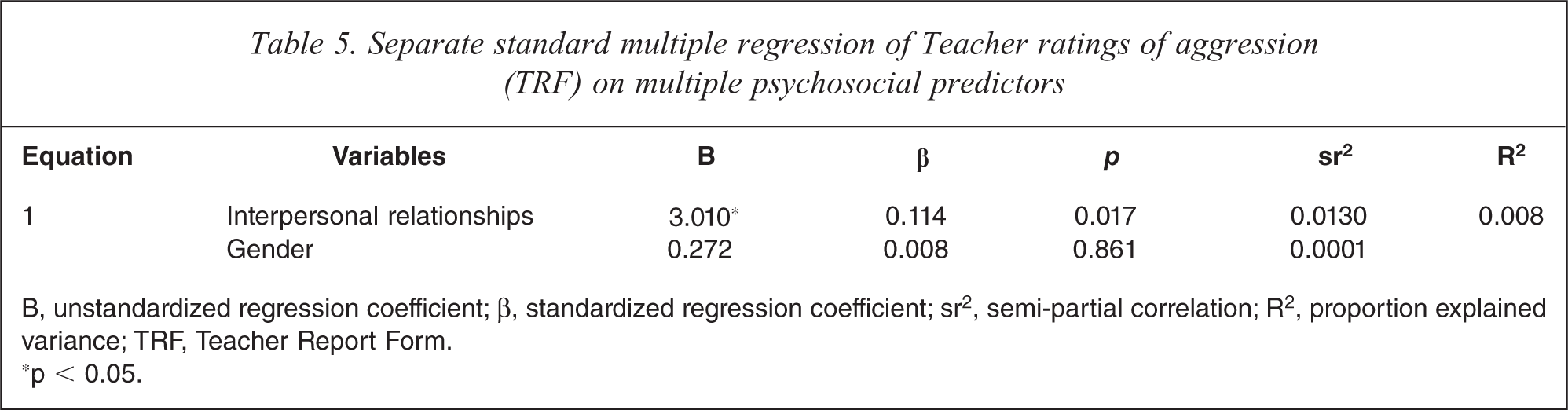
B, unstandardized regression coefficient; β, standardized regression coefficient; sr2, semi-partial correlation; R2, proportion explained variance; TRF, Teacher Report Form.
∗p < 0.05.
Discussion
The findings of this study support the contribution of several psychosocial factors including parental psychopathology, family dysfunction and children's peer relationship difficulties to parent ratings of aggression in the large sample of children and adolescents with ADHD. More specifically, high levels of self-reported parental depression and high levels of interpersonal sensitivity, that is, feelings of personal inferiority and inadequacy leading to discomfort in interpersonal interactions [39], were associated with higher ratings of aggression. This is consistent with studies that have linked poorer parental psychological adjustment to inconsistent and harsh child-rearing and disciplinary practices, which are associated with the development of aggressive behaviour and conduct problems [13,15]. In other words, children with parents who have more psychopathological symptoms are reported to have more behavioural problems/aggressive behaviour [46]. Poorer psychological adjustment may also impair parents’ ability to cope with aggressive behaviour displayed by their child in a healthy and productive manner, thus enabling its continuance.
Higher levels of dysfunction within the family unit were associated with higher parent-reported aggression levels in children and adolescents with ADHD. This included greater impairment in the overall ‘healthiness’ of the family (general functioning), as well as more problems establishing patterns of behaviour to deal with certain family responsibilities by family members (roles), and the amount of interest taken in the activities and concerns of family members (affective involvement). These findings fit well within the literature and the strong relationship between various familial and psychosocial factors with the development of aggression [13,15]. It is also consistent with those studies that have found the association between such factors and aggression to be greater when it is comorbid with ADHD [5].
Problems in interpersonal relationships outside the family evident in the child or adolescent were also related to higher levels of parent-rated aggression. This further supports well established findings of peer rejection and interpersonal problems, resulting in part from social cognitive processing biases occurring in highly aggressive children, extending it to children and adolescents with ADHD [26,47].
Unexpectedly, a measure of marital relationship quality was not associated with parent or teacher-reported aggression in children/adolescents with ADHD in the current study. This suggests that dissatisfaction in marriage and marriage quality is independent of the presence of aggressive behaviour in children, which is inconsistent with past findings indicating an association between marital conflict or dissatisfaction and child behavioural problems [23]. However, previous studies have found that persons who are divorced or separated report greater dissatisfaction, when reflecting on their marriage, compared to those still married or living with a partner [43]. Thus the results of the present study may have been biased by the fact that only those parents who were married or with a partner were able to complete the DAS, and that this potentially most dissatisfied group were excluded.
Interestingly, unlike parent-rated aggression, the only psychosocial factor associated with teacher ratings of aggression were problems in the child/adolescent's interpersonal relationships outside the family. As such, it was the only factor associated with both parent and teacher-rated aggression, suggesting that it is associated with aggression in both home and school contexts.
This difference in psychosocial factors associated with parent and teacher reports of aggression demonstrates the uniqueness of each perspective and the context on which it is based. This might reflect an informant bias or bias hypothesis (i.e. reflecting different domains that are considered important by parents or teachers in their judgement of aggressive behaviours), or situation specificity of the aggressive behaviour (a true variation in the child's aggressive behaviour across context) [30,48]. According to the results of the present study, a parent's rating of their child/adolescent's aggressive behaviour is associated with communication and conflict within the family context (family functioning), as well as the parent's own feelings and psychological status (parental psychopathology) and the way they perceive the quality of their child's peer relationships. On the other hand, a teacher's rating of the child/adolescent's aggressive behaviour is associated with peer relationships; an aspect which occurs in the school environment where the teacher is exposed to the child/adolescent's behaviour. Other factors such as parental mental health and family conflict are not directly observable in the school environment and hence are not associated with teacher reports of aggression in children and adolescents.
Given that all psychosocial measures in this study were based on parent reports, it is plausible that these associations may represent the influence of the parent's own mental health status on their perception of their child's behaviour, that is, their rating of aggression, rather than the actual manifestation of the behaviour. For instance, studies have shown that mothers with poorer psychological adjustment, including those with depression and anxiety-related symptoms, are more likely to perceive problem behaviours in their children than those who are better adjusted [49]. Instead of being a function of the child's actual level of problem behaviour, these perceptions are related to the mother's own level of psychological adjustment [50]. The dynamics of the parent–child relationship might also bear some influence, as described in a previous study that found parental reports of anxiety in children with ADHD were associated with negative affectivity linked to their child's disruptive behaviour, rather than fearful or phobic-type symptoms [51]. This highlights the potential role of the parent's emotional and behavioural dispositions not only in determining their child's behaviour, but also in determining their own perception of it.
Since the contribution of the significant psychosocial variables to the variance in parent-reported aggression was still relatively small, it suggests that there may be other contributors present that were not investigated in this study. These might include other familial or parental factors (e.g. socio-economic status, parenting style, quality of parent–child relationship, etc.) or other non-psychosocial factors such as deficient cognitive processing or temperamental factors [11,52,53]. This interaction of numerous factors is also evident from studies that have shown psychosocial risk factors to have the greatest impact on those who may already have a biological vulnerability to developing aggression, such as reduced serotonin activity in the brain [52].
The association between parent and teacher ratings of aggression was also relatively moderate, suggesting that substantial disagreement exists in their views of aggressive behaviour in children and adolescents with ADHD. This also is in line with more extensive research describing low concordance rates between parents and teachers in the prevalence of behavioural problems [28,30].
This study extends such findings by demonstrating differential contributions of psychosocial factors to parent and teacher reports of aggression in children and adolescents with ADHD. Such differences have important implications for both researchers and clinicians, who rely on measures based on reports from different informants in their work. They draw attention to the need to consider that reports of behaviour not only reflect the child's behaviour, but also reflect the nature of the child–informant relationship, as well as the informant's own psychopathology, emotionality and other contextual factors which moderate their perception of that behaviour.
Identification of factors associated with aggression in ADHD in the home and school contexts can help direct strategies to help prevent and manage aggressive behaviour that are appropriate and beneficial to each setting. This would include involvement in psychosocial programmes that target healthy family functioning, better parenting practices and coping with problem behaviour, as well as strategies that children and adolescents can use to control their own behaviour in social interactions at home and school. This further endorses psychosocial treatments for ADHD that have already been shown to improve aggressive and ODD symptoms in the short term [54].
The findings of the present study should be viewed within the context of several limitations: first, children and adolescents who participated in this study were clinic-referred and therefore may be more likely to exhibit greater levels of psychopathology compared to community-based samples. The combination of age groups (6 to 16 years) due to the high rates of DBDs throughout childhood and adolescence might mean that the profiles of aggression described in this study are not equivalent, as longitudinal studies have described the nature and level of aggression as varying systematically with age [55,56]. Nonetheless, this study shows those factors that may commonly contribute to aggressive behaviour in both adolescence and childhood, suggesting that these factors are consistent with the expression of aggression across all age groups.
Second, comorbid psychiatric disorders were not controlled in this study, and these comorbidities may have been a confound to the outcomes observed in this study. The rates of comorbidities in sample used in this study were high, and this is reflective of the ADHD comorbidity rates found in other population studies [3]. Given the high rates of comorbid conditions often seen in individuals with ADHD, this could be viewed as a strength, providing information that can be generalized to a wider population of those with ADHD, without being restricted to that minority with ‘pure’ ADHD. Future research that looks at the effect of these factors on aggressive behaviour in more distinct phenotypic groups would add further insight into the nature and risk factors associated with aggression in different psychiatric profiles.
Third, this study also combined all three ADHD subtypes. Differences have been reported in the symptomatology and impairments between these subtypes [57], suggesting that there may be some differences in the factors contributing to each, but these are few, and there is greater evidence supporting their similarity than not [58]. Nonetheless, the aim of this study was to investigate factors contributing to aggression in the heterogeneous context of ADHD, hence the findings represent information that is relevant in these terms.
Future studies with longitudinal designs would enable us to better understand the temporal ordering of correlates of aggressive behaviour and extend beyond the level of association, identifying causal relationships between key risk factors and the development of aggression. Making use of more objective measures of aggression and risk factors in these future studies would aid in removing the bias associated with informant perceptions, to ascertain clearer relationships.
In summary, this study identifies important differences in psychosocial factors associated with parent versus teacher ratings of aggression in a clinically heterogeneous group of children and adolescents with ADHD. The findings highlight how factors contributing to reports from different informants are unique, and highlight the need to consider the contextual factors that influence the expression of aggressive behaviour as well as influence informants’ perceptions of it. These differences have clear implications for both the study and clinical assessment of aggression and its measurement using reports from various informants.
Footnotes
Acknowledgements