
Abstract
The Australian Bureau of Statistics estimated that in 2003 there were over 2.5 million informal carergivers in Australia who provided assistance to family members or friends who needed help due to a disability or old-age [1]. Of these, 475,000 were primary caregivers: that is, the person providing the majority of informal help to a person in these circumstances. The annual cost of substituting formal assistance for the contribution of these informal caregivers has been estimated at over $30 billion [2]. The aging profile of the Australian population is likely to lead to increased demand for, and reliance upon, informal care [3,4]. Thus, informal caregiving is a topic with considerable contemporary policy relevance. In this context, research to inform and provide an empirical basis for health and social policies to better support Australia's caregivers is essential [5–8]. Much of the existing caregiver research is focused on specific disabilities or disorders (particularly dementia, psychiatric illness and intellectual disabilities). However, there is also a body of research (including Australian research) that has considered a broad range of caregivers, but is focused at the population level [7,9–11]. It is this research which is most directly relevant to informing general carer policies [8] and is the focus of this investigation.
The association between mental health and caregiving is well documented, with caregivers reporting significantly more psychological distress, poorer wellbeing, greater rates of clinical psychiatric disorders, and a greater number of depression and anxiety symptoms than non-caregivers (e.g., [5–7,10,12,13–20]). Recent Australian research has shown that caregivers have poorer mental health than other groups that are generally recognised as having a high risk of psychiatric morbidity, such as the unemployed [7]. Longitudinal data also demonstrate that the onset of distress coincides with transitioning into a significant caregiving role (e.g., [21]). Evidence such as this illustrates the personal costs associated with caregiving. However, there are issues in much of the caregiver research which limit its direct applicability to a general policy setting (e.g., small sample size, lack of representativeness and generalisability, methodological and analytic weaknesses; see [11,15]). Similarly, although much research has investigated the personal and situational factors associated with the poor mental health of caregivers (e.g., financial and employment concerns, burden of care, type of disability/condition, social support, coping strategies, etc; [6,7,10,13,15,19,20,22–26]), a greater emphasis is needed on research methodologies which evaluate whether it is these factors that account for differences in the mental health of caregivers and non-caregivers. Further, from a policy perspective, research is needed that investigates modifiable factors that can be targeted and changed by policy interventions [5].
Pearlin and colleague's stress process model provides a theoretical framework to conceptualise the potential roles of different stressors and intervening factors on caregiver outcomes such as mental health [27]. The stress process model differentiates between contextual factors (such as gender, SES, family composition, relationship), primary stressors (factors directly associated with the level of need of the care recipient such as type of disorder, impairment and behaviours, level of need, intensity of care), secondary stressors (which reflect the impact of caregiving on other roles/circumstances such as employment, financial situation, family functioning, and psychological constructs such as mastery and self-esteem) and exacerbating or mediating factors (such as social support, coping strategies). Evidence suggests that the effect of primary stressors on caregiver mental health may be indirect and mediated through the secondary stressors (e.g., [5,28]). This is important as it potentially provides a target for interventions. In this study we examine three general factors which can be labelled as either secondary stressors or mediating factors in Pearlin's stress model. They are financial circumstances (including employment and material deprivation), burden or role strain, and social aspects including positive social support and conflict with family and friends. These factors have been shown to be related to caregiver's mental health [5,7,10,13,17,20,24,27–30]. We also consider primary stressors and contextual factors (caregivers’ physical health, socio-demographic characteristics). The novel aspects of the current project include the analysis of data from a representative community survey of older adults, and the use of appropriate analytical methods to explicitly evaluate whether these factors account for caregivers’ poor mental health relative to non-caregivers.
The current study considers data from community dwelling adults aged between 64 and 69 years. Individuals in this age group are of particular interest as the prevalence of caregiving is high [1]. The age range also coincides with the major late-life transition from work to retirement and, therefore, the circumstances of caregivers of this age may differ from younger caregivers who are more likely to also be engaged in work. There is, for example, research evidence that differences in mental health of caregivers and non-carers are not as pronounced among older adults compared with younger age groups [7,10]. Therefore, it may be particularly informative from a policy perspective to identify mediating and potentially protective factors for caregivers in this age range.
The main aim of this study was to identify mediating factors that could provide a basis for intervention and policy options to better support older Australian carergivers. Based on previous research, it is hypothesized that caregivers will demonstrate poorer mental health than non-carergivers. It is also hypothesized that the poorer mental health of caregivers compared to non-carergivers will largely be explained by contextual (age, sex, physical health) and secondary stressors such as situational and social factors.
Method
Sample
Data are from the PATH Through Life Project, a large community survey examining the health and wellbeing of three cohorts of adults sampled from Canberra and the neighbouring town of Queanbeyan in south-eastern Australia. This project analyses the second wave data for the older cohort (born between 1937 and 1941), which was conducted in 2005 when the participants were aged between 64 and 69 years. The sampling frame was the Electoral Roll for Canberra and Queanbeyan (registration on the electoral roll is compulsory for all Australians with few exemptions). The response rate at wave 1 was 58.3% (with 2,551 people interviewed) and 2,222 of these (1,147 men and 1,075 women) were subsequently re-interviewed at wave 2 (a retention rate of 87%).
A trained interviewer met the participant at a convenient location, usually the participant's home or the Centre for Mental Health Research at the Australian National University. Postal and email options were offered for those who had moved interstate or overseas. Much of the data were entered directly by the participant on a laptop computer, though the interviewer administered physical and cognitive tests. The Human Research Ethics Committee of the ANU approved the study. Further detail of the survey including the sampling procedure are reported in Jorm et al. [31].
Measures
The survey covered socio-demographic characteristics, anxiety and depression, substance use, cognitive function, wellbeing, physical health, health habits, personality, current psychological risk factors, nutrition and caring. The components of the questionnaire relevant to the current study are outlined below.
Caregiving
Caregiving was assessed by the question ‘Do you provide care or informal assistance to a person with a disability, or a medical condition or to a person who is elderly?’. In addition, primary caregivers were identified as those who reported that they were ‘… the “primary carer” for someone? That is the person who provides the most care for an individual?’ Other items assessed the number of hours per week spent caring and the duration of the caregiving role. Those identified as primary caregivers were also asked about their relationship with the care recipient and the reason that care was required (physical disability, mental illness, cognitive disorder, other). This analysis is primarily focused on individuals providing a substantial level of care, defined as those who were either (i) primary caregivers, or (ii) providing greater than 5 hours of care per week.
Mental Health
The Goldberg anxiety and depression scales were used [32]. These scales each comprise nine items which assess symptoms of anxiety and depression in the last 4 weeks. Each scale produced a score from 0 to 9. This analysis used cut points of 5 on the anxiety scale and 2 on the depression scale which are recommended to identify clinically significant symptoms for follow-up in general practice. In addition, because of the strong positive association between these two scales (polychoric correlation of 0.67), a measure representing the sum of the depression and anxiety symptoms was also analysed (a count variable on which scores ranged from 0 to 18).
Socio-demographic covariates
Covariates included sex, marital/partnered status (current marriage or de facto relationship versus no current marriage-like relationship) and years of education corresponding to the highest level of educational attainment.
Physical health
Physical disability (functional impairment due to poor physical health) was assessed using the physical component summary score from the SF-12. The RAND scoring method [33] was used, with scores below 40 interpreted as an indication of moderate to severe physical impairment.
Financial situation
Three measures of economic circumstances were used. Participants were asked about their ‘main source of income’ and those who identified government pension or benefits were classified as welfare reliant. Employment status was coded as either employed (full or part time) or not employed (including those not participating in the labour-force and those unemployed). Financial hardship was assessed by four items which assessed lack of basic goods and opportunities due to a lack of financial resources (Over the past year have the following happened because you were short of money: pawned or sold something; went without meals, unable to heat home, asked for help from welfare/community organisations). Respondents who reported at least one of these items were classified as experiencing financial hardship.
Burden and role strain
Three questions assessed responsibility for: (i) household tasks, (ii) financial management, and (iii) providing money/household income. Possible response categories were: fully responsible, 75% responsible, 50% responsible, 25% responsible, and not responsible at all. Three binary variables were constructed for each of these items, contrasting those respondents reporting at least 75% responsibility with all others.
Positive social support and conflict
The PATH Survey included six scales measuring positive support (e.g., feeling cared for) from family (range 0–6), friends (0–6) and spouse/partner (0–15) and conflict (e.g., being criticized, having arguments) with family (range 0–9), friends (0–9) and spouse/partner (0–15) [18]. All scale scores were standardized, with a mean of 0 and standard deviation of 1. This analysis used the two friend scales and, as not all respondents had a spouse, we constructed combined scales reflecting the maximum value of the family and spouse/partner standardized scales for positive support and conflict.
Statistical analysis
All analyses were conducted using STATA 10.0. Descriptive statistics were used to contrast the characteristics of those participants providing substantial care with all others. Group differences were assessed by chi-square tests of association, linear regression or negative binomial regression models as appropriate. For subsequent analyses, logistic regression models were used to investigate the association between caregiving and estimates of clinically significant anxiety or depression (considering odds ratios; OR). For analysis of the combined depression and anxiety symptom scale (a count variable), negative binomial regression models were used due to overdispersion, with coefficients transformed to incidence rate ratios (IRR) to facilitate interpretation. After evaluating group differences in the dependent measures, covariates and potential mediators, further analyses considered whether there was a gradient in the effect of caregiving and whether greater severity (indexed by primary caregiver status, duration and time spent caring) was associated with poorer mental health. Analyses also assessed whether the characteristics of caregiving were associated with differences in mental health (i.e., using data from primary caregivers to consider the carer–caree relationship and reason for care).
Baron and Kenny [34] identify three criteria to define mediation: the independent measure (caregiving) is significantly associated with the mediator; the mediator is significantly associated with the dependent measure (mental health); and the effect of the independent measure on the dependent measure (caregiving on mental health) is reduced or eliminated after the mediator is included in a regression model. The analysis plan incorporates these steps. (For similar examples using negative binomial regression models see [35–37].)
A series of models examined whether the different categories of factors described above (financial situation, burden and role strain, and positive social support and conflict) mediated the association between caregiving and mental health. The first model (Model A) included the measure of caregiving status and basic demographic variables as predictors of mental health. This was used as the point of comparison to evaluate subsequent models. Four blocks of variables were each added separately to this base model, and the change in the caregiver OR/IRR and overall change in model fit were assessed. Model B included the measure of physical health, Model C added the three financial variables, Model D included the three measures assessing role strain, and Model E incorporated measures of positive social support and conflict with family/partner and friends. A final model included all the measures simultaneously to identify the variables which were independently associated with mental health symptoms. To assess the extent to which the effect of caregiving on mental health was mediated by the inclusion of these variables, the explained fraction approach was used for ORs and IRRs [(ORa – 1)–(ORb – 1)] / (ORa – 1) [38].
Missing data for most of the variables used in this analysis were minimal. One scale (the SF-12 physical functioning scale) had missing data for 3.1% of respondents and only four other scales had missing data for over 1% of cases. The multiple imputation procedure ICE available in Stata 10.0 was used to impute missing data using the multiple imputation by chained equations procedure [39]. All variables in the models were used in the imputation process, with five data sets generated for analysis.
Results
Demographics
Of the 2,222 survey respondents, 479 (21.6%) identified themselves as a caregiver. This analysis, though, is focused on the 212 respondents (9.5%) who reported that they provided a substantial level of care or assistance to someone with a disability, a medical condition or who was elderly. These 212 caregivers included 128 respondents who identified themselves as a primary carer (5.8% of total sample) and a further 84 who, while not a primary carer, reported providing more than 5 hours of care per week. Data on the duration and time spent caring provides an indication of the intensity of the caregiving role. A total of 80.7% of those providing substantial care had been caring for more than 2 years and 53.1% for more than 5 years. A total of 42% reported that they currently provided more than 15 hours of care per week. More detailed data were available for primary carers and showed that 52.3% were providing care for their spouse, while 91.4% were caring for a family member (spouse, child, grandchild or other relative). The majority of primary caregivers were providing assistance in respect of physical disability or chronic illness (the main reason for 57.8%), while 10.2% reported caring for someone with memory or other cognitive problems, and 13.3% caring for someone with a mental illness.
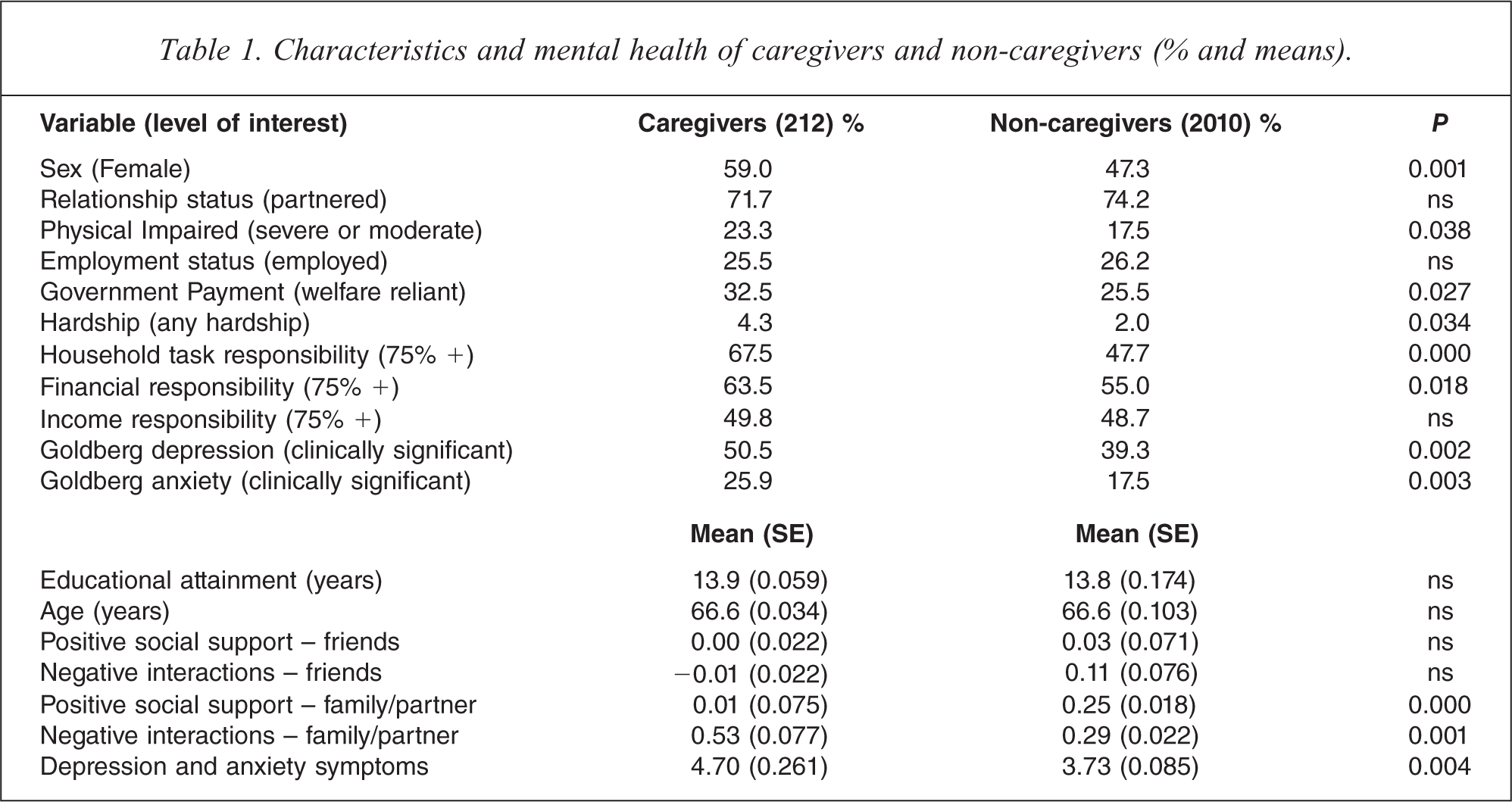
Table 1 presents information on the socio-demographic characteristics of caregivers and non-caregivers. It is apparent that caregivers were more likely to be women, to report physical impairment, to be reliant on welfare payments and have experienced financial hardship, and to report greater responsibility for household tasks and financial management. Caregivers also reported less positive support and more conflict with their family or partner relative to non-caregivers.
Characteristics and mental health of caregivers and non-caregivers (% and means).
Caregiving and mental health
Logistic regression models showed that caregiving was associated with an increased risk of clinically significant anxiety, OR = 1.57, CI.95 = [1.11, 2.20] and depression, OR = 1.52, CI.95 = [1.15, 2.03]. Similarly, the negative binomial regression models showed that caregivers reported a greater rate ratio for depression and anxiety symptoms than non-caregivers, IRR = 1.25, CI.95 = [1.07, 1.46]. A series of logistic and binomial regression models restricted to those who were caregivers investigated whether different aspects of caregiving were associated with mental health (results not presented). There was, however, no evidence that hours of care per week, years in the caregiving role, or primary caregiver status were associated with increased risk of depression, anxiety or overall symptoms. For primary caregivers, mental health was not associated with the nature of the carer–caree relationship or with the main reason that care was required.
Factors that explain the poorer mental health of caregivers
A series of regression models was conducted to investigate whether the association between caregiving and mental health was explained by secondary stressors or mediating factors. The pattern of results was consistent for the two dichotomous measures (anxiety and depression) and for the overall count of depression and anxiety symptoms. Therefore, Table 2 only presents the results from negative binomial models investigating the overall count of depression and anxiety symptoms. The results previously described in Table 1 assess the first criterion of a mediating relationship: the association between caregiving and the potential mediators. Table 2 presents the results of the series of negative binomial regression models from which it is possible to assess the second criterion (the association between the mediators and the mental health outcome) and the third criterion (the significance or size of the mediation effect).
Series of negative binomial regression models (reporting IRRs and standard errors) examining the extent to which the association between caregiving and overall mental health symptom count is mediated by physical health, financial circumstances, role strain, and social support/interactions.
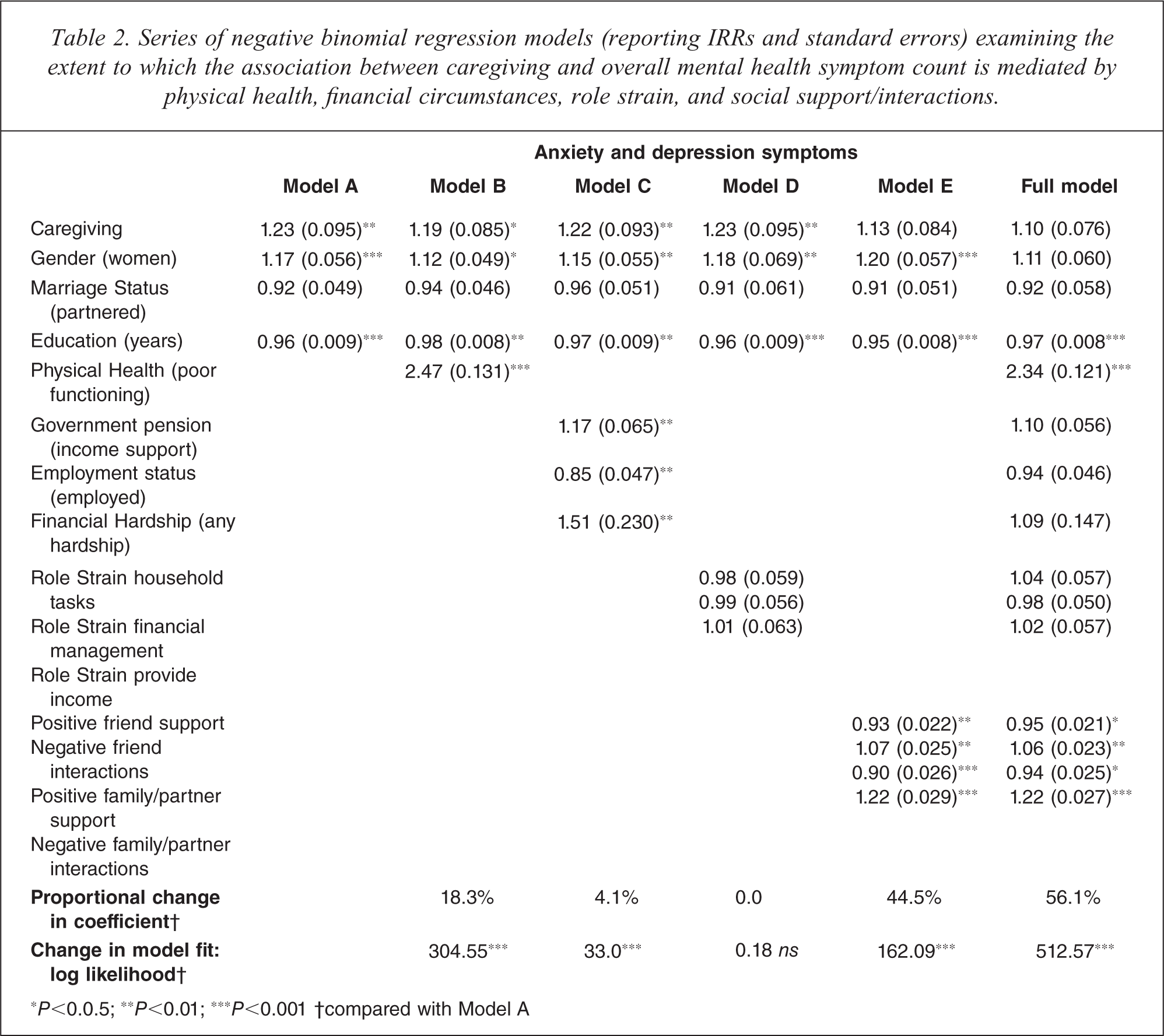
∗P<0.0.5; ∗∗P<0.01; ∗∗∗P<0.001 †compared with Model A
Compared to the univariate results described earlier, the inclusion of the basic demographic variables had little influence on the association between caregiving and depression/anxiety symptoms (IRR reduced from 1.25 to 1.23). Model A showed that caregiving, sex and educational attainment were each independently associated with depression and anxiety symptoms. The IRRs demonstrate that, holding all else constant, being a caregiver, being a woman, and having lower levels of educational attainment are associated with greater mental health symptoms. The inclusion of the binary measure of participants’ physical impairment (Model B) led to the greatest improvement in model fit of any of the steps. Although physical health was significantly associated with depression and anxiety symptoms (IRR = 2.47) and its inclusion improved the overall model fit, physical impairment only explained 18.3% of the effect of caregiver status. All three measures of financial circumstance (welfare receipt, employment, hardship) were significantly associated with mental health symptoms (Model C), meeting the second criterion of mediation. However, the improvement in overall model fit and the reduction in the caregiver IRR for this model was trivial. The results from Model D showed that none of the role strain measures was independently associated with mental health symptoms and that the inclusion of this block of measures did not explain any of the effect of caregiving. In contrast, each of the measures of social support/conflict was significantly associated with mental health and, more importantly, Model E reduced the caregiver IRR by almost 45% and to a level where it was not significant. Lower levels of positive social support from, and higher levels of conflict with, friends and family/spouse were associated with increased rate ratios for depression and anxiety symptoms.
In the final model, the combined effects of physical health, financial circumstances, role strain, social support and conflict explained 56% of the variance associated with caregiving status, and caregiving was no longer a significant independent predictor of mental health symptoms. The results were similar for the other two logistic models (not shown) in which these measures explained 57% of caregiver variance in anxiety and 38% in depression. The significant IRRs in the final model showed that lower levels of educational attainment, physical impairment, low levels of positive social support from friends and from family/spouse and high levels of conflict with friends and with family/spouse were associated with poorer mental health.
Discussion
Summary of findings
The findings of this study were consistent with the previous literature and showed that, compared with non-caregivers and those reporting low levels of caregiving activity, older adults involved in substantial caregiving had poorer mental and physical health, greater financial stress, and reported more conflict and less social support from family and spouse. Their odds of experiencing clinically significant anxiety and depression were over 50% greater than non-caregivers, and they reported 25% more depression and anxiety symptoms. Most critically, however, the test of mediation showed that it was the lack of positive support and greater conflict with family/spouse that explained caregivers’ poorer mental health relative to non-caregivers.
Caregiving, mental health and the PATH Survey
The characteristics of the caregivers in this study were consistent with those in representative Australian surveys. Overall, 9.5% of respondents in the PATH survey were providing a substantial level of care for a friend or relative who needed assistance due to a disability, illness or old-age: 21.6% reported providing any level of care and 5.8% identified themselves as a primary caregiver. The ABS [1] reported that, in the age range 65–74, 20.6% of people were caregivers, while 4.7% were identified as primary carers. The ABS and PATH data were also consistent in terms of sex differences in the prevalence of caregiving (both surveys found 59% of caregivers were women). The Victorian Carers Project [8] found that 5.3% of households included a primary caregiver and, while this reflects the overall population of caregivers, the results are broadly consistent with our age-restricted findings.
The current results showed that, for this group of older caregivers, most were caring for family members, particularly their spouse (see also [1]) and that, on average, the caregiving role was fairly intensive and long-term (see also [10]). The stress-process model of Pearlin and colleagues was used to categorise different sources of caregiver stress and mediating factors. Interestingly, this analysis found no evidence that differences in caregivers’ exposure to primary stressors were associated with different mental health outcomes. In analyses restricted to caregivers, neither duration of caregiving nor hours of care provided per week were associated with differences in mental health. Perhaps more surprising was the finding that care recipient condition was not related to the caregivers’ mental health. While data were collected in relatively broad categories, we expected to find that the burden of care associated with dementia and cognitive decline (memory or other cognitive problems) was greater than other disorders/conditions (e.g., [15,40]). Perhaps the current null finding was a consequence of the general nature of the question which led to the inclusion of a broader range of disorders (e.g., milder memory problems). However, all the respondents to this question had identified themselves as primary caregivers. This finding suggests that, within this community sample of older adults, substantial caregiving has an adverse effect on caregiver mental health regardless of the condition of the care recipient.
Mediation effects
The primary focus of this study was the identification of modifiable factors amenable to a policy response. The stress-process model of Pearlin et al. [27] was used to guide the selection of potentially important secondary stressors and mediating factors. This model suggests that the adverse personal consequences of caregiving may reflect secondary factors such as the impact of caregiving on one's ability to work, increased financial pressures, increased family conflict and role strain, while mediating factors, such as access to social support, can help caregivers to cope with the stressors brought on by the caring role.
Caregivers and non-caregivers did not differ in their reported employment status, income responsibility or reported social support and conflict with friends. Consequently, these factors cannot account for the difference evident between caregivers’ and non-caregivers’ mental health. Caregivers’ poorer mental health compared with non-caregivers was largely explained by their lower levels of positive social support and higher rates of conflict with family and spouse. The importance of social support and family conflict is evident in the literature [10,28–30,41]. Scharlach and colleagues [28] found that the effect of the care recipients’ impairment on caregiver strain was fully mediated by family conflict. Such evidence provides targets for policy and intervention. Mittleman [42] reviewed randomised controlled trials of caregiver interventions and noted that interventions comprising support groups, group counselling and support, and problem solving improved caregiver mental health. Similarly, family centred interventions seeking to improve family functioning, relationship quality and communication, or other strategies to build social support have been identified as effective strategies to assist caregivers [5,28]. Mittleman discussed an intervention (implemented and evaluated) for spouse caregivers based around improving social support and minimizing family conflict that seems directly relevant to our findings. We also note that the importance of family support and conflict could directly reflect the relationship between the caregiver and care recipient as the majority of caregivers in the study were caring for their spouse or another family member. Thus, the measures of family support and conflict could be viewed as a proxy for the quality of relationships with the care recipient [5].
Eastwood and colleagues [19] are amongst those who have reported that a consequence of caregiving is increased responsibility for general household tasks. The current study found evidence of caregivers’ increased responsibility for some household tasks but critically, did not find evidence that this contributed significantly to caregivers’ poorer mental health. The results were similar for the measures of financial circumstance. Poor financial circumstances is one of the most commonly cited factors associated with caregivers’ poor mental health and wellbeing (e.g., [7,10]), but differences in financial circumstances did not explain caregivers’ poorer mental health relative to non-caregivers. We are not suggesting that the adverse financial circumstances of many caregivers should be omitted from policy intervention. This analysis confirmed that caregivers were more likely to be reliant on welfare payments and over twice as likely to experience financial hardship than non-caregivers, and addressing this inequality is a valid policy objective in its own right, regardless of the implications for caregivers’ mental health. However, the current findings suggest that policy efforts to reduce the psychological burden experienced by caregivers require a different focus.
While the focus of the study was on identifying secondary stressors and mediating factors amenable to policy intervention, the analysis also found that caregivers reported poorer physical health than non-caregivers and that this difference contributed to caregivers’ poorer mental health. The stress-process model would consider physical health to be an alternative outcome measure and, therefore, it is not neatly categorised in the current analysis which is focused on mental health as the outcome. Physical health could be conceptualised as a background factor that caregivers bring to the caring situation, or as a secondary stressor that may be exacerbated by their caregiving role. However conceptualised, the strong association between physical and mental health and the poorer physical health reported by caregivers in the current study suggest that physical health is a factor that policy makers need to be mindful of when developing options to support older caregivers.
The present study has a number of limitations. First, the restricted age range means that the results are not generalisable to the overall population of caregivers. However, the circumstances and experiences of caregivers may not be consistent across the life course. There is evidence, for example, that the effect of caregiver status is weaker for older adults [7,10]. Further, different secondary stressors and mediating factors may be salient at different ages. For example, differences in rates of labour-force participation make older caregivers less likely to combine work and caring responsibilities. Thus, the current focus exclusively on older adults ensures the analysis is able to identify policy and intervention targets relevant for older caregivers. Second, the analysis was based on cross-sectional data, limiting conclusions about the causal direction of associations. However, the statistical models were soundly based on theory [27] and appropriate statistical methods were used. Finally, as we analysed data from a community survey with a broad health focus, many factors specific to the caregiving role (such as severity of care-recipient impairment or problem behaviour, ability and confidence to undertake the caregiving role) were not included in the survey. However, as our focus was on identifying secondary stressors and mediating factors potentially amenable to intervention, this need not be considered a major limitation.
In conclusion, caregiving is an important public health issue and likely to take on increasing significance into the future. Efforts to support caregivers should encompass strategies to promote better mental health and wellbeing. The current study represents important progress in policy-relevant Australian research into caregivers’ mental health and the results suggest that interventions focused on promoting positive social support and minimising family conflict will be important aspects of any future policy response.
Footnotes
Acknowledgements
Funding for data collection was provided by by NHMRC Program Grant 179805 and NHMRC Project Grant 157125. Financial support for this project was received from the Australian Government Department of Families, Community Services, and Indigenous Affairs through the Social Policy Research Services Contract. Butterworth, Rodgers and Anstey are funded by NHMRC Fellowships #366781, #148948 and #366756 respectively. Windsor is supported by NHMRC Capacity Building Grant in Population Health Research No. 418020. We wish to thank Helen Christensen, Anthony Jorm, Simon Easteal, Trish Jacomb, Karen Maxwell and the team of PATH interviewers for their contribution to the research.