
Abstract
Despite significant attempts to tackle homelessness, it is still a critical social issue. Family conflict, limited availability of affordable housing and financial pressures exacerbated in the current climate of financial crisis and job loss are recognized causes of homelessness [1]. Mental illness is also associated with homelessness, both as a cause [2] and a reaction to living homeless [3].
The incidence of mental illness in people living homeless far exceeds that of the general population. In a study of 5186 people living homeless in Melbourne, Australia, 30% had mental health problems [4]. A study of 210 people living homeless in inner Sydney also found that 73% of men and 81% of women met criteria for at least one mental disorder in the past year. Psychotic disorders were particularly common, seen in 23% of men and 46% of women [5], far greater than the general population rate of 1% [6]. A lifetime prevalence of a psychotic disorder was also identified in 42% of people living in marginal housing in inner Melbourne [7].
Discussions of causality are highly complex. Symptoms of some psychiatric disorders can cause a person to become homeless. Research in London has found that 25% of severely mentally unwell people supported by mental health services were evicted from permanent accommodation due to disturbed behaviour, or non-payment of rent that was a direct result of their mental illness [8]. Paranoid delusions, bizarre behaviour and neglect of personal or accommodation hygiene, common to acute psychosis, can result in conflict with neighbours, fellow tenants or landlords, directly compromising accommodation stability [2]. Cognitive impairments that are common in schizophrenia, particularly when affecting reasoning abilities, make it difficult to resolve issues of potential conflict, arrange payment of rent or utilities or sustain employment. These cognitive capacities are critical factors in maintaining housing [9].
The experience of living homeless can also contribute to the onset or relapse of mental illness [10]. In the study of homelessness in Melbourne, 50% of homeless people with mental illness became mentally unwell only after becoming homeless [4]. Living on the streets or in crisis accommodation is associated with high levels of social instability (e.g., not knowing where to sleep that night or find the next meal) and potential for violence or theft [3,11]. This traumatizing environment is even more damaging when combined with significant alcohol or other drug abuse (common in people living homeless [12]), and can trigger or exacerbate mental illness [13].
People living homeless are significantly less likely to engage with formal outpatient mental health services [14] and have lower rates of psychotropic medication use [15], but higher rates of emergency health service usage [16]. This means they need a different approach to providing mental health care. Assertive outreach models have the strongest evidence for successfully supporting people living homeless with a mental illness [17]. Assertive outreach involves mental health workers spending time at locations frequented by people living homeless such as soup kitchens or crisis accommodation services [18–20]. This enables them to work with welfare staff onsite to gradually build a therapeutic relationship with people attending who are mentally unwell, to provide direct support and transition them into more ongoing care.
The integrated homeless mental health initiative in Melbourne's Inner South
Beginning in 2006, the Victorian Department of Human Services funded an initiative that extended the assertive outreach model to embed mental health clinicians into the daily operations of two welfare agencies in Melbourne's inner south locality. The organizations involved were Sacred Heart Mission (SHM) and Hanover Welfare Services (Hanover). Both organizations provide accommodation, drop-in, health facilities and other welfare support for people living homeless. The Alfred Homeless Outreach Psychiatric Service (HOPS) who specialize in supporting people who are homeless and difficult to engage, offered direct mental health support to consumers and consultation to welfare staff.
As outlined in Figure 1, mental health care delivery onsite at both welfare services was achieved through two mechanisms. HOPS was funded to establish a dedicated onsite presence at three SHM locations (Central: a drop-in meals and resource centre; Homefront: a women's crisis accommodation service; Women's House: a women only resource centre) and Hanover's crisis accommodation facility, and were also responsive to requests for support. HOPS also provided formal education sessions on topics such as mental state assessment, medication effects, aggression management, and informal mental health consultation to welfare case management staff. Funding was also provided to Hanover and SHM to employ a mental health worker to liaise with HOPS, and provide full time, onsite consumer support and consultation to colleagues. The model of care was underpinned by the following principles:
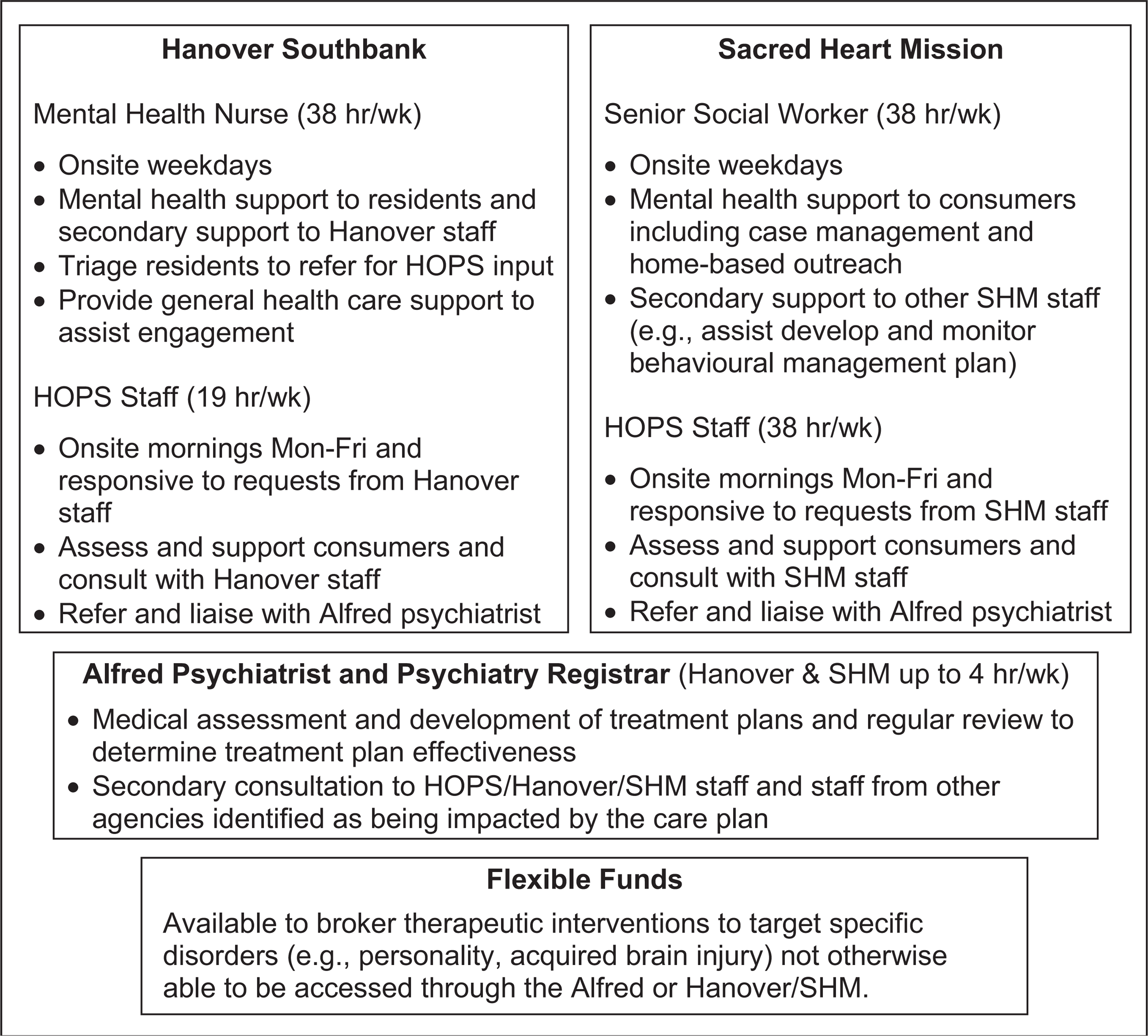
Representation of the model of care for the Integrated Homeless Mental Health Initiative.
(i) relationship building with consumers through assertive engagement;
(ii) comprehensive assessment of the consumer onsite and development of a care plan that systematically addressed their multiple presenting issues;
(iii) ongoing review and monitoring of care plans in partnership with consumers;
(iv) outreach support to maintain ongoing engagement to prevent crisis trajectory;
(v) a multidisciplinary care-team approach involving staff from relevant services.
The current report summarizes the methodology and findings from an evaluation of the initiative. In particular, it was expected that the initiative would result in improved identification, engagement and provision of support to people who are homeless with a mental illness. Improved collaboration between services would also be facilitated to enhance accommodation and mental health outcomes for consumers.
Methods
We evaluated the initiative over the first 2 years of operation and focused on three areas: (i) auditing consumer clinical service usage, gathering accommodation information and monitoring changes to the rate of inter-service referrals; (ii) gathering questionnaire data and interview feedback information from consumers who had contact with the initiative; and (iii) gathering questionnaire and focus group information from staff of all services who had contact with the initiative. Most of our focus for the evaluation was on audits of the consumer and service outcomes. The evaluation methodology was approved by The Alfred and Hanover Research Ethics Committees and all participants gave written, informed consent prior to entering the study.
Consumer audit
The consumer audit recorded details for all people identified from The Alfred Community Psychiatry intake database and the consumer databases of Hanover and SHM. Additional information was audited from individual consumer files. For each consumer the following was recorded: demographics; reason for and outcome of referral to the initiative; accommodation at referral; previous psychiatric diagnosis; the number of inpatient psychiatry admissions in the 12-month period prior to referral; presentations to Alfred Emergency and Trauma Centre in the past 12 months; and documented substance misuse at referral.
For people receiving active case management or short-term support from Alfred Psychiatry staff the following was also audited: length of engagement, and accommodation at 6 months post initial referral or discharge from Alfred Psychiatry support.
Service integration audit
As well as characterizing the nature and outcome of people having had contact with the initiative, the impact on service integration was also explored focusing on:
(i) changes to the rate of admissions of consumers from Hanover or SHM to the Alfred Inpatient Psychiatry Unit before (2005) and after (2006, 2007) the initiative commenced, audited from a review of Inpatient Psychiatry Discharge Summaries;
(ii) differences in inpatient psychiatry length of stay (LOS) for consumers admitted from Hanover and SHM compared to the overall Alfred Psychiatry LOS;
(iii) changes in the rate of contacts from staff and consumers of Hanover and SHM to Alfred Crisis Assessment and Treatment Service (CATS), audited from a review of all documented contacts received by Alfred CATS.
Analysis
Details relating to consumer's demographics, clinical presentation and service use are displayed as frequency (e.g., percentage of overall population) or mean (e.g., age in years) values. The Chi-square test of independence was used to compare changes in frequency data with analysis of variance used to explore differences in mean values. A single-sample t-test was used to compare the inpatient LOS for consumers of Hanover or SHM with the overall Alfred Inpatient Psychiatry LOS.
Results
Consumer demographics, clinical presentation and service usage
Across all three sites in 2006–2007 approximately 417 consumers were referred between mental health and welfare staff (Table 1). Additional consumers were supported solely by the SHM social worker (76 people were case managed over 2006–2007) and the Hanover mental health nurse (there were 27.2 average weekly contacts in 2006–2007 which were for mental health issues and triaging for a GP clinic). The age of consumers was significantly younger at Hanover, F(2,188) = 10.12, p < 0.0005, although an age range of 17–75 years was supported across all sites. Highlighting the transience of this population, over 8% were documented to have arrived from interstate in the past 2 months, in many cases to avoid community mental health treatment. Through being engaged by this initiative, some continued to receive support if staying in Melbourne, while others were provided therapy to stabilize their mental state and guidance in returning to their home state to re-connect with family or their previous mental health service. Most consumers had previous psychiatric diagnoses, with a psychotic or affective disorder (in particular bipolar or major depression) most common, personality and alcohol and other drug use (AOD) disorders also common with almost 52% experiencing current AOD misuse. For a number of people, the initiative facilitated their first engagement with a mental health service. The psychiatric history was unknown for a small proportion who either left the welfare service prior to completion of assessment or refused assessment. Transience and reluctance to engage with mental health practitioners were therefore still barriers to engaging with some in this population.
Consumer demographics and service usage at referral for mental health support
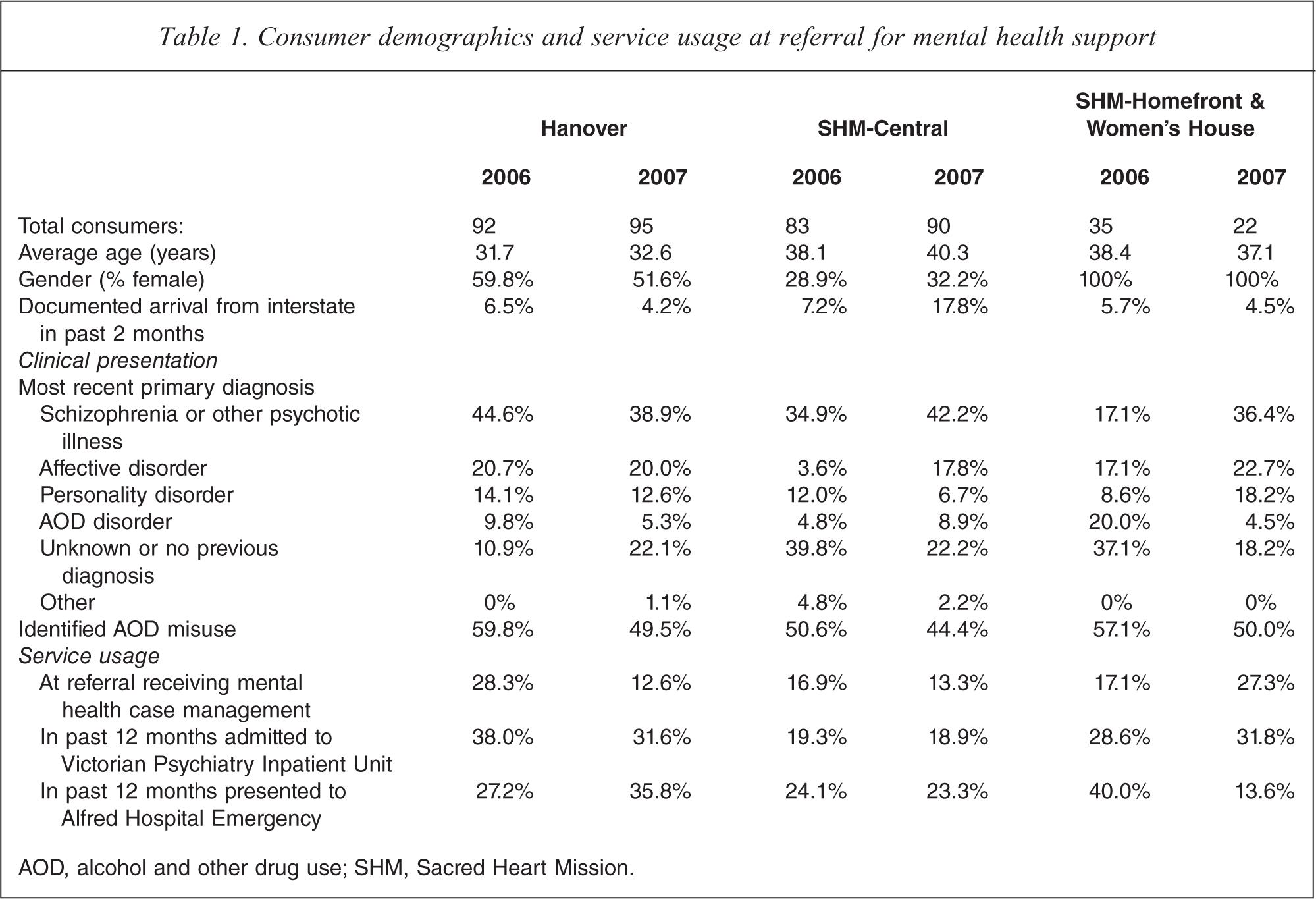
AOD, alcohol and other drug use; SHM, Sacred Heart Mission.
At time of referral for mental health support, relatively few (18%) were engaged in community mental health case management. This was despite a much higher proportion presenting to an emergency department (28% had recently presented at least once to The Alfred emergency) or requiring inpatient psychiatry care (28% had recently been admitted to a Victorian psychiatry inpatient unit) in the previous 12 months.
Outcomes for consumers referred through this initiative
Most consumers were managed solely through secondary consultation from HOPS to welfare staff (Figure 2). However, as there was a significant increase in the proportion of consumers solely supported through secondary consultation from 2006 (30%) to 2007 (46%), χ2(1) = 11.19, p = 0.001, this suggested an improved capacity of Hanover and SHM staff to manage people experiencing mental illness. Following completion of assessment, a number of consumers were referred for ongoing support from a GP or AOD service, with over 31% either actively supported by HOPS or admitted to the Alfred Inpatient Unit.
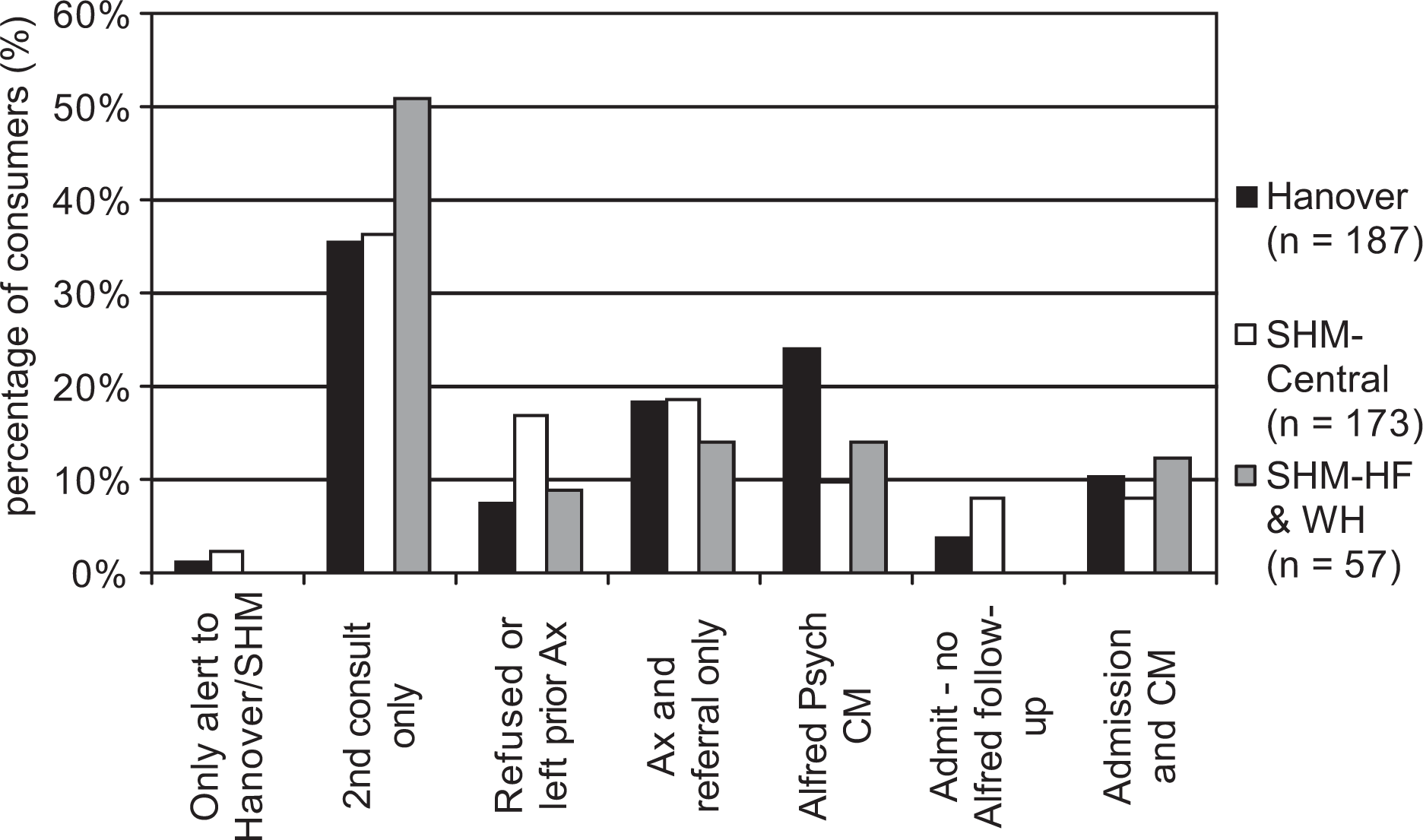
Combined 2006–2007 outcomes for referrals between welfare and mental health staff.
Highlighting some success in engaging this population in ongoing mental health care, Figure 3 shows the length of engagement for consumers receiving active support from Alfred Psychiatry staff. While the majority received short-term support lasting either less than 1 week or 1 month, almost 13% were still engaged in active case management or had been case managed for over 12 months.
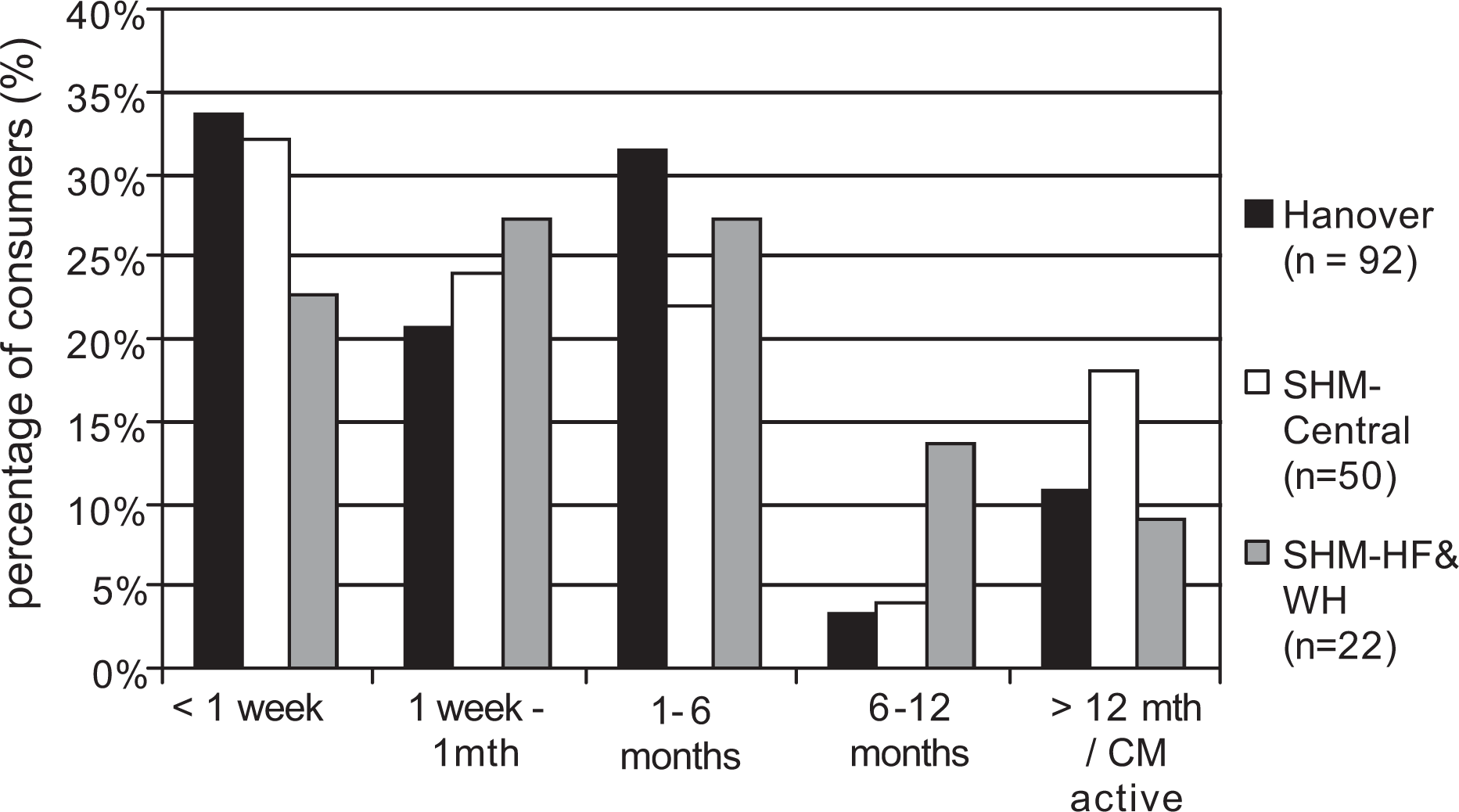
Combined 2006–2007 length of engagement for consumers directly supported by Alfred Psychiatry staff.
For consumers sustained in case management for at least 1 month, improved stability of accommodation was generally achieved (Figure 4). At referral, most consumers were either completely homeless or living in crisis or temporary accommodation. In contrast, at follow up, accommodation was more stable for most consumers.
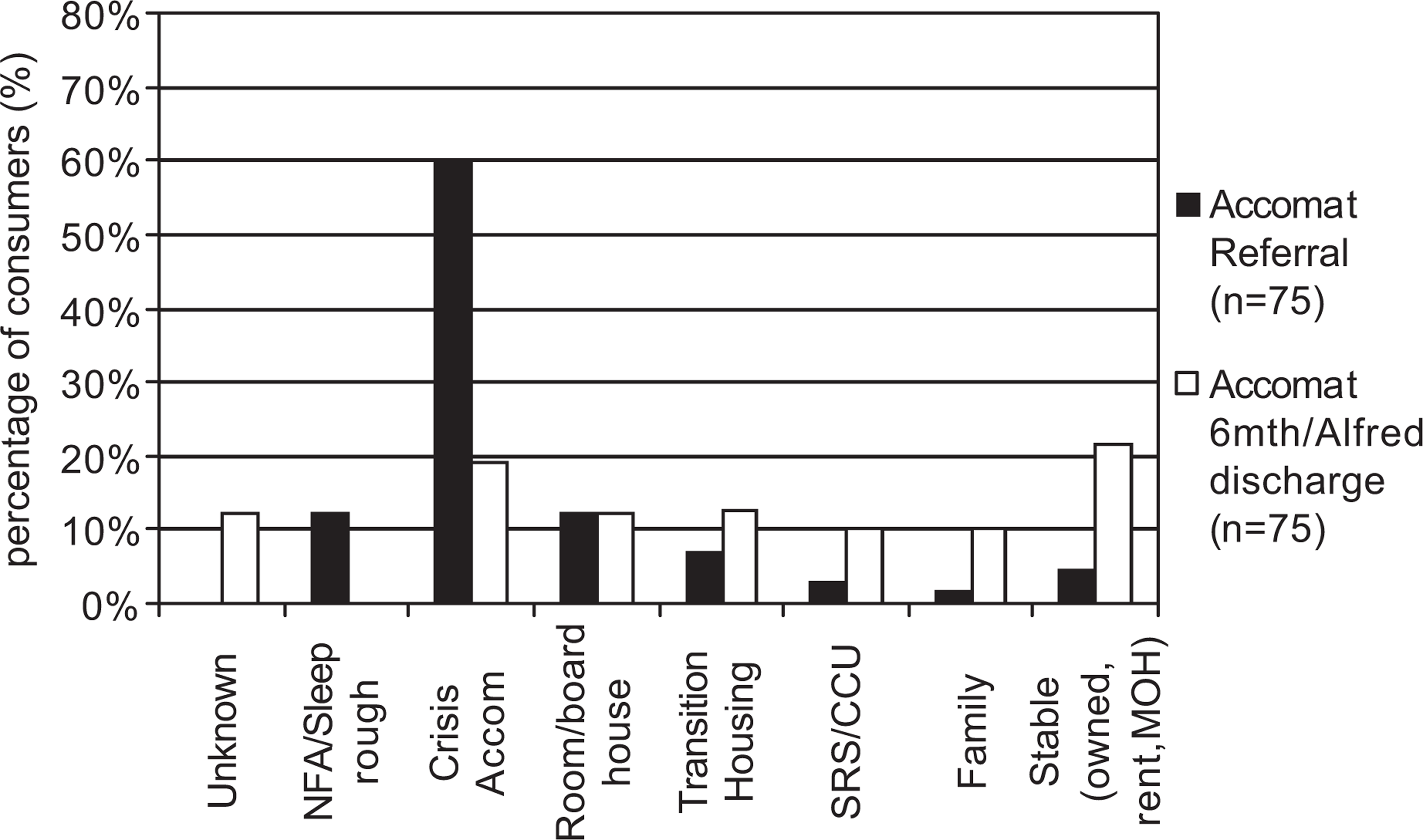
Accommodation at referral and 6 months follow up or discharge for consumers (combining 2006–2007) engaged by Alfred Psychiatry (and in most cases concurrently with welfare service staff) for at least 1 month.
Service outcomes
Service utilization was also impacted by the initiative, with significant differences (Figure 5) in the frequency of admissions to Alfred Psychiatry Inpatient Unit from each welfare service before and after commencing the initiative, χ2(4) = 12.53, p = 0.01. From Hanover the admission rate was halved, while from SHM-Central there was a threefold increase. With only four people admitted from SHM-Central in 2005, despite approximately 300 people attending daily, this suggested that the initiative enabled a greater number of people needing intensive psychiatric care to be identified. Consumers admitted from the welfare services required significantly longer inpatient hospitalization than was the average for The Alfred Psychiatry Inpatient Unit during 2005–2007, t(93) = 2.34, p = 0.02. While the average Alfred Psychiatry Inpatient LOS for 2005–2007 was 15.2 days (3249 admissions), the average LOS for consumers admitted from Hanover was 18.3 days, SHM-Central 25.0 days, and SHM-Homefront and Women's House 23.9 days. As well as homeless consumers being more acutely unwell, finding suitable discharge accommodation was also more difficult, delaying LOS further.
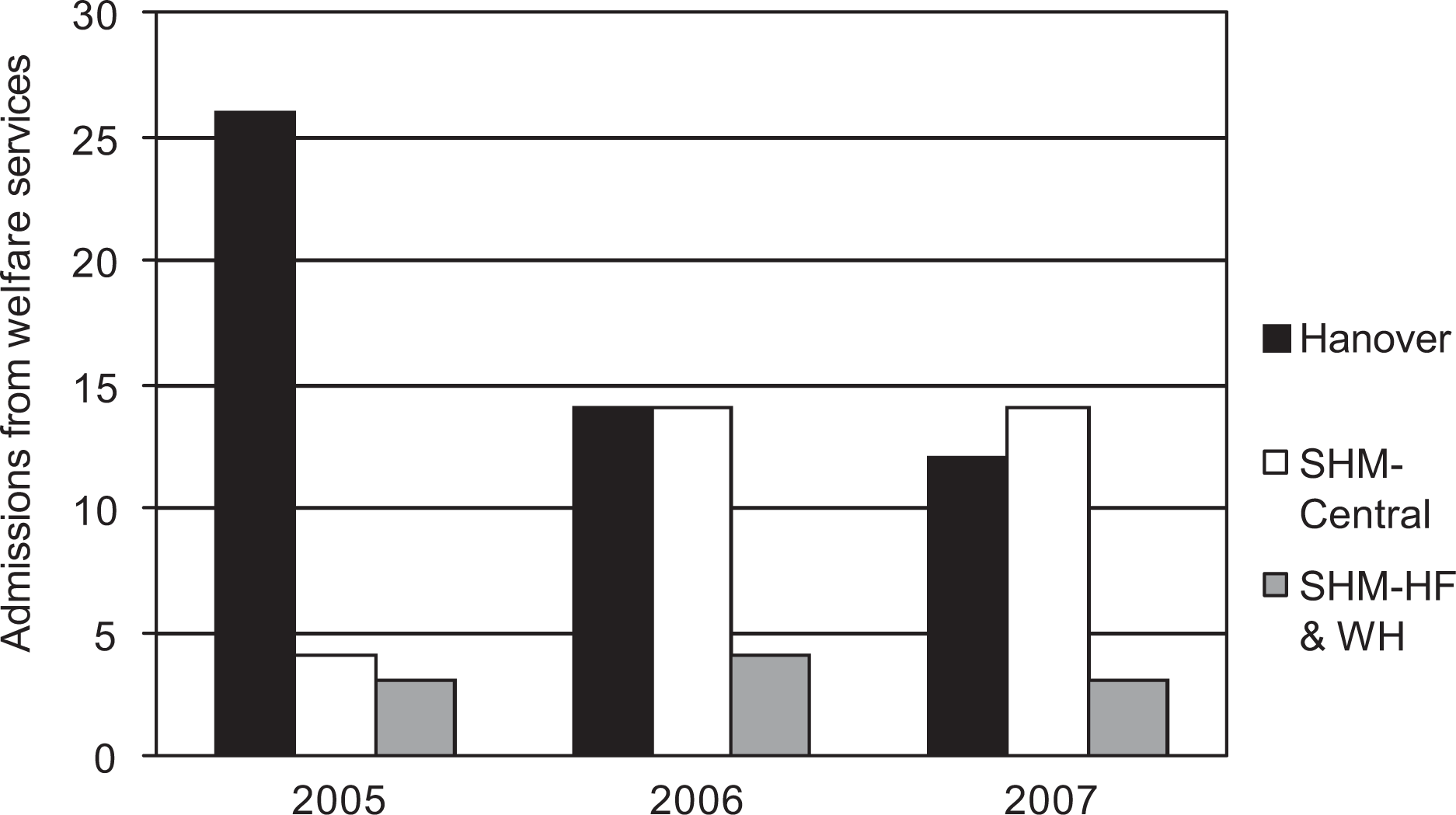
Consumers admitted to Alfred Inpatient Unit from Hanover Welfare Services or Sacred Heart Mission before (2005) or after (2006, 2007) the initiative commenced.
A final analysis explored the impact of the initiative on requests for a crisis mental health response from the Alfred Crisis Assessment and Treatment Service (CATS). A Chi-squared test of goodness of fit found a significant reduction in contacts from staff and consumers of Hanover and SHM to Alfred CATS after the initiative commenced, χ2(2) = 13.24 p = 0.001 (Figure 6).
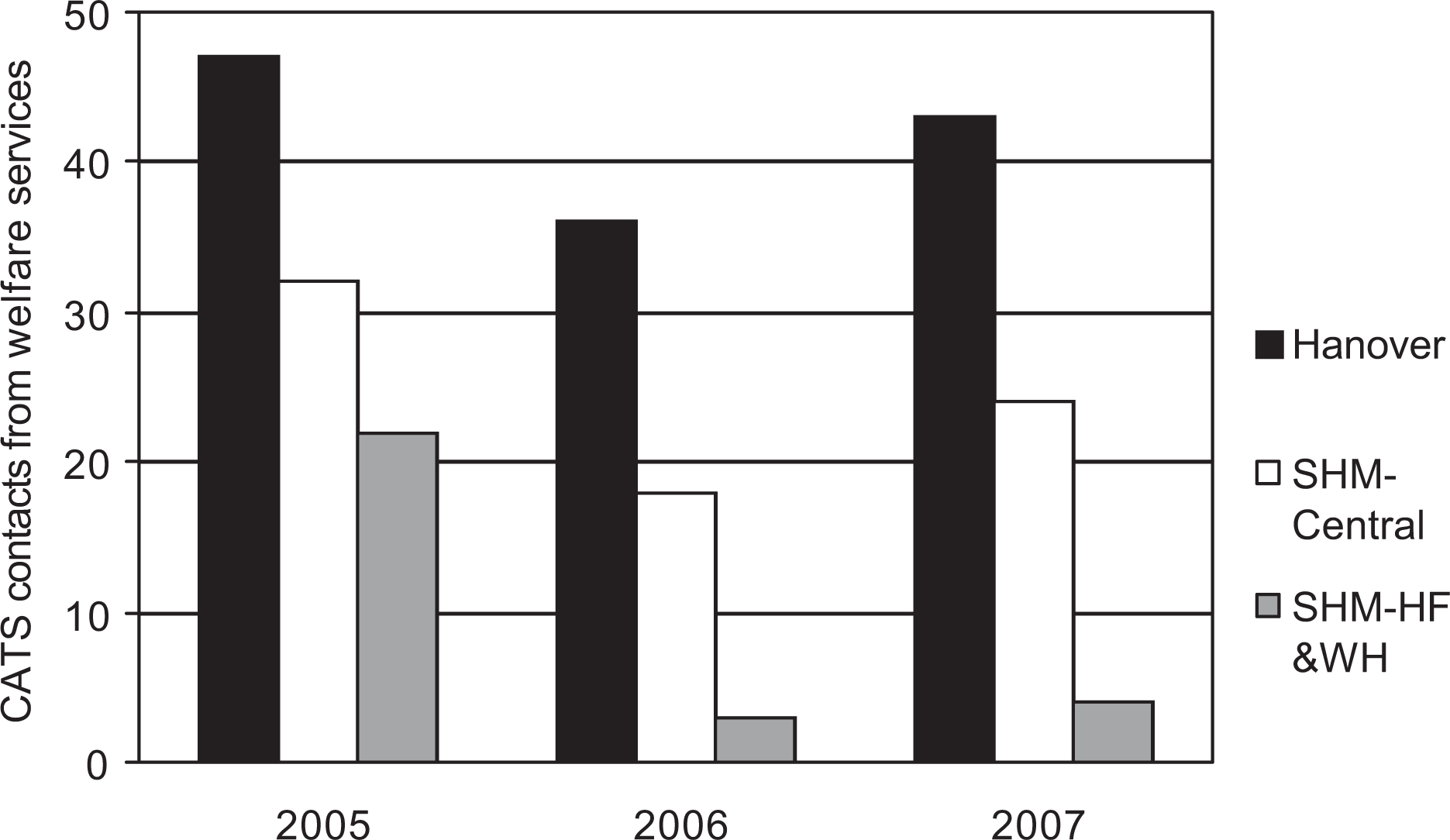
Contacts to the Alfred Crisis Assessment and Treatment Service from staff or consumers of Hanover Welfare Services or Sacred Heart Mission before (2005) and after (2006, 2007) the initiative commenced.
Discussion
Living homeless with a mental illness profoundly impacts on physical, psychological and social wellbeing, and worsens the potential to find and sustain stable accommodation [2]. This is a population that is often difficult to engage in community mental health care [14], something confirmed in this evaluation by the low levels of mental health service engagement at referral for mental health support, despite high levels of emergency health and psychiatric service usage. Our evaluation detailed the impact of a Department of Human Services funded initiative in Melbourne's inner south, aimed at embedding mental health staff into the daily operations of two welfare services offering a range of supports to people living homeless. The initiative enabled co-located mental health and welfare staff to work together to holistically identify and address consumers’ often complex needs. An important aim of the initiative was also to empower consumers to contribute to determining the targets for intervention and where and how this was delivered, thereby improving treatment adherence and ultimately recovery [21,22].
The evaluation demonstrated that this initiative, although supported by relatively minimal funding (the equivalent of four full-time positions across three services), produced significant benefits for people living homeless with a mental illness as well as staff from involved services. From 2006 to 2007 there was a significant increase in the number of consumers with a mental illness supported by welfare staff with only secondary consultation from Alfred HOPS. This suggested that welfare staff had developed an increased capacity to manage people living homeless with a mental illness. A number of homeless consumers were also successfully engaged in mental health care, with many maintained in case management for over 12 months. We found that if people received active case management for at least 1 month (often involving collaborative support between Alfred HOPS and welfare staff), they could in general achieve greater accommodation stability. This highlighted the importance of collaborative care delivery [23].
Outcomes for the collaborating services were equally positive. Co-locating mental health and welfare staff allowed earlier and more effective intervention for people experiencing mental illness. This had a differing effect on the admission rates from Hanover and SHM. At Hanover, consumers were generally younger and in many cases had a shorter and less chronic history of mental illness. Co-location of mental health and welfare staff at Hanover enhanced their capacity to work with many to prevent symptom escalation and subsequent psychiatric admission. The onsite presence of mental health staff at Hanover also prompted an increase in 2006 in the number of consumers discharged directly from the Alfred Psychiatry Inpatient Unit to the crisis accommodation facility of Hanover. This enabled Alfred HOPS staff to continue providing mental health outreach support to consumers discharged to Hanover, improving continuity of care.
From SHM-Central there was a marked increase in psychiatric admissions during the initiative. However, given the very high LOS for consumers admitted from SHM, this suggested that prior to the initiative a number of very unwell people were not receiving appropriate mental health care. For these people, locating mental health staff onsite who worked closely with staff of the meals and resource drop-in, improved identification and provision of care, consistent with previous assertive outreach models [18,19]. Post-discharge from hospital, a number of these consumers continued to access the meals, resource or accommodation services of SHM. Alfred HOPS staff were therefore able to monitor their progress during admission and work with SHM staff to establish a collaborative post-discharge care plan, again enhancing continuity of care.
The extent to which this initiative built on existing assertive outreach approaches is highlighted when contrasted with previous Australian and international assertive outreach models. Since 1994, a homeless outreach psychiatric service has operated in Melbourne's inner west [18]. Assertive outreach to engage individuals in their environment and collaborating with and providing educational support to staff from generic homeless services to enhance care delivery for homeless mentally ill consumers were core principles, similar to our initiative. The approach of having mobile psychiatric outreach teams with the dual foci of supporting people living homeless with a mental illness and the welfare agencies that support them has also been effective in improving the flexibility of care delivery, satisfaction with care and networking capacity of staff from different agencies in London [24] and Ottawa [19]. Despite even intensive assertive outreach, however, the experience of Melbourne's inner west homeless outreach service was that in 2005, 23% of engaged consumers still experienced long-term homelessness [25].
Barriers to the effectiveness of assertive outreach models have been identified including limitations on the availability and expertise of mobile mental health staff [19] and the availability of suitable long-term accommodation [25]. Assertive outreach that relies on mental health clinicians being called to respond to an identified mentally ill consumer or being onsite when a consumer requires assessment, can result in the response being delayed or unwell consumers missed if they leave before the clinician arrives. The current initiative sought to overcome these barriers through co-location of workers for daily dedicated times when welfare service consumers and staff knew that Alfred HOPS staff would be onsite. Employment of a full-time mental health clinician by each welfare service also expanded the availability of onsite mental health support. Welfare staff also commented that co-location established ‘mental health care’ as part of core business for their service. This encouraged them to seek advice from, and work collaboratively with, onsite mental health clinicians. Providing support outside normal business hours was, however, an ongoing challenge. The evaluation found that the reduction in requests for crisis support from The Alfred CATS was greater for SHM which mostly operates during business hours. Hanover as a crisis accommodation service operates 24 hours a day and many requests for crisis mental health support were received at night or on weekends when Alfred HOPS were not operating. Increased availability of mental health staff to ensure coverage during risk periods outside business hours would have strengthened the initiative.
Combining housing and assertive outreach programs have also been shown to produce better outcomes than assertive outreach alone [26]. Even for consumers with a chronic psychiatric history, combining outreach support and long-term accommodation can improve social, health and housing outcomes [22,27]. The provision of suitable housing can minimize the adverse physical and psychological effects and social disconnectedness forced by homelessness [28,29]. Stable accommodation can also facilitate a sense of ownership and motivation to pursue goals such as working or training, which are not able to be considered during the highly stressful experience of being homeless [21]. Co-location of mental health and welfare staff in this initiative offered more time and opportunities to share knowledge about accommodation resources, increasing the likelihood of finding suitable accommodation for consumers. The capacity to advocate for entry to suitable accommodation was also strengthened by joint input from welfare and mental health staff and the knowledge that ongoing and joint support would be provided where appropriate. The ongoing challenge, however, has been that Melbourne has had a reduction in available affordable housing increasing the difficulty of finding stable accommodation for mental health consumers [4]. A key component of the Commonwealth of Australian Government's response to homelessness is increased supply of specialist accommodation models that integrate with initiatives such as ours to offer permanency as well as coordinated psychosocial and other health support [30]. Greater availability of accommodation facilities in our region that foster independence while retaining links with family, service agencies and the broader community will be critical to enhancing our capacity to support people living homeless with a mental illness.
Conclusion
Mental health workers were embedded into the daily workings of two welfare services providing accommodation, meal and other support to people living homeless, as an important strategy to improve the identification and provision of treatment for people living homeless with a mental illness. The co-location of staff from a Melbourne mental health service (Alfred HOPS) and two welfare services (Hanover and SHM), greatly improved the provision of mental health care for a very difficult to engage and often acutely unwell population. This model of integrated welfare and mental health care is a relatively inexpensive intervention that can provide substantial improvement in the quality of life and functioning of people living homeless with a mental illness.
Footnotes
Acknowledgements
We would like to thank consumers and staff from The Alfred, Sacred Heart Mission and Hanover Welfare Services who helped in coordinating or completing the evaluation of this initiative. Staff from the Consumer Action Research Group also facilitated completion of interviews with consumers. Special thanks is also given to Australian Rotary Health for the funding of this mental health service evaluation.