
Abstract
Atypical antipsychotic medications (such as olanzapine, risperidone, quetiapine amisulpride, aripiprazole, ziprasi done and clozapine) have been approved in Australia to treat schizophrenia and, in some cases, bipolar disorder (olanzapine, risperidone, quetiapine, ziprasi-done). The use of these medications substantially increased in Australia between 1995 and 2001, with olanzapine the most commonly used [1,2]. Since 2002 olanzapine has been ranked fifth or sixth on the Pharmaceutical Benefits Scheme (PBS) list of subsidized drugs by cost to government. In 2006–2007 the cost to the PBS (excluding State-funded inpatient hospital use) was AUD$158m and the cost of risperidone was AUD$81m [3].
In Australia, the atypical antipsychotics are listed on the publicly subsidized PBS with an Authority Required listing. In order to be subsidized a drug must be approved by the regulatory authority, the Therapeutic Goods Administration (TGA), and recommended as cost-effective by the Pharmaceutical Benefits Advisory Committee (PBAC) for a specific indication. During the period of data collection, a prescriber had to obtain government approval by phone before prescribing these drugs for only the PBAC-approved indications. It is possible that some of these drugs were also prescribed for indications that were neither approved by the TGA nor subsidized by the PBS [4]. Olanzapine, for example, is listed on the PBS only for the treatment of schizophrenia and maintenance treatment for bipolar I disorder [5]. Nonetheless, olanzapine has been used (off-label) to manage behavioural disturbances in the elderly with dementia (among other conditions) [6]. Unlike risperidone, olanzapine is not currently registered for use in Australia for this indication, although there is evidence to support this use [7].
Risperidone was the first atypical antipsychotic listed on the PBS in February 1995 for the treatment of schizophrenia. It was followed by olanzapine in August 1997 and quetiapine in November 2000. Risperidone was subsidized as an adjunctive to mood stabilizers for mania associated with bipolar I disorder in February 1995. In April 2005 risperidone was also listed for the treatment of behavioural disturbances in dementia, and olanzapine was listed for maintenance treatment of bipolar I disorder. With typical antipsychotics, authority was required for both thioridazine (schizophrenia) and tetrabenazine (hyperkinetic extrapyramidal disorders) during the study period. Recommendations for listing these drugs for other indications on the Repatriation PBS (RPBS for Veteran concession card holders) were not considered.
The aim of the present study was to examine trends in prescribing of subsidized antipsychotic drugs in the Australian population from 2002 to 2007 by gender and age, and to examine gender differences in indications for use. Data on the gender and age of persons receiving a prescription were available from 2002, when entry of each patient's Medicare number enabled a check of details by Medicare Australia.
Methods
The data on the number of prescriptions for atypical and typical antipsychotic medications were obtained from the Department of Health and Ageing. These data comprised all PBS and RPBS prescriptions dispensed in Australia between July 2002 and June 2007. De-identified data included details of the drug product dispensed and information on the patient's gender and age. The majority of prescriptions (92%) dispensed in the Australian community (including residential care) are subsidized through the PBS and RPBS. Data on gender and age are collected by Medicare Australia for 87% of all community prescriptions of antipsychotics and 95% of atypical antipsychotics [8].
The amount of drug dispensed and supplied was standardized using the defined daily dose per 1000 population of each age group per day (DDD 1000 population−1 per day). The defined daily dose (as defined by the World Health Organization Collaborating Centre for Drug Statistics Methodology) corresponds to an estimated mean daily dose used for a medication's principal indication in adults [9]. It is useful for comparing drug use across different countries, patient groups and different formulations. The sample group used in the calculations corresponded to the number of Australians in each gender and 5 year age group [10].
The drugs included those with an anatomical therapeutic chemical code starting with N05A (indicating antipsychotics) listed on the PBS during the study period. These were (in alphabetical order): amisulpride, chloropromazine, flupenthixol, fluphenazine decanoate, haloperidol, lithium, olanzapine, pericyazine, prochlorperazine, quetiapine, risperidone, tetrabenazine, thioridazine, trifluoperazine and zuclopenthixol [9]. Aripiprazole was listed on the PBS in May 2004 but there were insufficient data for analysis. Utilization was calculated for three categories of prescribers: general practitioners (GPs), psychiatrists and other specialists (including geriatricians). The code assigned to each provider represents the specialty for which the bulk of services are provided. The gender/age and prescriber analyses do not include prescriptions that cost less than the general co-payment. All calculations were completed using Microsoft Office Excel 2003.
Results
Olanzapine was the most commonly prescribed medication, followed by risperidone and quetiapine (Table 1). There was considerable use of the older typical antipsychotics, haloperidol and lithium, in those aged ≥60 years. There was greater use of both atypical and typical antipsychotics in women than men aged ≥60 years. Conversely, there was greater use of both classes of antipsychotics in men than women aged 20–59 years. Lithium was used primarily as a mood stabilizer in bipolar disorder and adjunctively for psychotic illnesses. Prochlorperazine is used mainly as an anti-emetic. Use of both drugs remained stable over the study period (data not shown).
Drug utilization (DDD per 1000 population per day) for drugs listed on the PBS in the 2006–2007 financial year
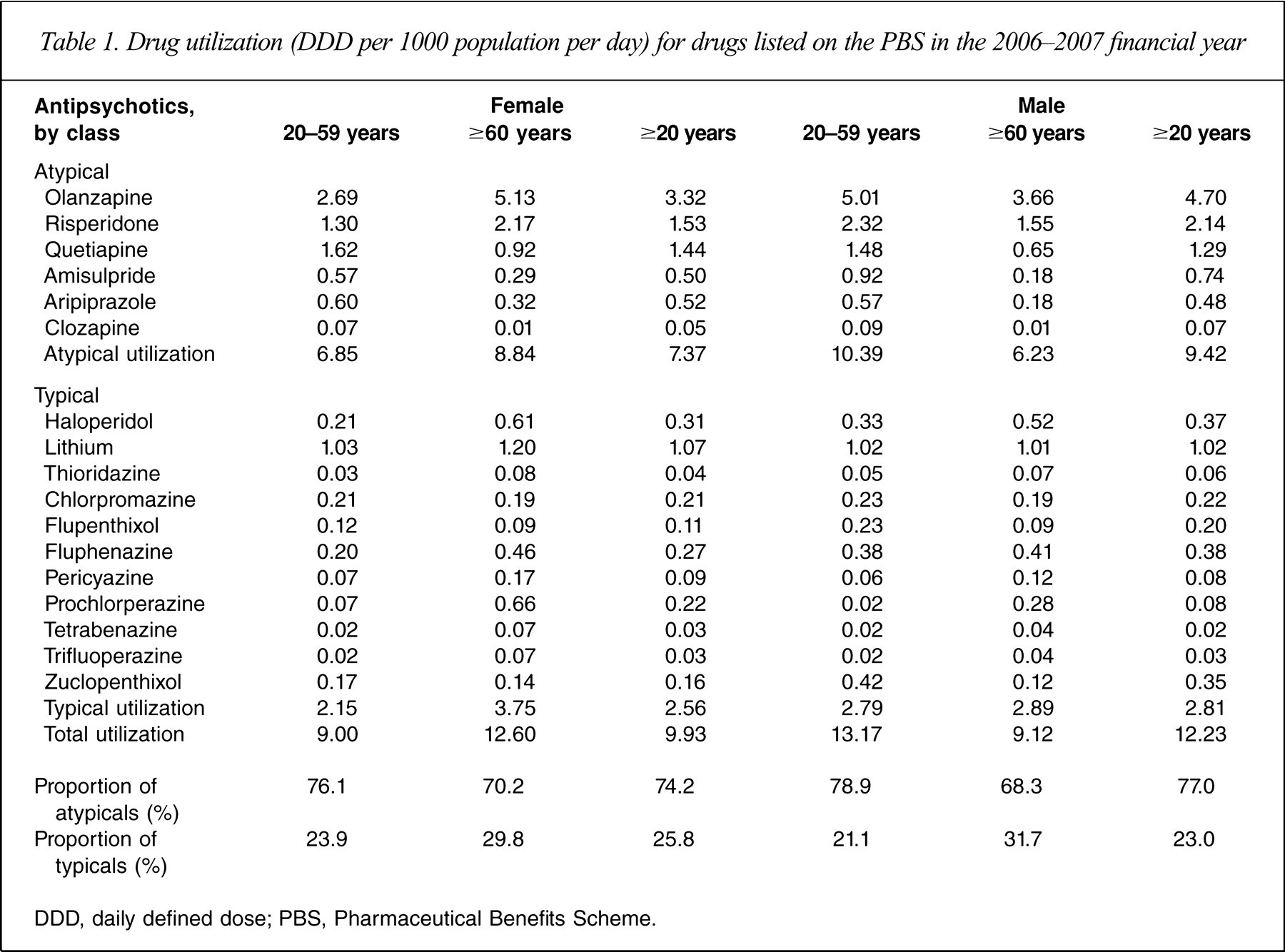
DDD, daily defined dose; PBS, Pharmaceutical Benefits Scheme.
Olanzapine use had only a small increase over the study period compared to risperidone and quetiapine, both of which increased (Figure 1). Amisulpride and aripiprazole increased to a steady approximately 0.5 DDD per 1000 population per day. Risperidone was subsidized for dementia and an injectable form of risperidone was introduced in 2005: utilization increased to 0.58 DDD per 1000 population per day by June 2007. Haloperidol use decreased slightly (approx. 0.2 DDD per 1000 population per day) over the period. The higher level of utilization towards the end of each calendar year reflects the safety net provisions introduced into the PBS in 1986. These ensure that patients with multiple medical conditions are not financially prevented from obtaining them [8].
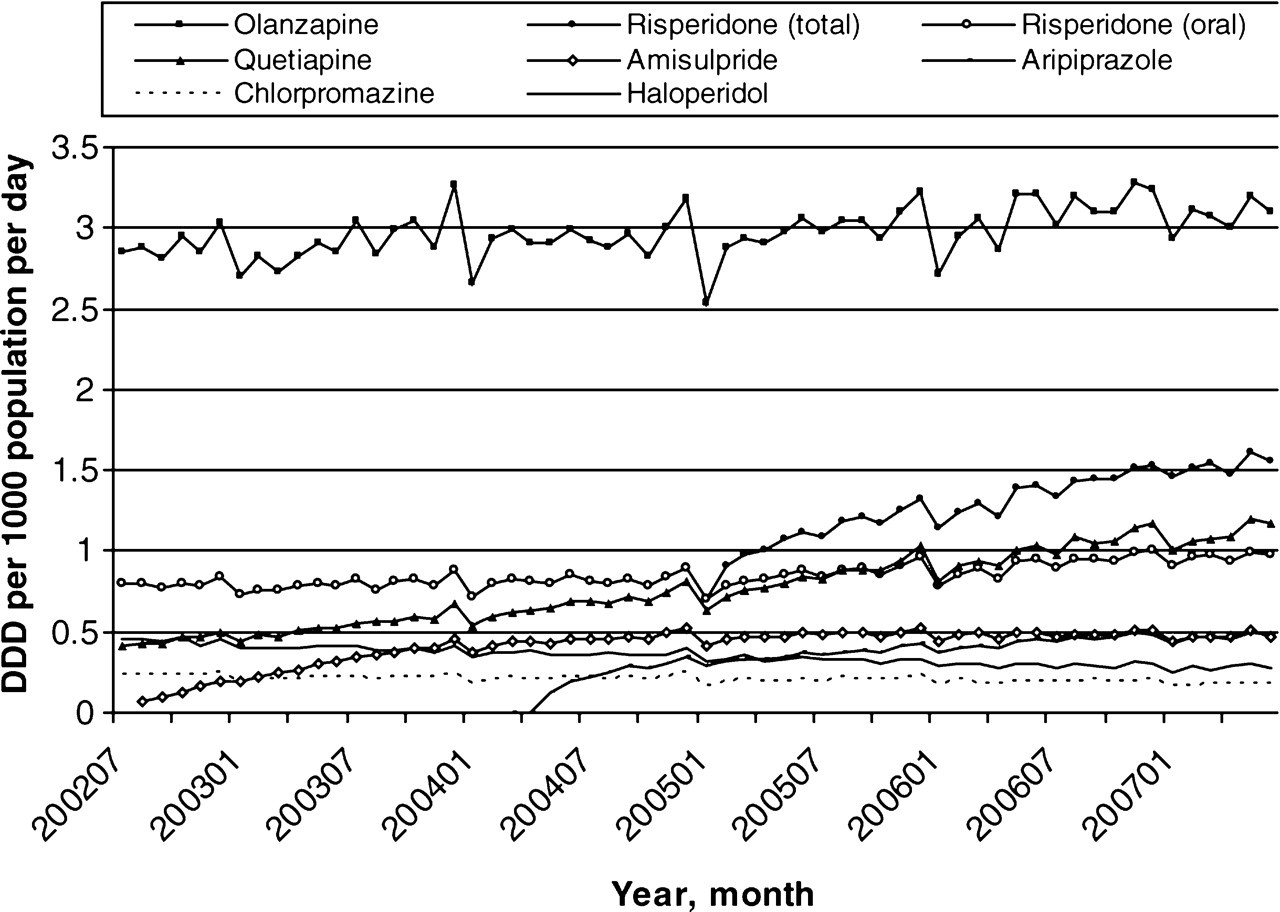
Trends in selected antipsychotic drug utilization (defined daily dose (DDD) per 1000 population per day) 2002–2007 (risperidone is shown for both total and oral only use).
There were large gender differences in the use of olanzapine across the lifespan (Figure 2). In men, peak use was in the 25–55 year age group and there was a smaller peak in men aged ≥90 years. In the younger age groups, the use of olanzapine in women was half that in men (30–34 years, female: male=0.45); in the older ages, in contrast, female use was double that of men (95–99 years, female: male=2.07). Thus the use of olanzapine was concentrated in the older age groups for women and in the younger age groups for men.
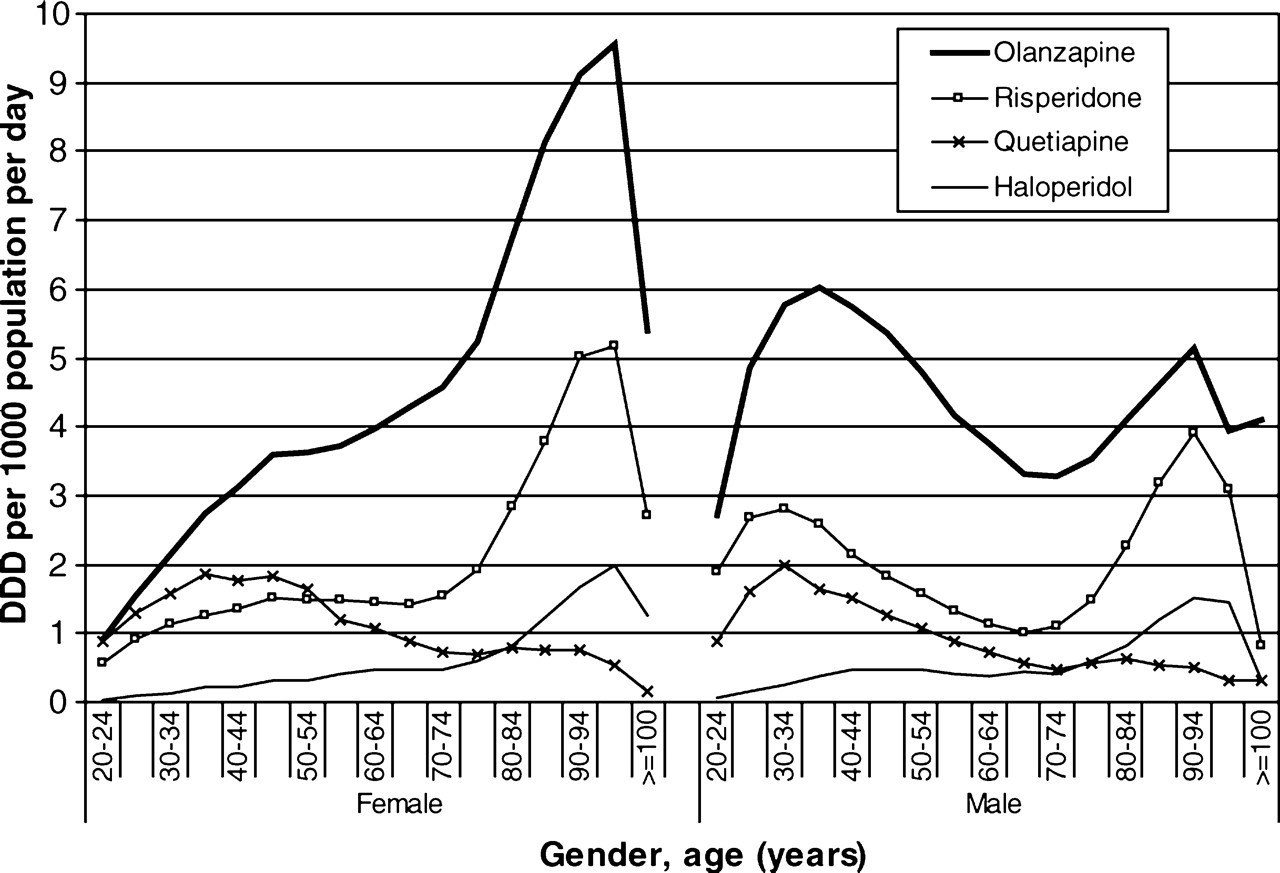
Drug utilization (defined daily dose (DDD)per 1000 population per day) for olanzapine, risperidone, quetiapine and haloperidol by gender and age (≥ 20 years) in 2006.
Risperidone use followed a similar pattern with a lower overall level of prescribing: there was less use in younger and more use in older women than men. Quetiapine was used more in the younger age groups than the older age groups. Haloperidol was used approximately the same in men and women but more often in the older than younger age groups.
In younger age groups the 10 mg tablet form of olanzapine was the dominant formulation for both men and women (Figure 3). Older men and women both had higher use of the 5 mg and 2.5 mg tablets, and women also had a higher use of the 5 mg wafer (data not shown).
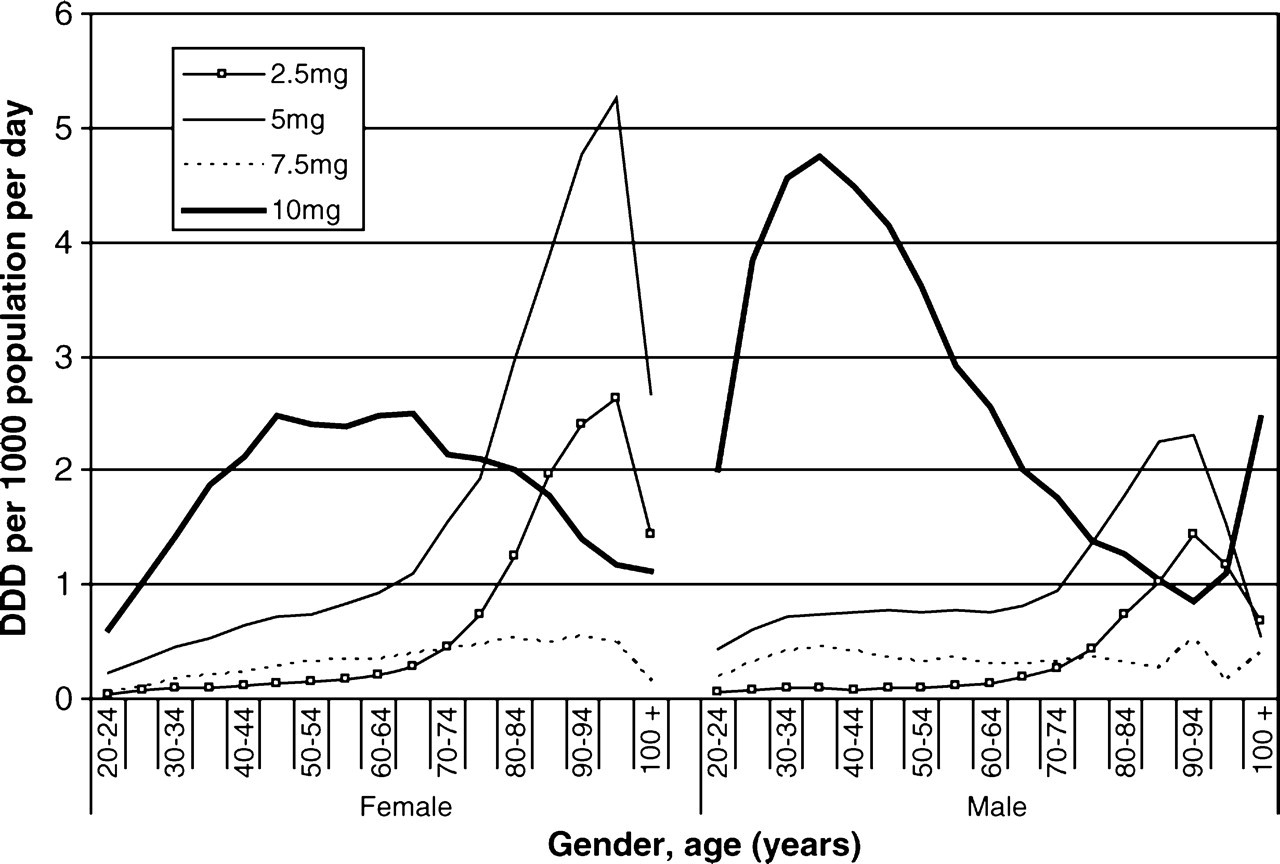
Drug utilization (defined daily dose (DDD) per 1000 population per day) of olanzapine dose formulations by gender and age (≥ 20 years) in 2006.
Analyses of atypical doses by prescriber category (GPs, psychiatrists or other specialists) showed that the pattern of doses prescribed for olanzapine and risperidone was similar between GPs and psychiatrists across all dose formulations. For quetiapine, however, GPs preferentially prescribed lower dose tablets than psychiatrists (25 mg: GPs 70%, psychiatrists 25%; 300 mg: GPs 55%, psychiatrists 38%).
Discussion
The use of atypical antipsychotics increased over the study period, with olanzapine and risperidone the dominant atypical antipsychotics used. There were substantial gender and age differences in the use of these drugs, particularly olanzapine, with considerable use in elderly women. There was greater use of lower dose formulations in those aged >60 years than those who were younger. There were marked differences in the patterns of olanzapine prescribing between men and women. Use among women was almost double that of men in the older age groups (in which dementia is more common). In the younger age groups (with the highest prevalence of schizophrenia) there was much more olanzapine use in men than women, possibly due to weight gain [11].
The present estimates may understate the use of these drugs in older women because the drug utilization calculations (DDD per 1000 population per day) were based on a dose of 10 mg of olanzapine that is used in schizophrenia. Because lower dose forms were more commonly used in the older age groups, this means that utilization of olanzapine for dementia in the older age groups has probably been under-enumerated. The actual drug utilization for this indication in older persons may accordingly be two–fourfold higher than we have calculated.
A 2006 Cochrane systematic review of atypical antipsychotic use in Alzheimer's disease showed that both olanzapine and risperidone were useful in reducing aggression, and that risperidone reduced psychosis [7]. Both drugs, however, caused increased extra-pyramidal side-effects and serious cerebrovascular events. The reviewers recommended against using these drugs routinely in dementia unless there was marked risk of severe distress or physical harm to those living and working with the patient [7].
The substantial use of olanzapine in elderly people has continued despite the PBS approval of risperidone for behavioural disturbances in dementia in 2005. Although there was a marginal decrease in olanzapine prescribing in the older ages (presumably substituting for risperidone), risperidone prescribing for dementia seems to have been added to the previous patterns of use. It also seems to have been added to the use of older typical antipsychotics, such as haloperidol, which have largely been prescribed for patients with dementia.
The introduction of risperidone for dementia (April 2005) closely followed the listing of the modified-release injectable form of risperidone (February 2005), which was quickly adopted (presumably for schizophrenia). Oral use increased only slightly after the listing for dementia and the increase was considerably less than that observed for the injectable form. This most likely represents a previously unmet need in schizophrenia.
Quetiapine appears to be primarily used for schizophrenia. A comparison of quetiapine prescribing by practitioner, however, showed that GPs prescribed a higher proportion of low-dose (25 mg) tablets compared to psychiatrists. This suggests that quetiapine may be used off-label for sedation, obsessive–compulsive disorder, post-traumatic stress disorder, personality disorder and substance abuse [12]. These patterns of use also noted in the USA [13] may also be occurring in Australia.
The present data are consistent with previous estimates of the use of these drugs in the Australian population [1,2] and in nursing homes [14–16]. In 2003 the Australian prevalence of schizophrenia was 4.4 per 1000 population [17]. There was a higher prevalence of schizophrenia in men than women (4.9 and 3.9 per 1000 population, respectively). The prevalence of bipolar disorder was 4.4 per 1000 population with a small difference between the genders (4.6 and 4.3 per 1000 population for men and women, respectively). Both men and women aged 20–55 years have the highest prevalence for both schizophrenia and bipolar disorder. An analysis of general practitioner consultations at residential aged care facilities (RACFs) showed that dementia was the most frequently managed problem and that schizophrenia was managed at twice the rate in RACFs compared to all usual GP encounters [18]. The highest prevalence for dementia was for people over the age of 65. The 2003 Australian prevalence for dementia was 8.4 per 1000 population, with a higher prevalence in women (6.2 and 10.6 per 1000 population for men and women, respectively) [17].
The present data indicate that a proportion of use of all atypical antipsychotic drugs (excluding risperidone) has been outside the approved subsidized indications of schizophrenia and bipolar disorder, despite an Authority Required restriction. The atypical antipsychotic drugs appear to have been used extensively in the older population to control behavioural disturbances in patients with dementia. Use has been markedly higher in older women than men. Such extensive utilization has had significant financial implications for the PBS.
Research is needed on the reasons for the extensive use and likely gender bias of these drugs in the elderly, particularly the twofold higher rate of use in women than men. It is also unclear why women in the younger age groups, in which schizophrenia has a similar prevalence in both genders, appear to be undertreated with these drugs compared to men. Further research is also needed to explore the characteristics of older women and men who receive these antipsychotics (e.g. how many are nursing home residents). Audits of selected patients >65 years who are taking these medications would be a useful start.
It is especially important to investigate the high rate of prescribing of atypical antipsychotics in the elderly given the recent research questioning their efficacy [19–21] and safety among elderly patients [7,22–25]. Atypical antipsychotics and concomitant use of anticholinergics also increase cognitive decline [26,27]. Further investigation of the use of these drugs is critical given the projected increase in persons with dementia in Australia [28].
Footnotes
Acknowledgements