
Abstract
Keywords
Velo-cardio-facial syndrome or 22q11.2 deletion syndrome (22q11DS), one of the most common genetic syndromes, occurs in approximately 1 in 5000 live births [1] and is associated with a microdeletion on the long arm of chromosome 22q11 in 97% of individuals [2]. The phenotypic variability is large but common features include congenital heart defects, characteristic facial dysmorphology, cleft palate, structural brain anomalies, and high rates of psychiatric disorder, particularly schizophrenia [3–6]. It is now well established that a general intellectual impairment is one of the key clinical features of 22q11DS [7,8]. Typically, general intellectual functioning is in the borderline range, and is unrelated to physical abnormalities such as cardiac and palatal anomalies [3]. In the last decade studies outlining the specific cognitive profile in 22q11DS have begun to emerge. These studies indicate that 22q11DS is characterized by multiple impairments in arithmetic and numeracy [9,10], object perception [11], memory [12–18], executive function [11,12,16,19], attention [12,14,16,20] and communication skills and language [21–24]. Indeed, it has been suggested that the same pattern of cognitive deficits is present in both children with 22q11DS (who are at a high risk of developing psychosis) and in non-22q11DS people with schizophrenia [16]. Many early studies of cognition in 22q11DS, however, were confounded by small sample sizes and the lack of appropriately matched control groups. Nevertheless, because impairments of attention and memory may be early childhood predictors of the future development of schizophrenia-related psychoses [25], it is important to accurately characterize the cognitive deficits in 22q11DS and the relationship to the behavioural expressions.
The gene coding for catechol-O-methyltransferase (COMT), the enzyme that metabolizes dopamine (especially in the prefrontal cortex), has attracted most attention as a possible modulator of the cognitive deficits in 22q11DS. Due to its location on chromosome 22q11.2, people with 22q11DS are hemizygous for either the low activity, Met 158 or the high activity Val108 polymorphism. Although COMT genotype has been associated with working memory function in the general population [26], the role of COMT in modifying cognitive function in 22q11DS is unclear. Some studies report that Met hemizygosity in 22q11DS is associated with poorer expressive language and working memory [27], decreased verbal IQ and expressive language [28]. Other studies, however, report that Met hemizygosity predicts higher full-scale IQ (FSIQ), verbal IQ, mathematical scores [29] and better executive function [26, 28–32], while others failed to find any associations between COMT genotype and cognition [33,34].
In the current study we utilized an extensive battery to further characterize memory, executive functioning and attention/inhibition abilities in a large sample of children and adolescents with 22q11DS. We hypothesized that (i) children with 22q11DS would have specific impairments of memory, executive functions and attention; and (ii) possession of the COMT val158 allele would be associated with impaired executive function.
Methods
Participants
We included 50 children (28 female) aged 6–16 years (mean =11 years, SD = 3), with a confirmed deletion of chromosome 22q11.2 as measured using fluorescence in situ hybridization (Oncor, Gaithersburg, MD, USA). We also included 31 sibling controls (13 female) aged 6–16 years (mean = 12 years, SD = 3), to control, as best we could, for environmental factors, socioeconomic status, and age. We excluded participants with the clinical phenotype of 22qDS but without the large 3 Mb 22q11.2 deletion, those with a clinically detectable medical disorder known to affect brain structure (e.g. epilepsy or hypertension), or a history of head injury. A chromosome 22q11 deletion was excluded in all sibling controls.
Participants were recruited through the family support group, Velo-cardio-facial syndrome (VCFS-UK). Informed written consent was obtained from carers of the participants and recruitment procedures were carried out in accordance with protocols approved by local and the multi-centre research ethics committees.
Cognitive testing
General intellectual functioning was assessed using the full Wechsler Intelligence Scales for Children-third edition (UK) (WISC-III) [35] enabling the establishment of verbal IQ (VIQ) and performance IQ (PIQ). The raw scores on the subtests are transformed to scaled scores in order to calculate the FSIQ, VIQ (Information, Similarities, Arithmetic, Vocabulary, Comprehension, Digit Span) and PIQ (Picture Completion, Coding, Picture Arrangement, Block Design, Object Assembly, Symbol Search) and factor index scores, verbal comprehension, perceptual organization, processing speed and freedom from distractibility. The population mean is 100 and the standard deviation is 15.
Memory
We used the Children's Memory Scale (CMS) to measure generalized learning and memory ability, and auditory/verbal and visual–spatial memory [36]. The battery provides index scores of verbal and visual immediate memory, verbal and visual delayed memory, delayed recognition, attention/concentration and learning. Each index score is derived from the subtests (i) Dot location; (ii) Faces; (iii) Stories; (iv) Word pairs; and (v) Sequences. In each case a scaled score was computed.
To measure executive function in the current study, three tasks from the computerized Cambridge Neuropsychological Testing Automated Battery [37] were utilized.
(1) Attentional set formation and set shifting was examined using the Intradimensional/Extradimensional set shifting task (ID/ ED)[38]. This contains nine stages during which the participants are required to learn to discriminate visual stimuli, by trial and error. The main performance measures are number of stages completed, number of errors prior to the Extra-dimensional shift (pre-EDS shift; set formation and maintenance) and the number of errors in the EDS shifts (specific measure of set shifting).
(2) Planning ability was tested using the Stockings of Cambridge (SOC) [39] a computerized variation of the Tower of London task originally designed by Shallice [40]. The main measures were the number of problems solved in the minimum number of moves, the average number of moves above the minimum at each level, the initial thinking time (i.e. the time it takes to initiate solutions minus the initiate time in the motor control section) and the subsequent thinking time (time taken to complete solutions minus time taken to complete motor control items).
(3) Spatial working memory and strategy formation was investigated using the Spatial Working Memory task (SWM), requiring the participants to search through a specific number of boxes and locate blue tokens hidden inside [39]. Once one had been located they should search for a new target location, with the rule that the old target locations will not be repeated. Main measures were (i) within-search error (when the subject searched the same box more than once in the same sequence); (ii) between-search error (when a subject returned to a location in which there had already been a target); and (iii) strategy (efficiency) of searches [39]. A high score represents poor use of this strategy and a low score equates to effective use, the minimum strategy score was 1 for each stage (i.e. 8) and the maximum was 1 for each search (i.e. 56).
To measure cognitive flexibility and inhibition three tasks from the Maudsley Attention and Response Suppression battery was included [41].
(1) The Switch task was used to investigate cognitive flexibility, that is, the ability to inhibit previously learned stimulus–response associations in order to facilitate new stimulus–response associations (attentional switch) [42]. The task was developed to minimize involvement of working memory functions. For more details, refer to Smith et al. [42].
(2) Inhibition of motor responses was measured using a Go–NoGo task (GNG) in which the subject has to either execute or inhibit a motor response depending on whether a go (70%) or no-go (30%) stimulus appear on the screen; these stimuli are in the form of space ships (Go) and enemy planets (NoGo).
(3) Inhibition of interference and selective attention were assessed on a Stroop task. In this task, spaceships pointing left appear on the left side of the screen, while spaceships pointing right appear on the right side of the screen (congruent trials). In 30% of the trials, spaceships pointing left appear on the right and spaceships pointing right appear on the left side of the screen (incongruent trials). Subjects must indicate in which direction the spaceship is pointing, thus inhibiting the interference introduced by the incongruency of the position of the spaceship on the screen.
COMT genotyping
The SNaPshot technique of single base extension (Applied Biosystems, Foster City, CA, USA) was used for individual genotyping of the COMT Val108/158Met polymorphism in 34 participants with 22q11DS (due to methodological reasons, COMT data from 16 participants were missing). The forward primer 5′-ACTGTG GCTACTCAGCTGTG-3′ was used for the initial polymerase chain reaction in addition to the reverse primer 5′-CCTTTTTCCAGGTCT GACAA-3′. A 30 bp extension primer was constructed for the extension reaction (5′-ATCACCCAGCGGATGGTGGATTTCGCT GGC-3′). Alleles were resolved on an ABI 3100 sequencer. Twenty-three 22q11DS children (11 female, mean age =11 years, SD = 3) were 158Met hemizygous and 11 (six female, mean age = 10 years, SD = 2) were Val108 hemizygous.
Statistical analysis
Sociodemographic characteristics of the two groups were compared using independent t-tests and χ2 analysis. Cognitive data were tested for conformity to a normal distribution, and if not present a natural log or square root transformation was applied. When outliers were identified, data were analysed with and without the subject to investigate the effect on the outcome of the statistical testing. One extreme outlier was excluded in the Stroop task. The variable ‘within-search error’ from the SWM task was collapsed due to low variability. In the SOC and SWM task the lowest levels were discarded due to ceiling effects.
A one-way between-group multivariate analysis of variance (MANOVA) was performed to investigate group differences in the CMS. Within-group index score and subtest analyses of memory were performed using paired samples t-tests. Gamma comparisons for ordinal data were conducted to investigate the predicted-actual memory index score of the CMS, these scores provides an opportunity to investigate how a child performs in relation to their FSIQ score, thus obtaining a label performing worse than, as expected, or better than expected from their FSIQ score.
Within-between mixed ANOVA were used in the variables of mean initial thinking time and subsequent thinking time in the SOC task; the variables of reaction time (RT) and accuracy in reaction time (RT) in the Switch task, and for the variables of standard deviation (SD) of reaction time and error in the Stroop task. Independent sample t-tests or appropriate non-parametric tests were used for the remainder of the continuous data.
For all cognitive variables a conservative alpha of p < 0.01 (two-tailed) was assumed as the threshold for statistical significance in order to control for multiple comparisons, while p < 0.05 was considered a trend. The effect sizes were obtained from the SPSS output, partial eta squared (ηp 2; 0.01 = small, 0.06 = moderate, 0.14 = large; SPSS, Chicago, IL, USA). The n in each task is reported, indicating missing data due to lack of completion by subjects or by equipment failure.
Results
The groups did not differ significantly in mean age or gender distribution (Table 1). As expected, however, the 22q11DS group had a significantly lower FSIQ. Within children with 22q11DS, VIQ, PIQ and index scores were largely in the normal borderline-mild learning disability range (although the variability within the group was large; Table 2).
Demographic information
22q11DS, 22q11 deletion syndrome.
General intellectual profile
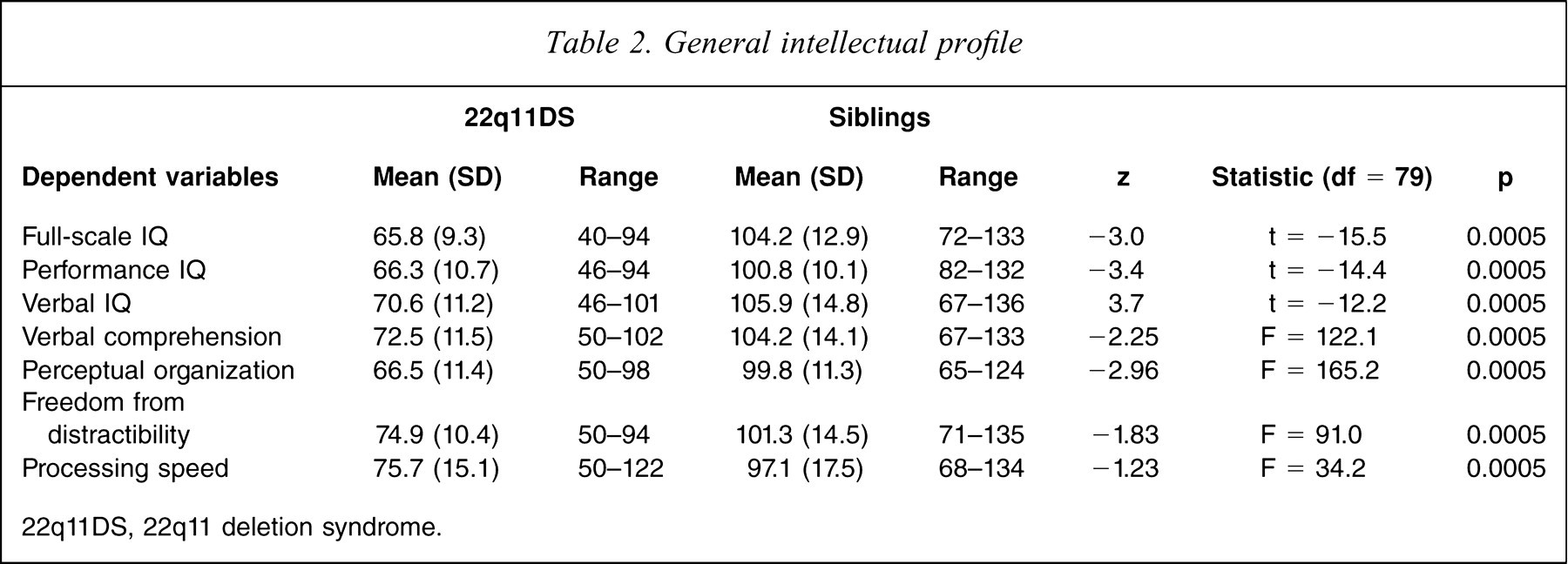
22q11DS, 22q11 deletion syndrome.
Memory
The 22q11DS group performed in the low average-borderline range on all the CMS memory index scores but in the group analyses their performance was significantly lower than their siblings on all memory index scores (p < 0.004; Table 3). The 22q11DS group performed significantly worse than (predicted-actual memory index score) expected from their FSIQ score more frequently than controls in visual immediate memory (γ = 0.56, n = 78, p = 0.002) and a similar trend was detected in visual delayed memory (γ = 0.54, n = 78, p = 0.02) only. Verbal memory (immediate and delayed: r = 0.38, df = 44, p = 0.07; r = 0.36, df = 48, p = 0.01) and learning was positively associated with intellectual functioning.
Cognitive data
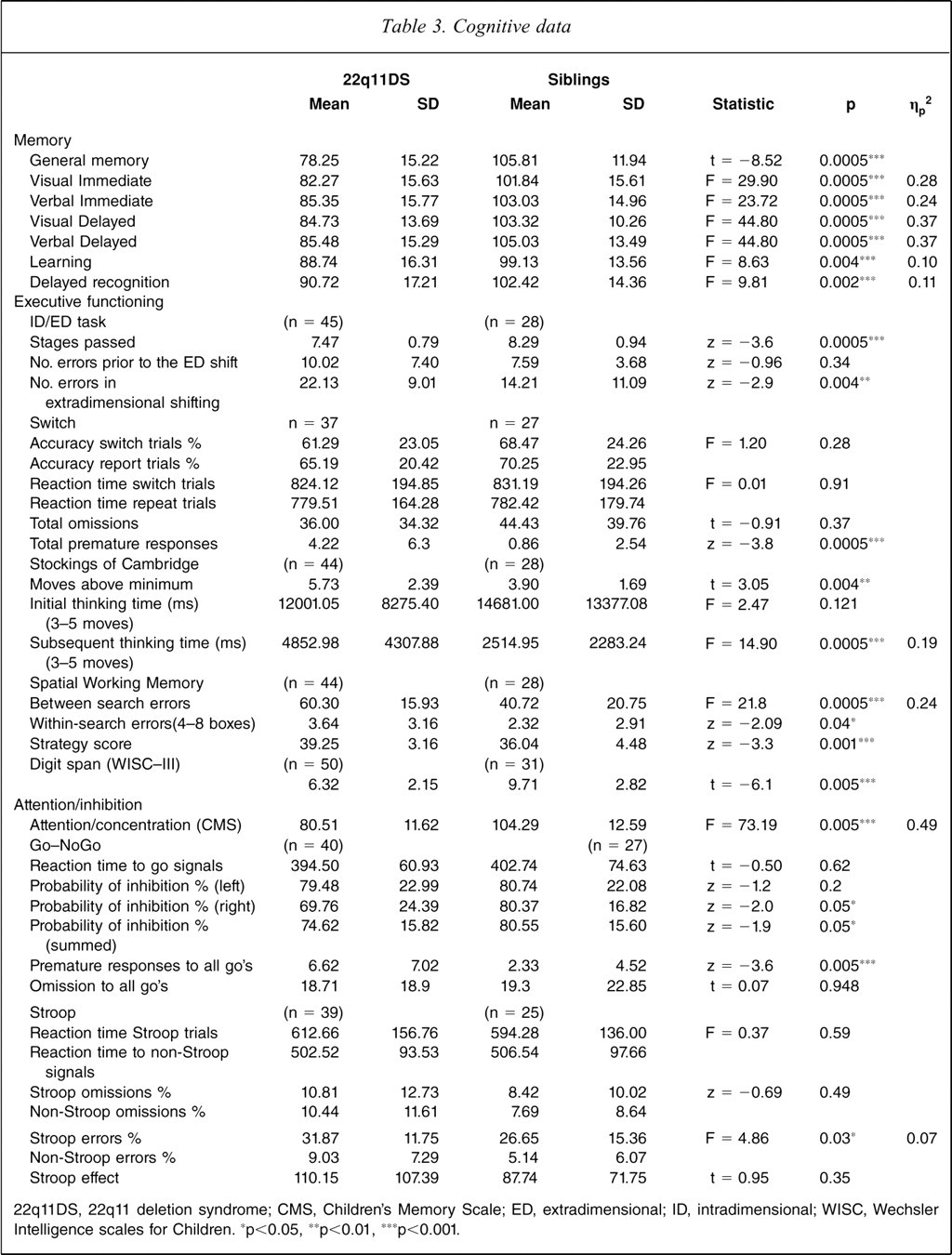
22q11DS, 22q11 deletion syndrome; CMS, Children's Memory Scale; ED, extradimensional; ID, intradimensional; WISC, Wechsler Intelligence scales for Children. ∗p<0.05, ∗∗p<0.01, ∗∗∗p<0.001.
In order to investigate the performance on individual subtests, further subsidiary analyses were performed. To explore potential differences between types of visual and verbal memory, within-group paired-sample t-tests were performed. In the non-verbal domain the 22q11DS group performed significantly better on the Dots task compared with the Faces task (immediate: t(47) = 4.4, p < 0.0005; delayed: t(47) = 6.1, p < 0.0005), while the performance on the verbal tasks were comparable (p > 0.05). In the recognition tests the 22q11DS group performed better at the Word recognition compared with the Stories recognition task (t(47) = −2.8, p < 0.008). The sibling group had more problems with the delayed Faces task compared with delayed Dots (t(30) = 2.9, p < 0.006) but no other task performance differences were seen. To explore forgetting paired t-tests were used within the groups for immediate versus delayed recall. These showed no significant effects for either group (p > 0.05).
Executive functioning
The 22q11DS group completed fewer stages and had more errors after the ED shift compared with siblings in the ID/ED task (Table 3). In the Switch task there was no accuracy × group interaction or main effect of group, but the 22q11DS subjects made more premature responses than the siblings. In the SOC task the 22q11DS group spent more time thinking during the tasks but still made significantly more moves to complete each problem compared with the sibling group. In addition, the 22q11DS group made more between-search errors and had worse strategy scores on the SWM task. Finally, the 22q11DS had a shorter Digit span as measured on the WISC-III than the sibling group.
Attention/inhibition
Children with 22q11DS performed significantly worse at the attention/concentration index of the CMS (Table 3) but not lower than expected from their general intellectual ability (p > 0.05). There were no between-group differences in the GNG or the Stroop task except that 22q11DS children made significantly more premature responses than sibling controls in the GNG task.
COMT genotype and cognition
There was no significant age difference (t(32) = −1.31, p = 0.2) or gender distribution (Fisher's exact test, two-sided = 1.0) in the two subgroups of children with 22q11DS (Table 4). There were no significant associations between the COMT Val108/158Met polymorphism and cognitive or behavioural variables. Splitting the group according to age (below or above 10 years) or gender and repeating the analyses in the young and older age group or according to gender did not change the results.
COMT genotype and cognitive data
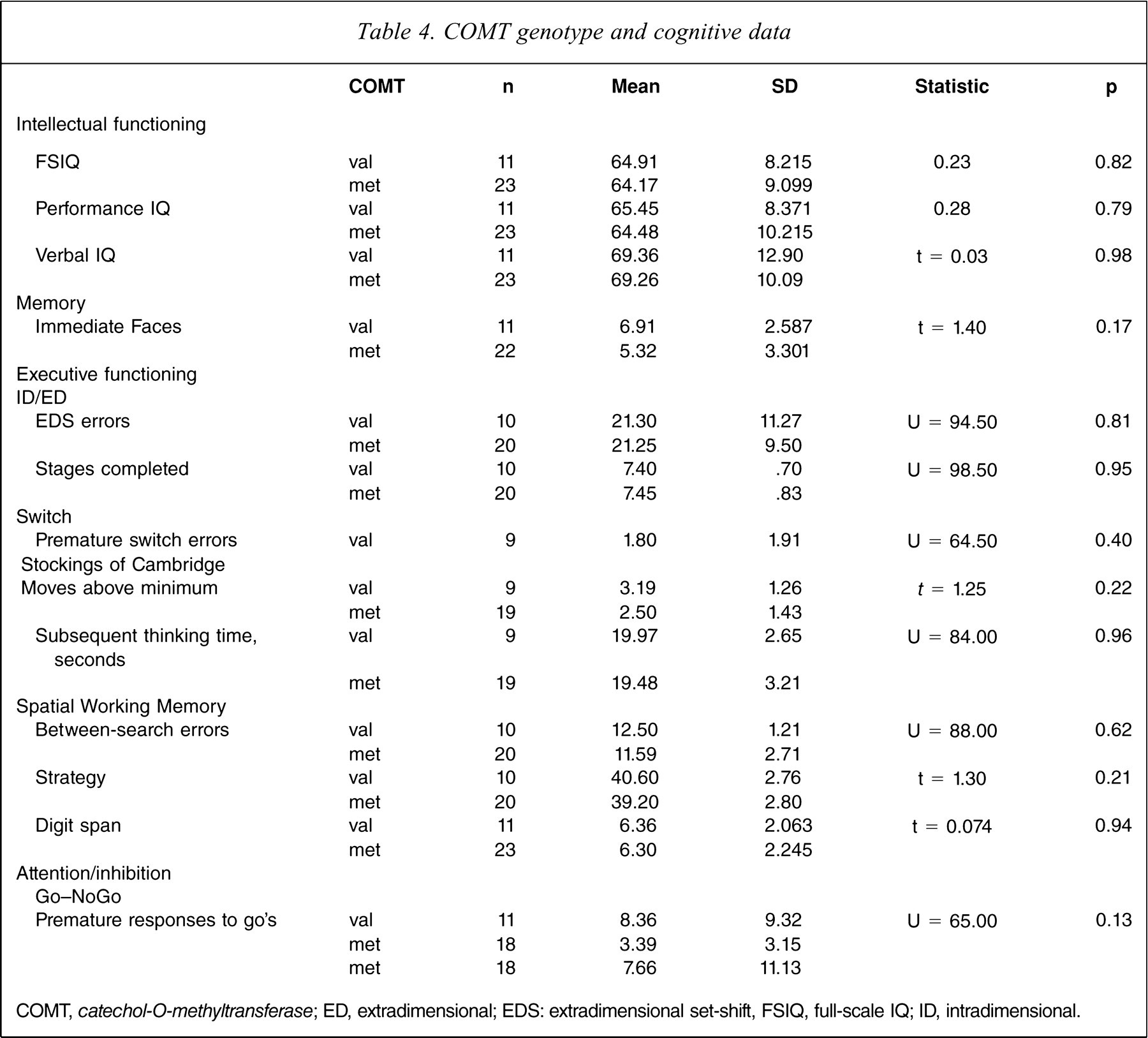
COMT, catechol-O-methyltransferase; ED, extradimensional; EDS: extradimensional set-shift, FSIQ, full-scale IQ; ID, intradimensional.
Discussion
We investigated the cognitive phenotype in a large cohort of children and adolescents with 22q11DS and found that, compared to sibling controls, children with 22q11DS had lower general intellectual ability, impaired planning abilities and impaired spatial working memory. Furthermore, cognitive impairments in the 22q11DS group were unrelated to COMT genotype.
The present results confirm previous reports that memory abilities of children with 22q11DS are within the lower average range but that there are more problems in the visual compared with the verbal memory domain [12–15,17]. The present study found that more children with 22q11DS performed worse than expected (with respect to their FSIQ score) on visual memory. This discrepancy, however, was not found on the verbal subtests (on which they performed as expected). The impairment in visual memory was driven by a lower performance on the Faces subtest compared with the Dots subtest, which may indicate more difficulties in processing, organizing and holding of more meaningful visual/non-verbal materials. The difference in performance, however, on the Faces and Dots subtests could also possibly be attributed to dissimilarities in the organization of the tasks, because the Dots test, for example, is a repetitive learning task while Faces is a one-trial learning task. Hence the findings may be indicative of the need of children with 22q11DS for additional structure, that is, repetitive learning in order to consolidate and store visual/non-verbal material [36]. This latter explanation is consistent with earlier reports of superior performances with repeated exposure among children with 22q11DS [3,9]. In addition, the controls also had more difficulties, at least with the delayed component of the Faces task compared to the Dots task, indicating that the task may be more taxing. Considering the social-emotional problems experienced by people with 22q11DS [12,43] and the reported high prevalence of autistic spectrum disorders in the population [44,45], this warrants a specific investigation of facial perception in this group.
Earlier studies of children with 22q11DS have suggested set-shifting impairments in the Wisconsin Card-Sorting task [12,16]. The current study found that the 22q11DS group displayed a deficit in the set-shifting ID/ED task, with an increased error rate at the extradimensional set-shifting stage, indicating impaired cognitive flexibility, while no group differences were found in set formation, that is, before the extradimensional shift. There was a lack of group differences, however, in the subsequent Switch task, in which the working memory component was minimized to enhance the switching effect. In addition, there was no correlation between performance on the ID/ED and the Switch task, indicating that different cognitive functions may be underlying task performance. It is possible that the influence of working memory could be a plausible explanation for the observed impairment in the ID/ED task because we found that children with 22q11DS have impairments of working memory, replicating the findings from previous studies [17,46]. We have previously reported that adults with 22q11DS have impaired planning [11], a finding replicated in the current study, in which children with 22q11DS had difficulty formulating an efficient strategy in the SWM task and in the SOC task. The data from the SOC task suggest that, although the children with 22q11DS began their solutions after a slightly shorter delay compared with controls, they spent more time thinking about the task once begun, indicating that they did not formulate a proper strategy before beginning the task and hence had a need to monitor and correct these plans throughout the task (resulting in increased moves), a difficulty previously observed in children with 22q11DS [12] and in patients with frontal lobe damage [39]. Planning responses to tasks such as the SOC are also dependent on working memory abilities and response inhibition. While the former has been found to be impaired in 22q11DS (as discussed earlier), inhibitory impairments were not located in the current study. Furthermore, even though children with 22q11DS displayed a general impairment in attention/concentration, this deficit was proportional to their lower general intellectual ability. The 22q11DS subjects, however, displayed an increased prevalence of premature responses, which could be explained by a lack of appropriate motor response.
We did not identify a relationship between COMT genotype and the cognitive measures investigated in the current sample. Although the present results are consistent with data reported by Glaser et al. [33], other studies of children and adolescents with 22q11DS have argued that COMT genotype is related to, at least, prefrontal function in 22q11DS, although the impact may be age and gender dependent [27–29,47]. Therefore we performed additional analyses to investigate if performance on the cognitive tasks was modulated by age or gender and COMT genotype. No such effect, however, was found. Although the sample size and age range of the current study was comparable to earlier studies, the inconsistencies between the current and earlier studies may be linked to differences in the cognitive measures used. We would like to suggest, however, that the findings from the current study and from the Glaser et al. study [33] highlight the complexity of the relationship between genotype and phenotype even when delineating a disorder caused by an identified deletion. Interestingly, a recent study has indicated that the interaction between COMT genotype and proline levels may modulate brain function in children with 22q11DS [48]. Studies of other disorders also highlight the importance of gene × environment interactions for the phenotype. Hence, the relationship between cognitive functions and the genotype is likely to be complex. Future analyses need to incorporate more comprehensive information about the genotype as well as other factors that may shed more light on this issue.
In conclusion, we replicated and extended earlier findings of impairments of memory (especially visual memory) and executive functions in children with 22q11DS and demonstrated that children with 22q11DS have specific deficits within these domains. Surprisingly we did not identify any correlation between COMT genotype and cognition or brain structure. The present study was limited in its cross-sectional design and hence a longitudinal extension of this study is planned to investigate the relationship between changes in cognition and COMT genotype. We incorporated many comparisons in the study and tried to limit type 2 errors by using conservative p.
Footnotes
Acknowledgements
We would like to thank all children and their families who participated in this study and the 22q11DS-UK support group for all the help and assistance received over the years. We would also like to thank Dr Chris Barnes, Guy's Hospital, and other colleagues in clinical genetics for their help with recruiting subjects. This work was supported by a grant from the Healthcare Trust.