
Abstract
Despite extremely high cigarette smoking rates among people with a psychotic disorder, and associated financial and health costs [1], smoking is often not addressed by clinicians, even when acute psychotic symptomatology has been well managed. Clinicians may feel ill-equipped to address smoking, given that few randomized controlled trials of smoking cessation interventions have been conducted among this group and most existing studies report only short-term outcomes, usually up to 6 months [2]. Given the paucity of information on smoking, symptomatology and functioning following smoking cessation treatment among people with psychosis, the aim of the present study was to improve current understanding of prognosis among this group following participation in a smoking cessation study.
While there is accumulating evidence that smoking reduction increases the probability of future cessation among samples without mental disorders [3], to our knowledge only one small study has reported longer-term follow up of smoking reduction among people with a psychotic disorder [4]. Reduction status (e.g. the proportion achieving a ≥50% reduction) may be a particularly useful index among people with a psychotic disorder following smoking cessation treatment [4]. In that study, 18 subjects with schizophrenia were treated with bupropion and cognitive behaviour therapy (CBT) and followed up at 12 weeks and 2 years. Of the seven subjects who reduced their smoking by ≥50% at the end of the trial, six maintained that reduction at 2 years, with four of these becoming abstinent. Evins et al. concluded from their naturalistic study that people with psychosis who were able to reduce their smoking during a trial were capable of maintaining such a reduction at 2 years [4]. They further concluded that smoking reduction during an intervention may also predict later cessation in this group. They noted, however, that the small sample size, absence of a control group and the naturalistic nature of the follow up limited the conclusions that can be drawn.
Studies of the health consequences of reduced daily cigarette consumption among heavy smokers have not yielded clear evidence of physical health benefits [5]. Smoking reduction, however, might be considered as a step in the right direction because no new risks are introduced to the smoker, there is reduced harm to others and other people are unlikely to adopt smoking just because they know they can smoke fewer cigarettes [6]. In addition, as smokers with psychosis are typically of lower socioeconomic status [7], there is an additional important financial benefit associated with smoking reduction. Reduced use of drugs has been recognized as possible for dependent users of other drug classes (e.g. alcohol [8]), and among people with psychosis [9,10]. Despite the potential benefits of smoking reduction, however, surprisingly little attention has been directed towards the investigation of longer-term smoking reduction among people with psychosis or to the use of other indices of improvement.
This naturalistic long-term follow-up study is the largest to date to investigate whether smoking reduction status at 1 year following a smoking cessation trial was related to that at 4 years, among a sample of people with a psychotic disorder. The 1 year follow-up results of the original randomized controlled trial are reported elsewhere [11]. Briefly, 298 regular smokers with a psychotic disorder residing in the community were allocated to a routine care comparison condition (n = 151) or an eight-session, individually administered smoking cessation intervention (n = 147), consisting of nicotine replacement therapy (NRT), motivational interviewing (MI) and CBT. Although there were no overall differences between the treatment and comparison groups in abstinence rates, a significantly higher proportion of smokers who completed all eight treatment sessions had quit smoking at each of the follow ups compared to those with partial treatment attendance (point prevalence rates: 3 months, 30.0% vs 6.0%; 6 months, 18.6% vs 4.0%; and 1 year, 18.6% vs 6.6%). There was also a strong dose–response relationship between treatment session attendance and smoking reduction status, with no evidence of any associated deterioration in symptoms or functioning.
Previous studies among the general population have not found predictors of longer-term change. For example, in a 3 year follow-up study of smoking cessation among patients from a general practice setting, no predictors of 3 year abstinence were found [12]. A recent meta-analysis of the long-term efficacy of NRT versus placebo in treatment trials in the general population reported only modest effects of NRT beyond 12 month follow up [13]. We predicted that (i) the majority of subjects who reduced their smoking at the 1 year follow up in the previous smoking cessation trial [11] would maintain that reduction at 4 years; and (ii) smoking reduction at 1 year would be associated with greater rates of abstinence at 4 years, compared to those who had not reduced their smoking by ≥50%.
Method
Participants and procedure
The initial smoking cessation trial has been described previously [11,14], and consisted of 298 smokers with a non-acute psychotic disorder who were recruited from Sydney and the Newcastle region of NSW, Australia. Inclusion criteria were (i) age ≥18 years; (ii) smoking >15 cigarettes per day; and (iii) International Classification of Disorders (ICD-10) diagnosis of schizophrenia, schizoaffective disorder, bipolar disorder, severe depression with psychotic features, or other psychotic disorder [15]. Participants were also required to express an interest in quitting smoking. Exclusion criteria were (i) medical conditions that would preclude use of nicotine patches; (ii) being acutely psychotic (in which case, participants were reassessed 1 month after screening); and (iii) evidence of cognitive impairment.
Participants were randomly assigned to one of two conditions: routine mental health care (no specific smoking advice) or an eight-session intervention consisting of NRT, MI and CBT. Four assessment phases were planned (baseline, 3 and 6 months, and 1 year follow up), with the 4 year follow up an addition to the original study. All follow-up interviews were conducted by researchers who were blind to treatment allocation. This paper reports on predictors of outcome at 1 year (n = 247) and 4 years (n = 164) and associations between outcomes at 1 and 4 years (n = 149). At 4 years, last known contact details were used as the basis of contact for participants and next of kin (if necessary). Two weeks following a contact letter, the research team telephoned each participant. At least five attempts were made to contact each participant by telephone, including two evening calls. If contact was unsuccessful, the participant's next of kin was telephoned, several times if necessary. But if this proved unsuccessful, after a period of at least 2 weeks, the participant's last known case manager or treating health professional was contacted with a view to them providing information about the 4 year follow-up study to the participant. If this final attempt to contact the participant was unsuccessful, no further contact attempts were made.
Upon contact with participants, permission was sought to mail them the information sheet and consent form relating to the study. If participants agreed, an appointment was arranged (n = 156) or assessments were conducted over the telephone (n = 8) for those participants unable to attend the study clinics. Participants were reimbursed $AUD20 for the time taken to attend the follow-up interviews and transport and parking costs. Ethics approvals were obtained from relevant regional and university ethics committees in Sydney and Newcastle.
Measures
Smoking-related measures
The main outcome measures from the original study were re-administered 4 years after the baseline assessment and have been described previously [11,14]. The primary smoking outcome measures were continuous abstinence; point prevalence abstinence; and smoking reduction status. These were all evaluated on a treatment efficacy (as opposed to a program effectiveness) basis [16], with no attempts to impute missing data (or to conduct intention-to-treat analyses). This decision was taken based on the naturalistic nature of the 4 year follow up, the relatively high attrition rate, and the absence of associations between baseline characteristics and retention status. Secondary smoking outcome analyses were based on the amount of treatment actually received, on a self-selection basis. Continuous abstinence refers to the proportion of participants who reported not smoking at all from the nominated quit date to the 1 and 4 year follow-up assessments. Point prevalence abstinence refers to the proportion of the sample who had been abstinent for the 7 days preceding the follow-up assessment points. Smoking reduction status between baseline and 1 year follow up was categorized into four subgroups: no reduction; <50% reduction; ≥50% reduction; or abstinence. Likewise, smoking reduction status at 4 year follow up was categorized into similar subgroups (relative to smoking at baseline). Current abstinence from smoking was confirmed using a Micro 11 Smokerlyser (Air-Met Scientific Pty. Ltd., Melbourne, Victoria, Australia), which assesses breath levels of carbon monoxide (CO). A CO level <10 p.p.m. signified that the participant was unlikely to have smoked in the last 8 hr. Nicotine dependence was measured by the Fagerstrom Test for Nicotine Dependence (FTND) [17]. Motivation to quit smoking was measured using the 11-item Readiness and Motivation to Quit Smoking Questionnaire [18], which provides an elaborated stages of readiness scale, ranging from 0 (pre-contemplation level 1: not contemplating quitting or cutting down) to 4 (preparation stage).
Measures of psychopathology and quality of life
Psychiatrie symptoms were assessed using the 24-item Brief Psychiatric Rating Scale (BPRS-24) [19]. The Beck Depression Inventory II (BDI-II) [20] and the State–Trait Anxiety Inventory (STAI) [21] were used to assess depression and anxiety symptoms, respectively. General functioning was measured using the 12-item Short Form survey (SF-12) [22], which produces mental component scores (MCS) and physical health component scores (PCS), with lower scores indicating greater disability. ICD-10 diagnoses were obtained via the Diagnostic Interview for Psychosis [23]. Recent alcohol and cannabis use were assessed using the Opiate Treatment Index (OTI) [24].
Statistical analyses
Data were analysed using SPSS (version 14 for Windows; SPSS, Chicago, IL, USA). For the key smoking-related categorical outcome variables, differences between the overall treatment group (n = 127 at 1 year; n = 83 at 4 years) and the comparison group (n = 120 at 1 year; n = 81 at 4 years) were analysed, together with selected subgroup analyses based on patterns of treatment session attendance and also on smoking status at follow up. Odds ratios (OR) and associated confidence intervals (CI) are reported, with the comparison group as the reference point (OR = 1.00). Chi-squared tests were also used for other categorical variables. For the continuous outcome variables (e.g. cigarettes per day), planned comparisons between assessment phases, from repeated-measures analyses of variance (ANOVA), were used to examine group differences in patterns of change. As a partial control for the number of statistical tests, the threshold for statistical significance was set at p<0.01.
Results
Variables associated with retention status at follow up
The 4 year follow-up assessment occurred on average 3.99 years (SD = 0.57) following baseline assessment. Because we were primarily interested in examining smoking reduction status at 1 and 4 years, retention status at follow up was classified into the following three groups: completed neither 1 or 4 year follow ups (n = 51); completed the 1 year follow up only (n = 98); or completed both the 1 and 4 year follow ups (n = 149). There were no significant differences at baseline between these three groups in terms of: gender, age, or body mass index; diagnosis (schizophrenia/schizoaffectivevs other psychotic disorders), medication status, or course of psychiatric disorder since initial diagnosis; age at first cigarette use, age at commencement of daily smoking, or baseline scores for number of cigarettes per day, number of quit attempts, level of nicotine dependence, or stage of change; baseline psychopathology scores (BPRS-24 global score, STAI state and trait anxiety, mental and physical functioning on the SF-12); or smoking cessation treatment group allocation status, or the number of treatment sessions attended (within the treatment group). In short, retention in the follow-up study was not associated with any obvious biases.
Sample characteristics
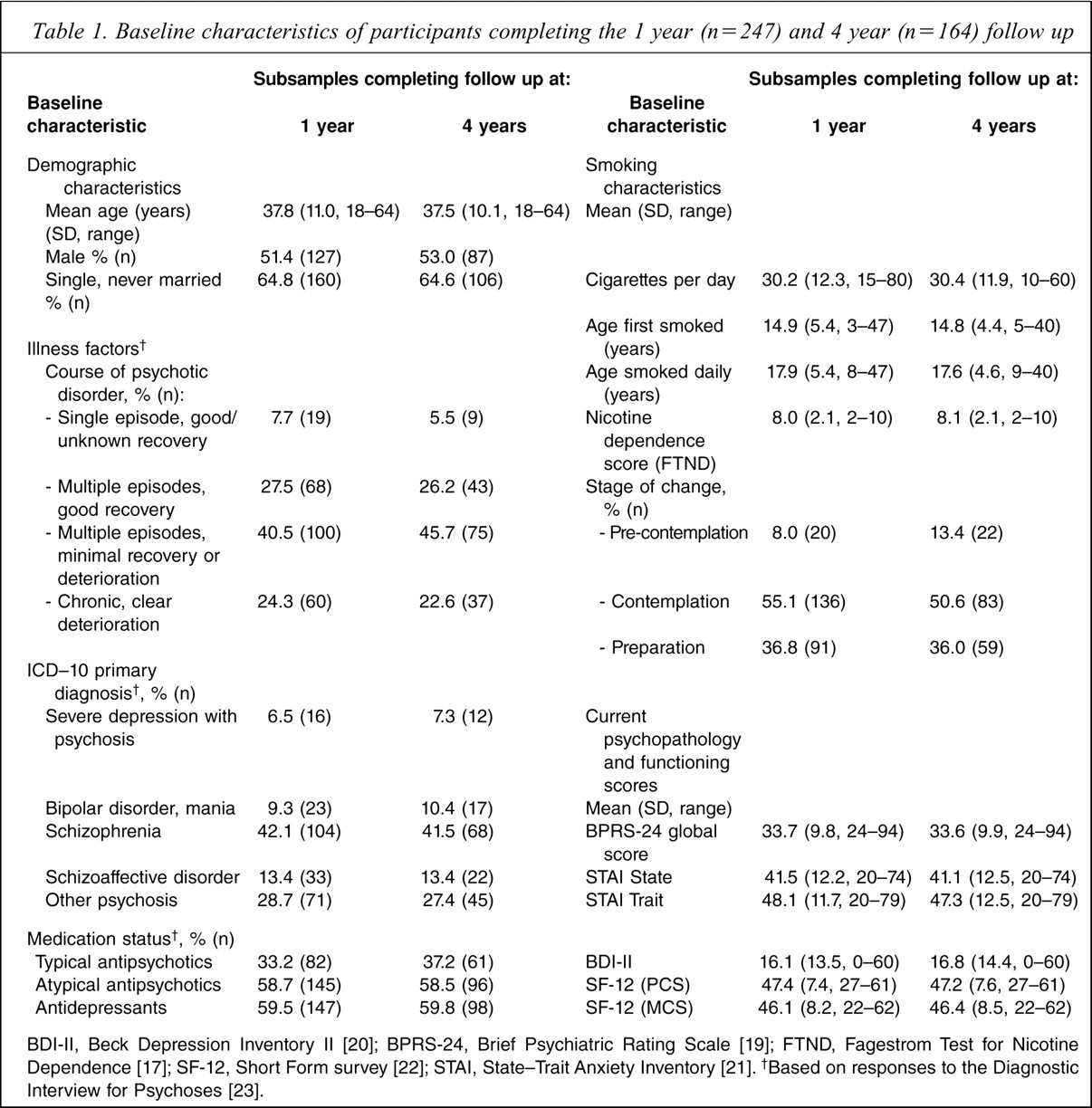
Baseline demographic, clinical and smoking characteristics are reported in Table 1 for the sample of people who completed the 1 year follow up (n = 247) and those who completed the 4 year follow up (n = 164). The baseline characteristics for these two subsamples were similar. At the 1 year follow-up, the smoking reduction status subgroups were distributed as follows: no reduction, 94 (38.1%); <50% reduction, 75 (30.4%); ≥50% reduction relative to baseline, 49 (19.8%); and abstinent for ≥7 days, 29 (11.7%). At the 4 year follow up, for those people who also completed the 1 year follow up (n = 149), the corresponding values were: no reduction, 48 (32.2%); <50% reduction, 50 (33.6%); ≥50% reduction relative to baseline, 24 (16.1%); and abstinent for ≥7 days, 27 (18.1%).
Baseline characteristics of participants completing the 1 year (n = 247) and 4 year (n = 164) follow up
Variables associated with smoking status at 1 year follow up
The following baseline variables were analysed as possible predictors of 1 year smoking Status: gender, age, diagnostic subgroup, medication status, number of previous quit attempts, number of cigarettes per day, and scores on the following scales: the FTND, BDI-II, STAI, BPRS-24, OTI alcohol and cannabis subscales, and the SF-12 mental and physical components. The number of intrinsic versus extrinsic reasons for quitting, stage of change, whether participants were allocated to treatment or comparison conditions, and the number of sessions attended were also analysed. With the exception of treatment status (χ2 = 24.51, df = 9, p < 0.01), none was a significant predictors of 1 year smoking status. Among those who attended all eight treatment sessions (n = 63), 31.7% reported a≥50% reduction at the 1 year follow up, while an additional 20.6% reported abstinence at that time. Across the remaining subgroups, the corresponding rates were 15.8% (29/184) and 8.7% (16/184), respectively. The individual smoking outcome variables are examined further in the following section.
Variables associated with smoking status at 4 year follow up
The same variables, assessed at baseline and 1 year, were analysed as potential predictors of 4 year smoking status. None was significant. In addition, potential correlates of 4 year smoking status (contemporaneous use of NRT, lifetime quit attempts, OTI alcohol and cannabis usage, functioning (physical, mental, general), symptoms, medication status and stage of change) were not significant.
Analysis of smoking-related data and changes in smoking status between 1 and 4 years
The left-hand columns of Table 2 report associations between treatment status and the individual smoking outcome variables at 1 year (n = 247), while the right-hand columns report associations at 4 years (n = 164). There was no evidence of a treatment effect on continuous or point prevalence abstinence. In addition, there were no statistically significant differences between treatment groups in smoking status at the 4 year follow-up assessment. The observed difference in point prevalence abstinence at the 1 year follow up between participants who attended all sessions and the comparison group (20.6% vs 9.2%, p = 0.03), however, may have clinical relevance to future treatment studies. At the 1 year follow up, there was a statistically significant dose-response pattern for participants allocated to the treatment condition. More than half (52.4%) of participants who attended all eight treatment sessions displayed a ≥50% reduction in smoking relative to their baseline, compared with one-quarter (24.2%) of the comparison group. This difference was not significant at 4 years (43.8% vs 35.8%, Table 2). Overall, as seen in Table 2, 78/247 (31.6%) had reduced their smoking by at least 50% at 1 year and 57/164 (34.8%) at 4 years. At 4 year follow up, those who reported that they had reduced their smoking by ≥50% had a 48.2% reduction in CO levels (from a mean of 22.71 p.p.m. (SD = 16.18) at baseline, to a mean of 11.76 p.p.m. (SD = 10.56) at 4 years). Those who reported abstinence at 4 years showed a decline in CO levels of 89.5% (from a mean of 22.26 p.p.m. (SD = 9.97) at baseline, to a mean of 2.35 (SD = 10.44) at 4 years).
Continuous and point prevalence abstinence rates and smoking reduction status at follow up
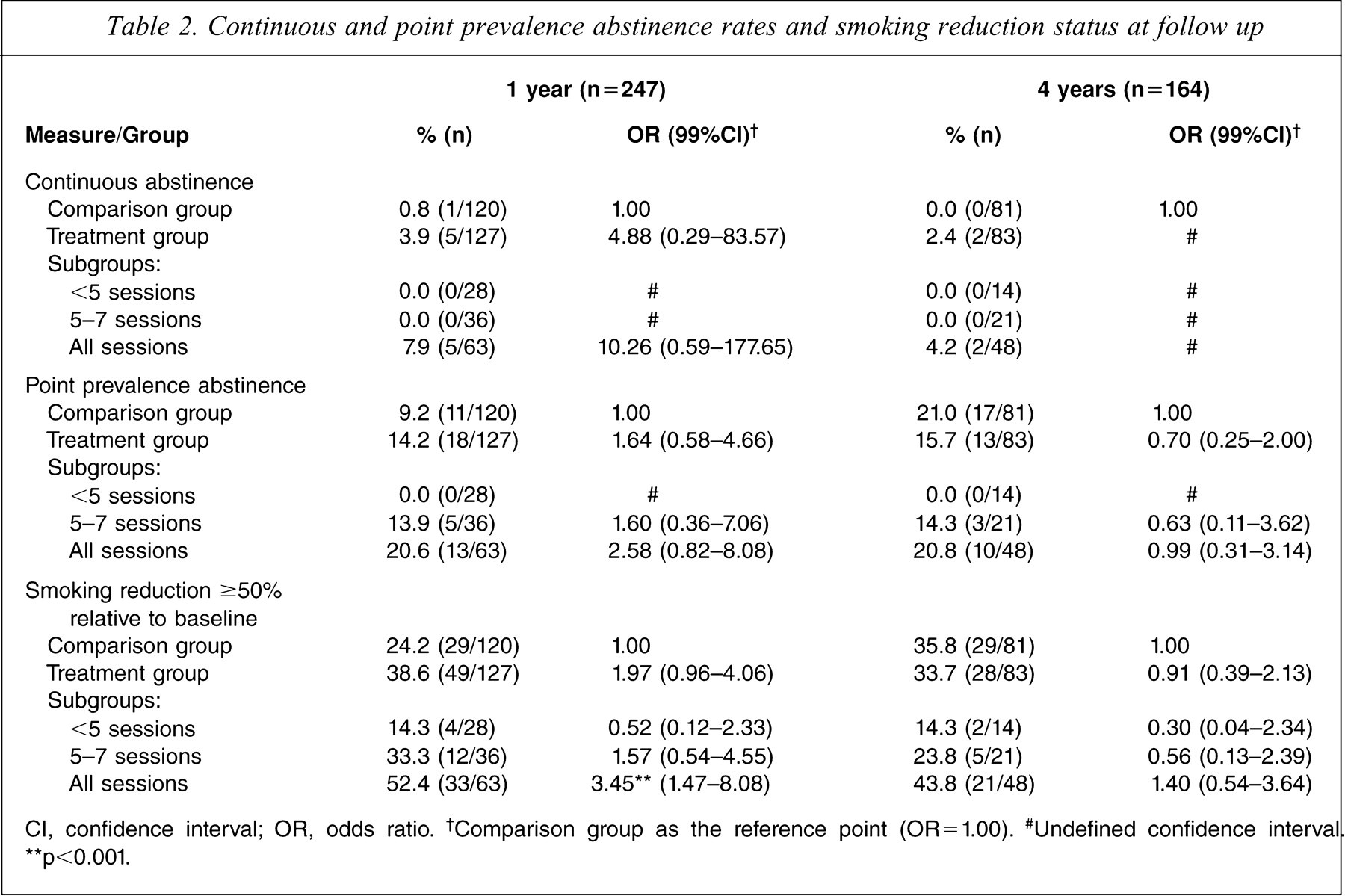
Cl, confidence interval; OR, odds ratio. †Comparison group as the reference point (OR = 1.00). #Undefined confidence interval ∗∗p<0.001.
As can be seen in Table 3, there were significant overall improvements between baseline and 1 year in terms of depression and mental functioning, and between baseline and 4 years in terms of state anxiety, depression and mental functioning. There were no significant differences between the 1 year and 4 year follow ups, nor any differential changes by treatment status.
Symptom and functioning profiles
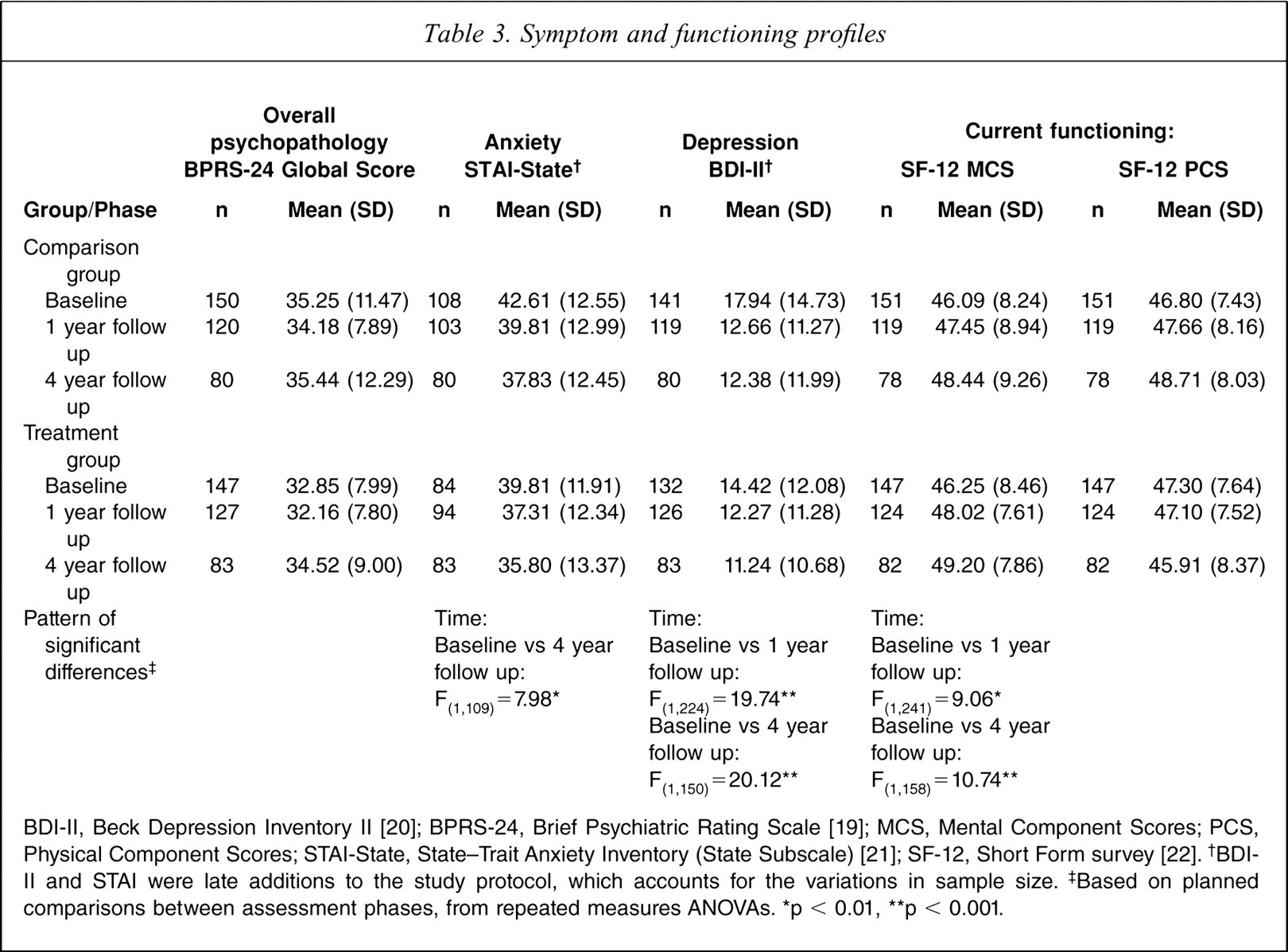
BDI-II, Beck Depression Inventory II [20]; BPRS-24, Brief Psychiatric Rating Scale [19]; MCS, Mental Component Scores; PCS, Physical Component Scores; STAI-State, State-Trait Anxiety Inventory (State Subscale) [21]; SF-12, Short Form survey [22]. †BDI-II and STAI were late additions to the study protocol, which accounts for the variations in sample size. ‡Based on planned comparisons between assessment phases, from repeated measures ANOVAs. ∗p < 0.01, ∗∗p < 0.001.
Table 4 reports a cross-tabulation of the overall smoking reduction status categories at the 1 and 4 year follow ups. As shown in the diagonal of Table 4, more than half (59.7%, 89/149) of the participants were placed in the same smoking reduction category at 1 and 4 years, while approximately one-fifth (19.5%, 29/149) had improved (above diagonal) and another fifth (20.8%, 31/149) had deteriorated (below diagonal; χ2 = 97.36, df = 9, p < 0.001). Table 4 also illustrates the patterns of change by reporting mean daily cigarette consumption at baseline and the 1 and 4 year follow ups.
Cross-tabulation of smoking reduction status at 1 and 4 year follow up (relative to baseline)
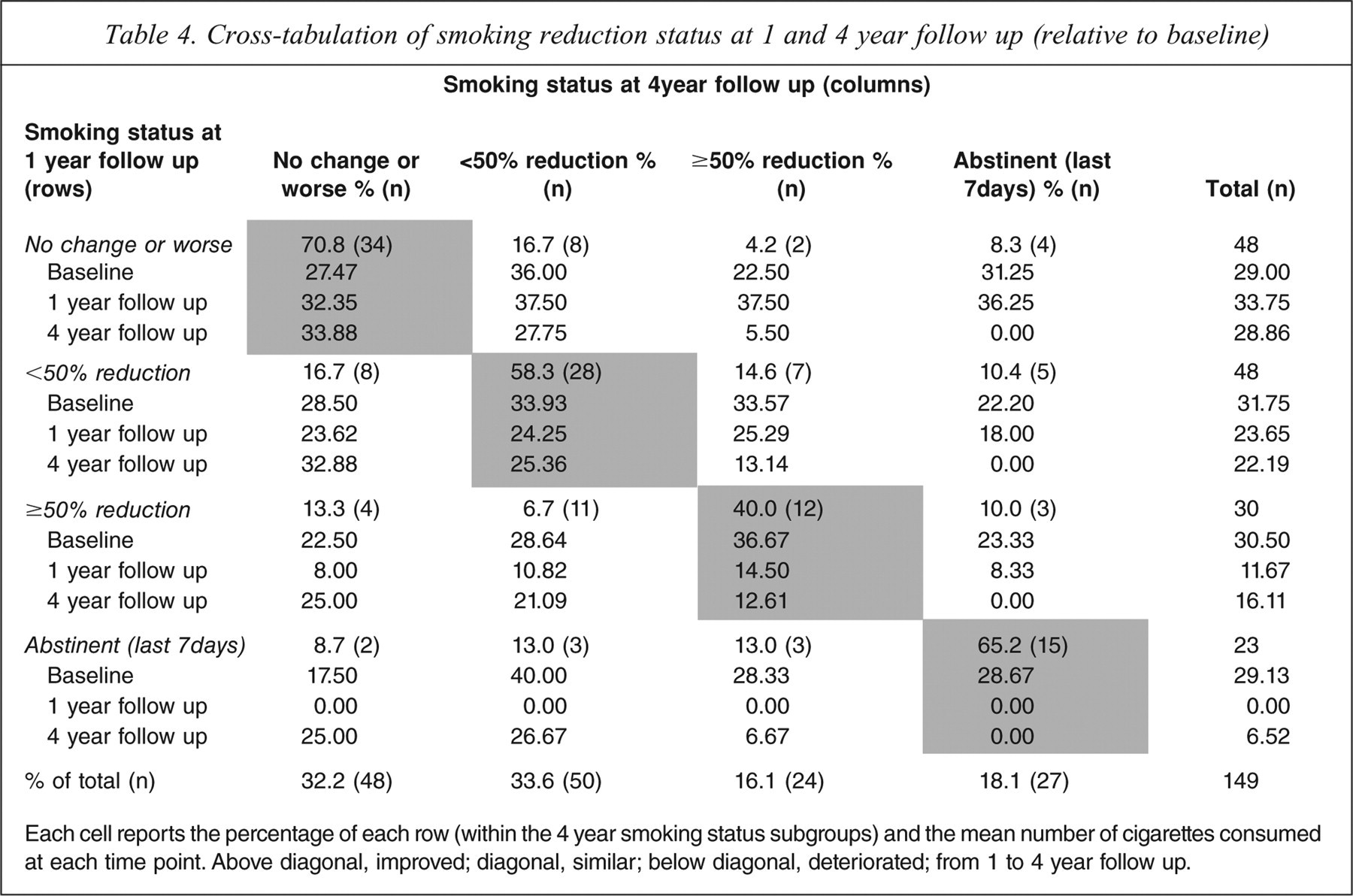
Each cell reports the percentage of each row (within the 4 year smoking status subgroups) and the mean number of cigarettes consumed at each time point. Above diagonal, improved; diagonal, similar; below diagonal, deteriorated; from 1 to 4 year follow up.
Most participants (70.8%, 34/48) who had not made any change in their smoking, or whose smoking had worsened between baseline and 1 year, remained in that category at 4 years, whereas most participants (84.6%, 66/78) who had made at least some reduction in their smoking between baseline and 1 year also reported at least some reduction in their smoking at 4 years. Of those who reported abstinence at 1 year, 93.2% (21/23) maintained at least some reduction in their smoking at 4 years. Abstinence from smoking at 1 year, rather than a reduction in smoking, was associated with point prevalence abstinence at 4 years: almost two-thirds (65.2%, 15/23) of those reporting point prevalence abstinence at 1 year, also reported abstinence at the 4 year assessment; whereas only 10.0% (3/30) of those who had reduced their smoking reported abstinence at 4 years (χ2 = 40.74, df = 3, p <0.001). Mean reported longest time without a cigarette in the year prior to the 4 year follow up (excluding continuously abstinent participants) was 253.40 days (SD = 139.32) for those reporting point prevalence abstinence, 53.52 days (SD = 105.74) for those reporting a ≥50% reduction, 8.19 days (SD = 17.51) for those reporting <50% reduction and 10.92 days (SD = 30.91) for those reporting no change or worse smoking (F = 72.17, df = 3,143, p<0.001). Only 8.7% (2/23) of those abstinent at 1 year reported continuous abstinence at 4 years. A total of 43.6% (61/140), however, recorded CO levels <10 p.p.m. at 4 years, indicative of a low likelihood of having smoked in the last 8 hr.
Discussion
In the present study, which is the first to report long-term (4 year) outcomes following a smoking cessation intervention among smokers with a psychotic disorder, more than three-quarters of the sample (79.2%, 118/149) reported maintenance or improvement in their smoking reduction status relative to their status at 1 year. This is an important clinical finding in that it suggests that smokers with a psychotic disorder are capable of long-term change in their smoking. Thus, clinicians can be assured that addressing smoking among people with psychosis is worthwhile and that reduction in smoking can be maintained in the longer term.
Where there had been a dose response to treatment on smoking reduction status (i.e. ≥50% reduction relative to baseline) at the 1 year follow up, treatment per se was not associated with smoking reduction status or abstinence at 4 years. This might be expected in that a 4 year period may be too long for an eight-session intervention to continue to exert an effect, and it has been suggested that more intensive and longer interventions may be needed to improve smoking cessation among people with psychotic disorders [1]. Etter and Stapleton recently suggested that, given the modest results of NRT at 12 month follow up, tobacco dependence could be better regarded as a chronic, relapsing condition that may require multiple doses of treatment [13]. Thus, the clinical implication is that smoking cessation treatment should be available on an ongoing basis to people with psychosis, in much the same way as other pharmacological interventions are, with ongoing monitoring and encouragement regarding compliance with NRT and behavioural interventions. Factors that impact on and enhance treatment adherence and retention require further research because there was a dose response to treatment in the initial study. In addition, new, more efficacious, treatments need to be developed.
The inability to identify variables associated with smoking status at 4 years suggests that other individual or systemic variables may potentially be associated with longer term smoking status. For example, it is possible that smoking may ameliorate impairments in sustained attention among people with schizophrenia [25,26]. In addition, systemic variables, such as policies regarding smoking in health service settings and the availability of healthy lifestyle programs, may influence longer term outcomes [27]. Systemwide policies involving the introduction of smoke-free environments, with appropriate NRT and counselling support for staff and patients, may also enhance responses to smoking cessation interventions aimed at individual behaviour change [1].
The present study was also one of the first to investigate whether smoking reduction status was associated with later quitting among smokers with a psychotic disorder. The finding that smoking reduction status did not increase the probability of later quitting is contrary to the conclusion drawn in a literature review by Hughes and Carpenter, who reported that smoking reduction increased the probability of future cessation in the general population [3], and contrary to the results of the small study among people with schizophrenia conducted by Evins et al. [4]. The finding in the present larger study that abstinence at 1 year was associated with abstinence at 4 years suggests that, when possible, interventions should continue until abstinence is achieved. In the context of smokers with psychotic disorders, interventions may be more effective if there is enough flexibility to allow continued sessions, in the event of delayed quit attempts, and the resumption of sessions following lapses in motivation to quit [1]. Although continuous abstinence was very rarely seen in the present study, it is apparent that lengthy periods of abstinence are attained from time to time by those assessed as currently abstinent, or who have reduced their smoking by ≥50% at a single time point, in this case, 4 years. It seems that treatment providers will need to be prepared to discuss coping with lapses and relapse prevention strategies with smokers with a psychotic disorder, realistically addressing a fluctuating course in the process of quitting smoking. Although reduced smoking at 1 year was not associated with abstinence at 4 years in the present study, nor was it associated with relapse to a previous higher level of smoking. Those who reported at least halving their smoking at 4 years were smoking fewer than 15 cigarettes per day, on average (Table 4), which was the threshold for entry into the initial study [11]. West has pointed out that if smokers who resume smoking (after a course of treatment) receive an advantage from a subsequent course, over repeated courses the aggregate effect will be greater [28].
Recently, Fernander et al. proposed a biopsychosocial framework for examining health disparities, including smoking, lifestyle factors (diet, weight, physical exercise and alcohol consumption) and psychosocial and occupational/environmental issues [29]. In a small pilot trial of a smoking and lifestyle intervention among people with psychoses we have demonstrated the potential utility of directing motivational interviewing and CBT concurrently to a range of health-related behaviours among people with psychoses [30]. A large randomized controlled trial of this healthy lifestyle intervention is currently under way. Apart from offering additional treatments, with the aim of cessation among smokers who resume smoking, further longitudinal studies are needed to determine the course of smoking among people with severe mental health problems and whether smoking reduction has health as well as economic benefits. Although studies of the health consequences of reduced daily cigarette consumption among heavy smokers have not yielded clear evidence of physical health benefits [5], the present results suggest that reductions in smoking over a 4 year period are not detrimental to mental health among people with psychotic disorders. Smoking cessation could also facilitate usage of lower doses of antipsychotic medication [31].
The major limitation of the present study was that only 164 people attended the 4 year follow up, with only 149 of these attending at both 1 and 4 years, resulting in a follow-up rate of 60.3%. Although no differences were detected between those followed up and those not followed up, there may be unknown variables that limit the representativeness of the obtained sample. Retention rates would probably have been improved if the 4 year follow up had followed annual follow ups, with contact details being revised regularly. Notwithstanding, the present study provides the largest long-term profile of smoking, symptomatology and general functioning among smokers with a psychotic disorder.
Conclusions
Few studies have provided information on smoking and clinical profiles following smoking cessation intervention among people with psychosis. We assessed smoking, symptom and functioning profiles among 164 people, 4 years following recruitment into a smoking cessation study. More than three-quarters of the sample reported maintenance or improvement in their smoking reduction status relative to their status at 1 year. Therefore, whether or not the smoking outcomes achieved are attributable to the specific interventions provided, longer term change may be possible, with associated health and financial benefits. We hope that these results will encourage clinicians working with people with psychotic disorders to address and monitor smoking during treatment for psychosis, with an emphasis on harm reduction benefits and a view to eventual smoking cessation.
Footnotes
Acknowledgements
The initial study was a joint project conducted by the Centre for Brain and Mental Health Research (University of Newcastle and Hunter New England Mental Health) and the University of NSW. Funding was provided by the National Health and Medical Research Council (grant number: 141708), Rotary, and Community Health and Tuberculosis Australia. NRT was provided free of charge by GlaxoSmithKline. Self-help booklets were provided at a discounted price by SANE Australia. Funding for the 4 year follow up was provided by the Commonwealth Department of Health and Human Ageing. We wish to thank all of the participants and the various agencies and health professionals who assi sted with recruitment, including the SRI Schizophrenia Research Register. Thanks also to our academic colleagues (Vaughan Carr and Kay Wilhelm) and to the research staff at the University of Newcastle (Lisa Phillips, Melanie Haile, Louise Thornton and Vanessa Clark) and the University of NSW (Rachel Taylor, Sylvia Jansons, Caitlin McCue, Amber de Lucia and Shiraze Bulsara).