
Abstract
Keywords
Attention-deficit–hyperactivity disorder (ADHD) has been recognized as a chronic disorder with high psychiatric comorbidity, persistence of core symptoms, and long-term impairment lasting to adolescence and adulthood [1–3].
Differential persistence rates of ADHD into adolescence, ranging from 22–43% to 80–85% across several longitudinal follow-up studies [2,4–6], might be partly explained by the definition of remission [7], and the use of ascertainment criteria, with the lowest rates associated with the use of the DSM-II diagnostic criteria of hyper-kinetic disorder, and the highest rates with the use of the DSM-III-R criteria of ADHD [8]. Regarding the definition of remission proposed by Biederman et al. [7], persistence rates of ADHD at age 25 are around 15% according to the syndromatic persistence criteria, and up to 65% according to the symptomatic persistence criteria [9]; but the rate of functional remission is low at adolescence and young adulthood [7]. Insufficient sensitivity of the DSM to identify the developmental change of ADHD symptoms makes it difficult for children with ADHD to meet diagnostic criteria as they age [9]. Therefore, adolescents or adults having functional impairments but only partial DSM-IV symptoms may not be diagnosed as having ADHD [10]. Use of the dichotomous approach to estimate the diagnostic retention rate and to investigate the associated problems of ADHD might be insufficient, but using the dimensional approach to examine symptomatic changes over time may help in the understanding of the developmental course of ADHD [11].
Western follow-up studies among children with ADHD have demonstrated a decline in hyperactivity, quality change in impulsivity, and persistence of inattention at adolescence and adulthood [7,12]. Persistence of ADHD may contribute to increased comorbid conditions [4,13], as well as academic and social impairments [3,4,14]. A small number of similar studies using Asian subjects have found that the prevalence rate of ADHD according to the DSM-IV diagnostic criteria at grade 7 (7.5%) decreased at grade 9 (3.3%) in Taiwan [15], that approximately 70% of hyperactive children assessed in 1979 continued to manifest typical symptoms 15 years later in China [16], and that high psychiatric comorbid conditions were demonstrated in Taiwanese and Japanese children with ADHD [1,17].
Parents and adolescents often disagree in their reports on the presence or severity of behavioural problems, with low–moderate parent–child agreement in most studies [18,19]. Kashani et al. reported that children and adolescents often report fewer problems of hyperactivity and inattention than their parents [19], a finding not supported by Verhulst and van der Ende [18]. Moreover, children reported more internalizing problems whereas parents reported more externalizing problems [20,21]. Knowledge about different perceptions of the child's symptoms between parents and youths is needed to enhance integration of information from both informants in clinical practice and research of child mental problems/disorders. Despite some Western studies on this important topic, however, no such study has been reported in Asian populations.
The high prevalence of DSM-IV ADHD worldwide and in Taiwan as well [15], and the long-term impact of ADHD on the individual, family, and society reported in Western studies [22,23], warrant investigation to enhance understanding of symptom persistence and psychiatric outcome of ADHD longitudinally in a non-Western population. The current study examined the symptoms that continue to manifest at adolescence in terms of inattention, hyperactivity, and impulsivity, the proportion of persistent ADHD, the psychopathology, and the mother–child agreement on reporting ADHD symptoms at adolescence among children with ADHD in Taiwan. We anticipated that children with ADHD were more likely to have comorbid psychiatric disorders and persistent ADHD symptoms, particularly based on maternal report, at adolescence.
Methods
Participants
The clinical sample included 93 11–16-year-old youths with ADHD (77 boys and 16 girls with a ratio of 4.8; mean age= 13.2 ± 1.5, who were clinically diagnosed with DSM-IV ADHD at the age of 7.3 ± 2.8 years at the Children's Mental Health Center, National Taiwan University Hospital, Taipei, Taiwan based on medical records. These clinical participants were observed to have overt ADHD-related symptoms at the mean age of 4.5 ± 1.5 years, based on maternal interviews, There were 116 eligible patients, whose full-scale IQ was >80, who had complete contact information, and who met the DSM-IV diagnostic criteria for ADHD as assessed clinically for at least three clinic visits in 1997 and 1998. Given that 23 refused follow-up assessments, 93 patients completed the assessments (participation rate, 80.2%). The baseline clinical diagnoses of ADHD and other psychiatric disorders were further confirmed by psychiatric interviews of the participants and their mothers using the Chinese version of the Kiddie epidemiologic version of the Schedule for Affective Disorders and Schizophrenia (K-SADS-E) in 2003 or 2004.
More than half of the fathers (60.2%) and nearly half of the mothers (47.8%) had college degrees or higher educational levels (Table 1). More than 90% of patients lived with both parents. The DSM-IV diagnostic distributions (Table 1) for the case group at baseline were 53 with combined type (ADHD-C, 57.0%), 26 with inattentive type (ADHD-I, 28.0%), and 14 with hyperactive–impulsive type (ADHD-HI, 15.0%). A total of 86.0% of participants had taken immediate release (IR) methylphenidate for the treatment of ADHD in a wide range of treatment duration (range=1–96 months) and 61.3% were currently being treated with IR methylphenidate (Table 1).
ADHD subject characteristics
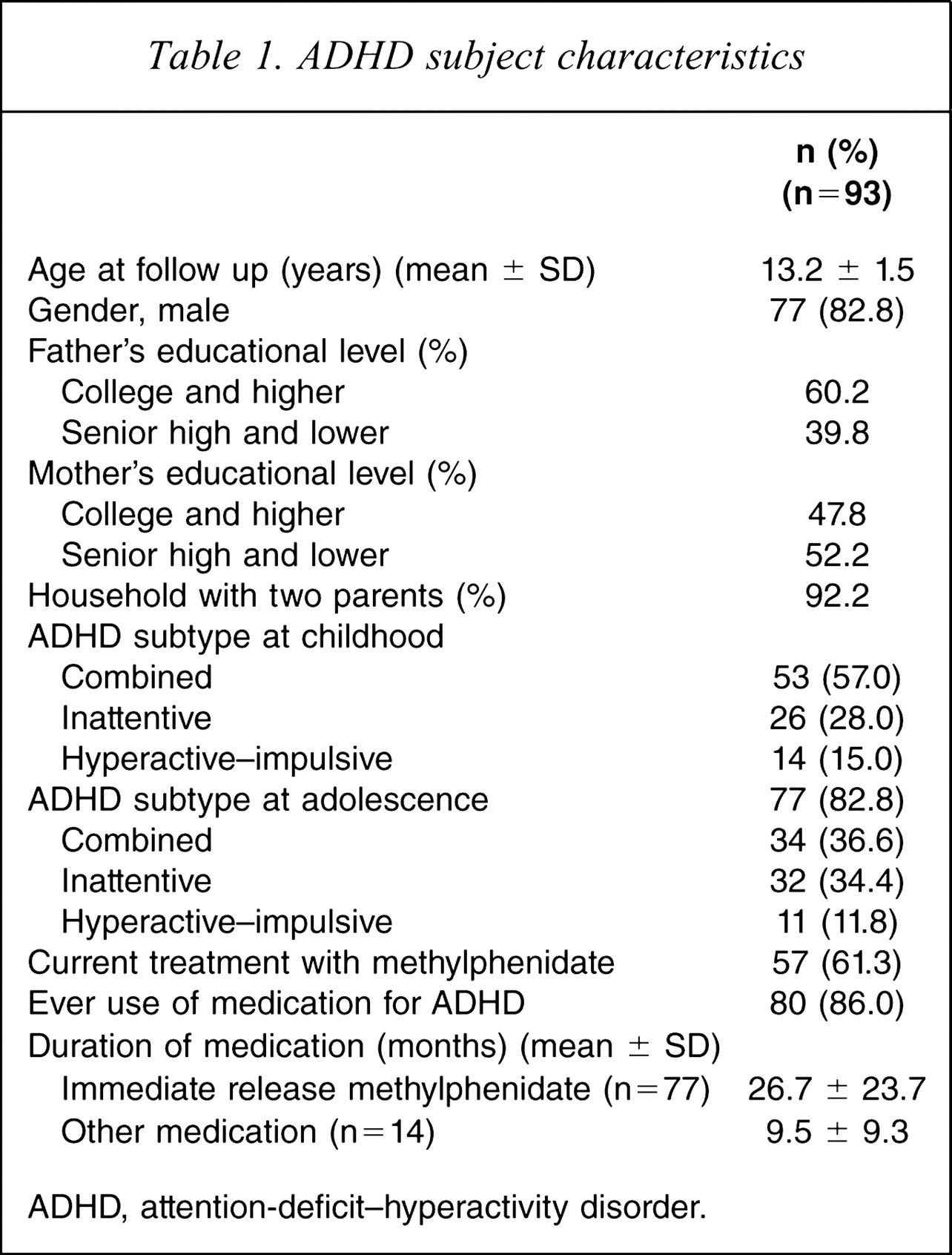
ADHD, attention-deficit–hyperactivity disorder.
The comparison sample consisted of 93 school controls, aged 11–16 years, without lifetime DSM-IV ADHD, who were matched for sex, age, and parental educational levels and were recruited from the same school districts of the ADHD group. The school controls were assessed to have no ADHD diagnosis at the age of 6–8 years, and at adolescence using the Chinese K-SADS-E at the mean age of 13.3 ± 1.4 years.
Measures
Chinese version of the K-SADS-E
The K-SADS-E is a semi-structured interview scale for systematic assessment of both past and current episodes of mental disorders in children and adolescents [24]. The Chinese K-SADS-E was prepared by the Child Psychiatry Research Group in Taiwan [25]. This included a two-stage translation and modification of several items with psycholinguistic equivalents relevant to the Taiwanese culture, and further modification to meet the DSM-IV diagnostic criteria [15]. Previous studies have shown that the Chinese K-SADS-E is a reliable and valid instrument to assess child psychiatric disorders and has been used extensively in a variety of studies on childhood mental disorders in Taiwan [26,27]. In the present study the internal consistency (Cronbach α) for the three dimensions of ADHD was good for adolescent interviews (a=0.60 for impulsivity at school and follow up, α= 0.86 for inattention at home and baseline) and was satisfactory for mother interviews (α=0.78 for impulsivity at school and follow up, α= 0.92 for inattention at school and baseline). The internal consistency of the total scores of the ADHD section in the Chinese K-SADS-E was satisfactory, ranging from 0.90 to 0.94.
Interviewer training
Two interviewers (YC Lai and HY Luo) who majored in psychology and psychiatric nursing had received 1 year full-time intensive clinical and research training in child and adolescent psychiatry before the interview training in use of the Chinese K-SADS-E by the authors. The two interviewers reached 98.25 ± 1.91 agreement of all mental disorders assessed by the Chinese K-SADS-E against the rating of each item in the K-SADS-E by SS Gau for 30 clinical subjects before implementation of the present study. Their K-SADS-E interviews of parents and children at follow up were audiotaped periodically and monitored by SS Gau, who was blind to the personal information of the participants, to ensure the quality of interviews. Twelve of 93 children, who were clinically diagnosed with ADHD according to the DSM-IV diagnostic criteria in 1997–1998, also completed the Chinese K-SADS-E to confirm the diagnosis of ADHD at the same time. Agreement for all the 18 baseline ADHD symptoms between the baseline assessments and retrospective assessments using the Chinese K-SADS-E interview among the 12 participants reached >90% for each behavioural symptom.
Best-estimate diagnoses
The first author, SS Gau, who was blind to the diagnostic status and name of the participant and was not involved in the direct K-SADS-E interviews of any of the participants or their parents at follow up, made all the best estimates of each psychiatric diagnosis according to the data from the K-SADS-E interviews of the participants and their mothers [1], medical records, and other self-administered questionnaires reported by the participants, parents, and teachers. The diagnostic coding was categorized into definite (meeting all DSM-IV diagnostic criteria including functional impairment), probable (either not meeting all DSM-IV symptoms criteria but more than half or no functional impairment), possible (some symptoms but no impairment), and no diagnosis [28]. Those patients who received a rating as definite or probable by best estimate were categorized as having a particular mental disorder.
Procedures
This study was approved by the Research Ethics Committee of National Taiwan University Hospital prior to implementation. We obtained written informed consent from the participants and their parents after detailed explanation of the purpose and procedure of the study and reassurance of confidentiality. They were also informed clearly that there was no obligation to participate in this study, and participation choice would not influence clinical practice. Participants and their mothers were interviewed independently by two separate interviewers to confirm the child diagnosis of ADHD in 1997–1998 for the ADHD group and the non-diagnosis of ADHD for the controls using the Chinese K-SADS-E. Subsequently, all the participants and their mothers were interviewed using the Chinese K-SADS-E to determine psychiatric diagnosis at follow up (past 6 months) in 2003–2004. The interviewers were blind to the case/control status.
Statistical analysis
We performed the data analysis using SAS 9.1 (SAS Institute, Cary, NC, USA). The pre-selected alpha was at the p < 0.05 level. The descriptive results are displayed as frequency and percentage and compared by χ2 test; for continuous variables, mean and SD and analysis of variance are shown.
Given the matched case–control study design, a multi-level model with random and fixed effects was used to address lack of independence within the matched case–control pairs to compare the ADHD symptoms at home and school settings between the two groups. For the comparisons of ADHD symptoms between baseline and follow up and between child and mother reports, we further adjusted the repeated measures within the same participants using a linear multi-level model. Cohen's d was used to compute the effect size (standardized difference between the two means) for the group comparisons. The effect sizes are defined as small, medium, and large for Cohen's d in the range of 0.3 - <0.5, 0.5 - <0.8, and > = 0.8, respectively [29]. We used conditional logistic regression to compare the rate of psychiatric disorders between the two groups, and to calculate the odds ratio (OR) and 95% confidence interval (CI).
Results
Difference in ADHD symptoms
The ADHD group significantly scored higher in symptoms of inattention, hyperactivity, and impulsivity at both home and school settings, at both baseline and follow up, and based on youth and mother interviews with very large effect sizes (Tables 2, 3). These significant differences between adolescents with and without ADHD at childhood were not modified by sex or age (all p > 0.05).
ADHD symptom severity
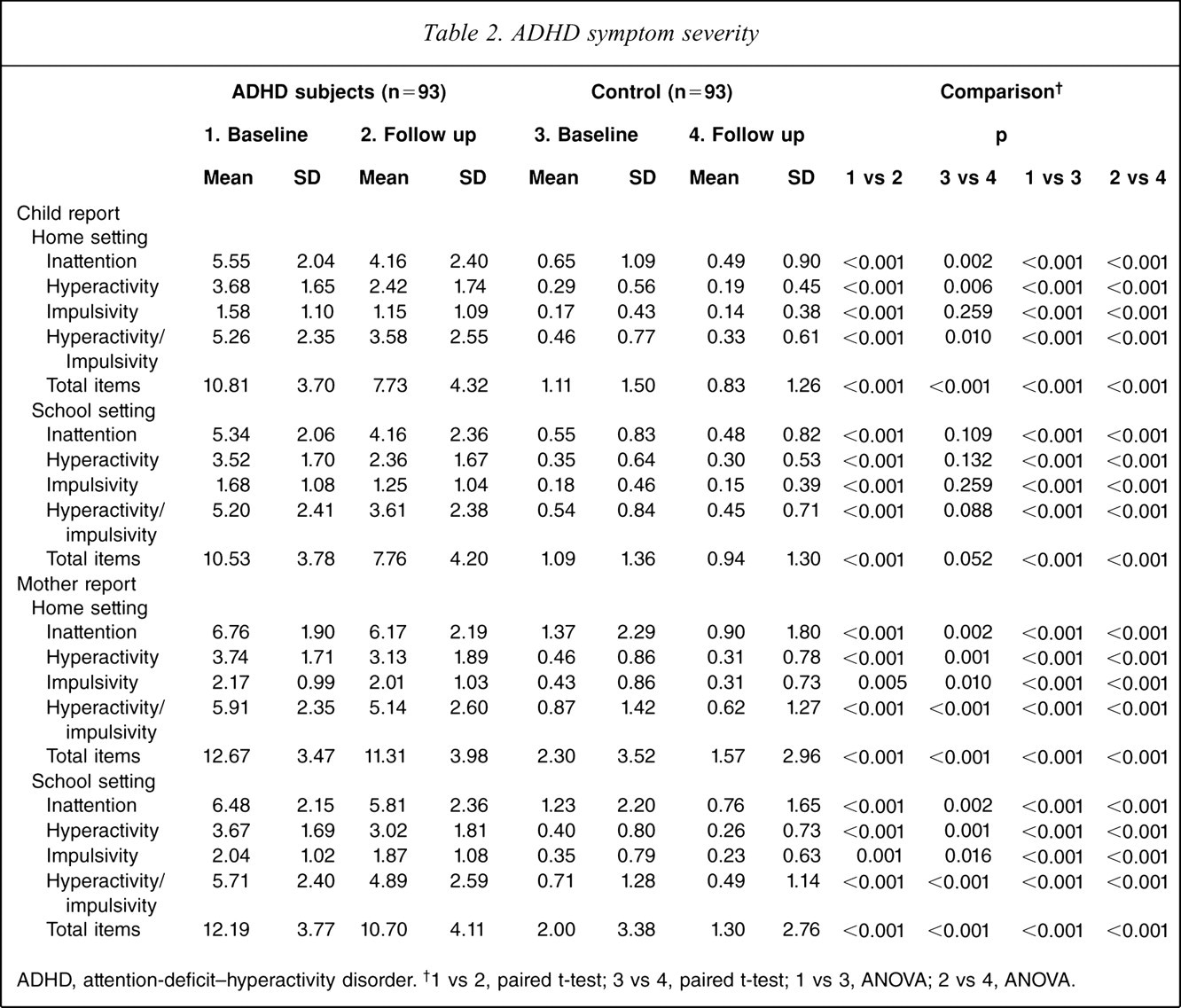
ADHD, attention-deficit–hyperactivity disorder. †1 vs 2, paired t-test; 3 vs 4, paired t-test; 1 vs 3, ANOVA; 2 vs 4, ANOVA.
Effect sizes (Cohen's d)
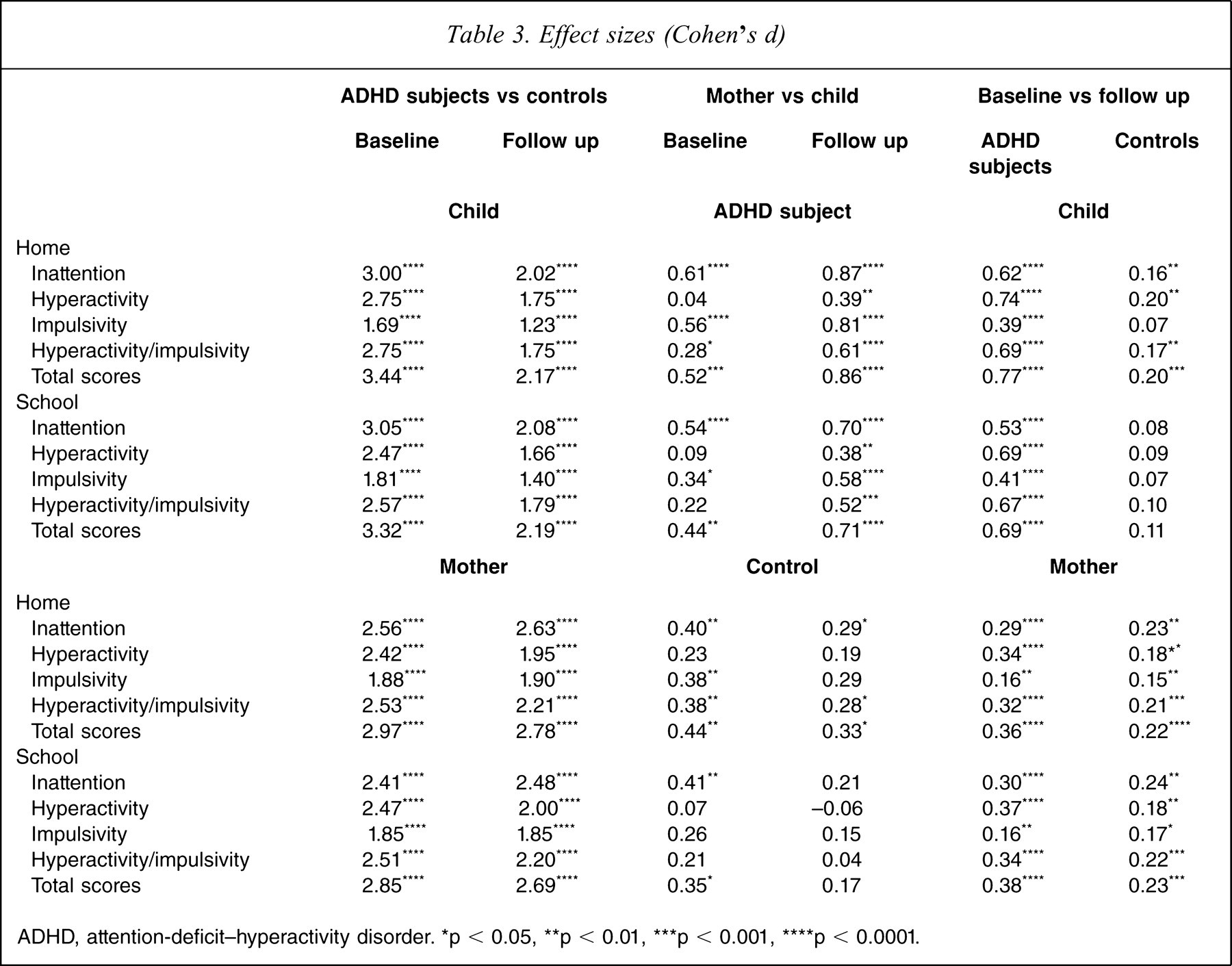
ADHD, attention-deficit-hyperactivity disorder. ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001, ∗∗∗∗p < 0.000l
Symptom changes at follow up
According to the Biederman et al. definition of remission [7], the prevalence rates of syndromatic remission, symptomatic remission, and functional remission at adolescence were 50.5%, 17.2%, and 3.2%, respectively.
The ADHD group demonstrated significant improvement in these three behavioural dimensions over time with medium effect size, except for impulsivity (home, d = 0.39; school, d = 0.41) in both settings based on the youth interviews, but small effect size for all ADHD symptom dimensions in both settings based on mother interviews (Table 3). Similarly, the controls also had reductions in these ADHD symptoms based on mother interviews although with very small effect sizes; but only significant improvement in inattention and hyperactivity over time at the home setting was noted, however, based on youth interview (Table 3).
Regarding modifying effects from sex, ADHD, or informants, we found that the magnitude of improvements over time was significantly greater in the ADHD group than the control group (p < 0.001) based on youth interviews. According to the mother interviews, the magnitude of reduction in hyperactivity over time was significantly greater in the ADHD group than in the controls in both home (p < 0.001) and school (p < 0.001) settings. The reduction in youth-reported symptoms was greater than that of mother-reported symptoms for the ADHD group regarding inattention (home, p < 0.001; school, p = 0.019), hyperactivity (home, p < 0.001; school, p = 0.009), and impulsivity (home, p = 0.002; school, p = 0.007). The magnitude of symptom reduction did not differ between girls and boys except that boys reported greater reduction in hyperactivity from baseline to follow up in school settings than did girls (β = 0.471, F = 5.43, p = 0.012).
Mother–child Agreement on reporting ADHD symptoms
We found that the mother–child agreement on reporting ADHD symptoms was moderate at baseline intraclass correlation (ICC = 0.44–0.71) and small-moderate at follow up (ICC = 0.32–0.56). Mothers tended to report more severe ADHD symptoms in their children than their children reported for themselves at baseline with small–medium effect sizes except hyperactivity (home, d=0.04; school, d = 0.09), and at follow up with medium–large effect sizes except hyperactivity (home, d = 0.39; school, d = 0.38; Tables 2,3). These discrepancies were significantly more obvious in boys than in girls at both assessments (p = 0.013–<0.001) and in the ADHD group than the controls at follow up (p=0.003–<0.001) except for hyperactivity (p > 0.05). There was no difference in the magnitude of mother–child difference between the ADHD and control groups at baseline (all p > 0.05).
Psychopathology at follow up
At adolescence, 46 (49.5%) met full criteria of DSM-IV ADHD, 31 (33.3%) had more than half of the required symptom items of ADHD, and 16 (17.2%) had only a few symptoms remaining. Among the 77 adolescents (combining full diagnosis and subthreshold diagnosis), the number of subjects in the ADHD-C, ADHD-I, and ADHD-HI groups was 34 (36.6%), 32 (34.4%), and 11 (11.8%), respectively (Table 1). Of 53 children with ADHD-C, 29 (54.7%) maintained ADHD-C, 16 (30.2%) changed to ADHD-I, two (3.8%) changed to ADHD-HI, and six (11.3%) did not reach ADHD diagnosis at adolescence. Of 26 children with ADHD-I, 16 (61.5%) maintained ADHD-I, three (11.6%) changed to ADHD-C, and seven (26.9%) did not reach ADHD diagnosis at adolescence. Of 14 children with ADHD-HI, eight (57.1%) maintained ADHD-HI, three (21.4%) changed to ADHD-C, and three (21.4%) did not reach ADHD diagnosis at adolescence. The weighted kappa for the agreement of ADHD subtypes at baseline and follow up among the 77 adolescents with ADHD was 0.50 (95%CI= 0.31–0.68).
Compared to the controls, children with ADHD were more likely to develop oppositional defiant disorder, conduct disorder, mood disorders (mainly major depression and bipolar disorders), and sleep disorders at adolescence (Table 4).
Psychiatric diagnoses at adolescence vs presence of ADHD
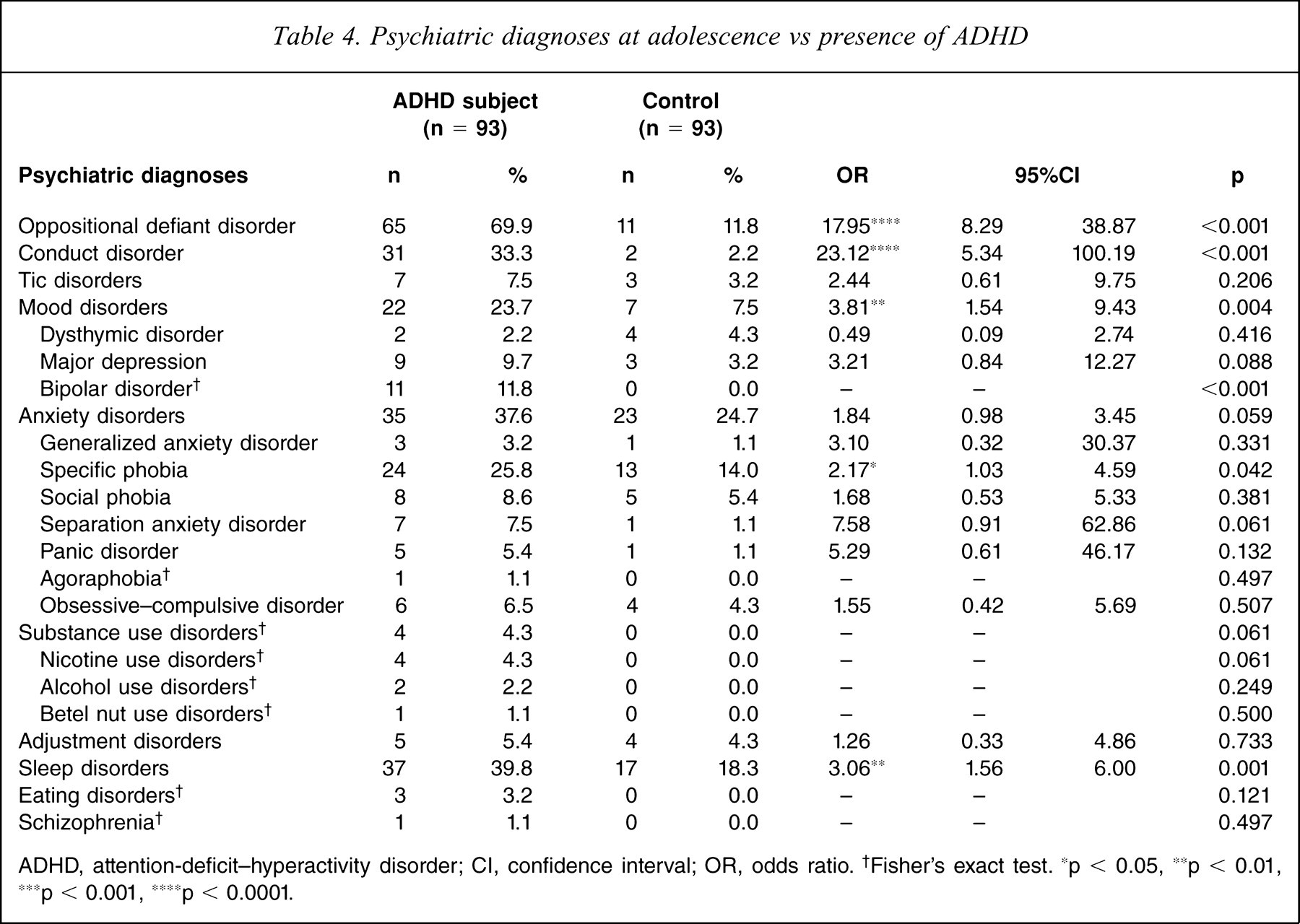
ADHD, attention-deficit-hyperactivity disorder; CI, confidence interval; OR, odds ratio. †Fisher's exact test. ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001, ∗∗∗∗p < 0.0001.
Discussion
Parallel to several longitudinal follow-up studies of children with ADHD at adolescence and adulthood conducted in Western society [4,7,9,12], the present study provides the first data on the changes of DSM-IV ADHD symptoms and psychiatric outcomes at adolescence in an ethnic Chinese population. The major findings were significant reductions in all three domains of ADHD symptoms at a different pace (greater magnitude of symptom reduction in inattention and hyperactivity than impulsivity) in all children, greater improvement but persistently more severe ADHD symptoms at adolescence among children with ADHD than the controls, higher rate of psychiatric comorbidities associated with ADHD, and increasing mother–child disagreement on reporting ADHD symptoms as children aged, especially among boys and children with ADHD.
Slightly lower rates of ADHD diagnosis retention in the present study than in several previous studies may be explained by different diagnostic criteria and sample sources [11]. Compatible with Western findings of ADHD symptom decline as a function of age [7,12,30], the present data showed significant decline of three core symptoms over time among both groups, suggesting that symptom decline was not influenced greatly by different ethnicities, cultures, and educational environments. More severe ADHD symptoms at adolescence in children with ADHD as compared to normal adolescents regardless of greater magnitude of symptom reductions, has lent evidence to support the persistence of ADHD symptoms into adolescence [2,6,30]. Greater symptom reduction in the ADHD group than the controls might be explained by regression to the mean [12], the ground effect of the measurement for the controls, the possibility of outgrow of ADHD [31], or a decrease of ADHD symptoms under treatment with time [28,32]. In addition, lack of the developmental sensitivity of the DSM-IV criteria to the variations of ADHD symptoms in adolescence and adulthood may lead to underestimation of symptoms in adolescence [9]. Further investigations to clarify the developmental difference of persistence and remission of ADHD symptoms will help establish age-appropriate diagnostic criteria and define the subgroup that needs more intensive interventions.
Similar to several cross-sectional studies showing ADHD symptom reductions over time [7,11,12,30,33], but unlike those studies showing more pronounced developmental reduction in hyperactivity–impulsivity symptoms than inattentive symptoms in normal children [11,30] and children with ADHD [7,12,33], we found that the magnitude of hyperactive symptom reductions was only slightly higher than that of inattentive symptom. These discrepant findings can be explained by different diagnostic criteria (DSM-III-R) [7,12] and older ages at follow up in previous studies [33]. Due to only one follow-up assessment at age 13 in the present study, we were not able to observe more obvious symptom reductions in hyperactivity–impulsivity than in inattention [12]. The present findings lend evidence to support that inattention and hyperactivity–impulsivity symptom reductions are more obvious among children with ADHD than normal controls [30].
Consistent with previous studies [12,34], the present results also demonstrate a higher proportion of ADHD-C at childhood than ADHD-I and ADHD-HI, and decreasing ADHD-C proportion at adolescence. The developmental symptom change is considered to contribute partly to the subtype switch [35]. The agreement of ADHD subtypes between childhood and adolescence (k=0.50) is higher than in other studies (11.1–24.0%) [33]. Although the present results did not show much greater symptom reduction of hyperactivity–impulsivity than inattention, more patients with ADHD-C were re-classified to ADHD-I than to ADHD-HI, and there was an increased ADHD-I proportion at adolescence. A similar magnitude of symptom reductions and fewer average numbers of hyperactive–impulsive symptoms than inattentive symptoms may cause some participants to have fewer than, but close to, six hyperactive–impulsive symptom items and more than six inattentive symptom items at adolescence.
To the best of our knowledge, the present study is among the few studies to evaluate mother–child agreement on reporting ADHD symptoms using the DSM-IV diagnostic criteria and psychiatric interviews [30,36]. The present findings lend evidence to support greater ADHD symptom reductions reported by youth than their mothers [20,30], and also demonstrated more ADHD symptoms reported by mothers than the youth using the Chinese version of the K-SADS-E [36]. In summary, several lines of data, including the present data, suggest that mothers are superior over their children in reporting ADHD symptoms with regard to accuracy and ADHD diagnosis [11,37].
Consistent with some [18] but contradictory to others [20,21], decreased mother–child agreement of ADHD symptoms with age was noted in the ADHD group rather than the controls. These findings suggest that adolescents with childhood diagnosis of ADHD tend to view their symptoms as less severe than their mothers. Among 18 ADHD symptoms evaluated in the Chinese version of the K-SADS-E, the most discrepant symptom between mother and child reports at both baseline and follow up was ‘having difficulty organizing tasks and activities’ (k=0.05–0.1). This discrepancy could partly be explained by different perception and expectation of organization ability from the participants and the mothers because of the over-involvement of Taiwanese parents in preparing and scheduling for their children's daily activities and academic learning. The greatest decline in the mother– child agreement was the symptom ‘fidgeting with hands or feet or squirming in seat’ (k=0.6 at childhood and 0.3 at adolescence), suggesting greater discrepancy in perception and tolerance of minor extremities and body movements between adolescents with ADHD and their parents.
Consistent with previous studies [2,26,38,39], the findings suggest that children with ADHD have increased risks of oppositional defiant disorder, conduct disorder, mood disorders and sleep disorders at adolescence. Contrary to others [2,4,26], we did not find an association of substance use disorder with ADHD, which can be partially explained by relatively small sample size, selection bias (subjects from Taipei City only), young age at follow up and low prevalence of adolescent substance use disorder in urban Taiwan [15]. We also failed to find a reduction in any anxiety disorder among the ADHD group [39,40], except for the specific phobia. The prevalence of anxiety disorders among the ADHD group was similar to that in other Western studies [40]. The novel finding of the association between specific phobia and ADHD at adolescence is supported by a recent study in Taiwan [1], which suggested the side-effect of anxious and phobic symptoms in long-term use of methylpheni-date [41]. Further investigation is warranted to delineate the underlying mechanism of the association between specific phobia and ADHD.
Surprisingly, the present advanced analysis did not find that ever (p=0.132–0.956 for child report, 0.254– 0.995 for mother report) and current (p=0.463–0.986 for child report, 0.740–1.000 for mother report) treatment with methylphenidate had effects on ADHD symptom reductions over time. The present findings are in line with those of Hart et al. that treatment had no effect on symptom change [12], and those of the MTA study that the earlier advantage of medication treatment was no longer apparent by 36 months [42]. These negative findings may probably be due to age-related symptoms declines or the change of treatment intensity. In addition, children with more disruptive behaviours, which are associated with persistent ADHD [4,6,12], may need pharmacotherapy [30].
Limitations
The major methodological limitations of the present study were the relatively small sample size, clinically referred subjects, questionable generalization, retrospective K-SADS-E (Chinese version) interviews to confirm clinical diagnoses of ADHD at baseline and to assess the psychiatric diagnosis including ADHD of the controls approximately 6 years before recruitment, only one follow-up assessment at adolescence, and no information about treatment adherence. Several features of the sampling require the findings to be interpreted with caution, such as recruitment of patients with ADHD from a medical centre, higher parental educational levels, nearly all patients living with both parents, inclusion criteria of full-scale IQ .80, and higher rate (86%) of treatment with methylphenidate than the estimated rate in a population-based study in the USA (77.3%) [28].
Several strengths of the study include complete psychiatric interviews of the participants and mothers at baseline and follow up, complete medical data of treatment history, and being the first study in an Asian population to address DSM-IV ADHD symptom changes at adolescence among children with ADHD and to examine the mother–child agreements on reporting ADHD symptoms.
Clinical implications
The findings suggest that even under methylphenidate treatment sometime during their childhood, a large proportion of children with ADHD may still have severe core symptoms meeting DSM-IV diagnoses of ADHD at adolescence. Therefore, psychiatrists need to carefully re-assess ADHD symptoms and psychiatric comorbid conditions among adolescents with a childhood diagnosis of ADHD because of the persistence of ADHD, changes of ADHD subtypes, and high psychiatric comorbidity at adolescence. Identifying factors affecting the persistence of ADHD and the development of other psychiatric disorders at adolescence will be the next step for planning of intervention. Finally, combining several lines of data, the present study strongly suggests that maternal reports and child reports are important to make the diagnosis of ADHD and to measure ADHD symptom changes over time.
Footnotes
Acknowledgements
This work was supported by grants from the National Science Council (NSC91-2314-B-002-223) and the Academic Sinica (IBMS-CRC92-T06). The preparation of this manuscript was supported by the National Health Research Institute (NHRI-EX94-9407PC), Taiwan (Clinical Trials. gov number: NCT00417781).