
Abstract
Eating disorders (anorexia nervosa (AN), bulimia nervosa (BN) and eating disorders not otherwise specified (EDNOS)) are psychiatric disorders in which intense preoccupations with food, eating, and restriction of food and eating, are characteristic [1,2]. Although individuals with eating disorders (EDs) spend much time reading about nutrition and may appear to have a good knowledge of nutrition, the knowledge tends to be selective and skewed towards the aspects that maintain the ED and they do not necessarily have sound knowledge of the energy and nutritional values of different foods [3–5]. In short, it is a potentially harmful misconception to assume that intense preoccupation with nutrition equates to a high degree of nutrition knowledge [4].
Numerous studies have investigated the level of nutrition knowledge in a range of groups, including medical and nursing staff, individuals from different age groups, from different sociodemographic backgrounds, and individuals with different comorbidities [6–11]. Despite the heavy emphasis of and preoccupation with weight, body shape, food and eating in individuals with EDs, only a few studies have examined their actual level of nutrition knowledge. The Beumont et al. study is believed to be the first to quantify nutrition knowledge in AN patients, and it found that patients had significantly greater knowledge than controls but a similar level of knowledge to psychiatrists and psychiatry trainees [12]. In the present literature search we found only two other studies, Laessle et al. [13] and SH Merriman [unpublished data, 2007]. Laessle et al. found that individuals with anorexia and BN had significantly greater knowledge in only some aspects of nutrition when compared to control participants [13], while Merriman found that individuals with AN had similar levels of nutrition knowledge to controls.
Nutrition knowledge is a predictor for eating behaviour [14], and a significant correlation between nutrition knowledge and eating behaviour in 7–8th grade Caucasian students was observed in the Pirouznia study in the USA [9]. Acculturation is associated with diet composition [15] and may presumably influence an individual's food choices through their nutrition knowledge. Pirouznia also found an association between ethnicity and nutrition knowledge in 6–8th graders, in that those who identified as Caucasian had significantly higher knowledge levels than their non-Caucasian counterparts [9]. Ethnicity, however, is a poor proxy for culture and no previous studies have examined the association between culture and nutrition knowledge. Cross-cultural issues are pertinent because EDs, which were once believed to be Western culture-bound syndromes, have been presenting from diverse ethnic and cultural groups in recent decades [16].
The current dearth of empirical literature on the nutrition knowledge of individuals with an ED provides poor evidence-based information for guiding interventions. In practice, nonetheless, multiple assumptions are made, and these permeate treatment recommendations. In AN, although it is not recommended that dietary counselling be the sole form of treatment [17], weight and nutritional restoration are significant components of AN management and the incorporation of nutritional advice is recommended [4,18,19]. Nutrition counselling is also recommended as part of the management of BN [4,19]. There is presently a lack of information regarding the impact of cross-cultural factors, despite information elsewhere supporting the influence of culture on dietary intake [15], eating habits and nutrition knowledge [9]. The aim of the present pilot study was to assess the level of nutrition knowledge of young women with and without EDs in a Western and non-Western country with reference to cultural orientation. We hypothesized that individuals with EDs would have greater knowledge than those without EDs and that acculturation to Western culture would be associated with greater nutrition knowledge.
Methods
Participants
The present data form a subset from a larger suite of cross-cultural studies into EDs [15,20,21]. Singapore was chosen as the non-Western country for study because there is presently relatively little research on EDs in Asia and very little conducted in Singapore. Participants were women aged 14–38 years who were either undergoing treatment for an ED (n = 55) as classified by the DSM-IV criteria [1] (AN, BN and EDNOS) or healthy controls who had never been diagnosed with an ED (n = 99). The final study sample consisted of ED North European Australians (n = 35), control North European Australians (n = 32), ED East Asian Australians (n = 2), control East Asian Australians (n = 22), control North European expatriates in Singapore (n = 12), ED Singaporean Chinese (n = 18) and control Singaporean Chinese (n = 33). Participants were of self-identified North European or East Asian backgrounds and those recruited in Australia were either born in Australia or migrated to Australia by the age of 12 years. The East Asian group in Australia included participants who identified as being of Chinese, Vietnamese or Korean descent.
ED participants were recruited from four teaching hospitals in Sydney and two teaching hospitals in Singapore. Control participants were recruited from a variety of sites: Australians through the University of Sydney campus, Singaporean Chinese from the nursing staff of one of the teaching hospitals in Singapore, and North European expatriates from staff and students of an international school in Singapore. Exclusion criteria included non-fluency in spoken or written English, pregnancy or lactation. The study was approved by the relevant ethics committees in both countries and written informed consent was obtained from all participants. Where participants were considered minors, consent was obtained from their parents.
Measures
Participants completed the following questionnaires.
Demographics questionnaire:
This questionnaire recorded ethnicity, level of education and parental occupation.
Vancouver Index of Acculturation
The Vancouver Index of Acculturation (VIA) has two scales: the Mainstream or Western scale, which measures orientation to Australian/Western culture, and the Heritage or Traditional scale, which measures orientation to traditional culture [22]. Both scales have strong internal consistency and concurrent validity [22]. The VIA was modified for language appropriate to Australia and Singapore following consultation with the Index's author [Ryder A: personal communication]. Participants were instructed to answer the VIA's items on cultural minority with respect to their own cultural background, and participants of North European background interpreted these items with respect to cultural minority groups in general.
Nutritional Knowledge Questionnaire
The Nutritional Knowledge Questionnaire consists of 20 multiple-choice questions, each with five options, and yields a score of 0–20, with a higher score indicating a higher level of nutrition knowledge [23,24]. The Questionnaire assesses knowledge over a range of nutrition topics, including energy content and requirement, dietary fibre, public health nutrition, nutrient sources, the effects of food processing and the metabolic role of nutrients, and was developed by an Australian dietitian to assess the need for dietetic counselling across a variety of patients [23]. Participants are instructed to endorse the correct or most correct statement and some example questions are as follows: (i) all red meats are rich in calcium; (ii) calcium is used in the synthesis of haemoglobin; (iii) iron requirements are reduced in pregnancy; (iv) seafoods contain more iodine than meat and poultry; and (v) all seafoods are rich in fat. The Questionnaire was administered to 2175 subjects (mean age = 27.0 years, SD = 13.8) and showed good internal consistency (Cronbach α = 0.80, p < 0.001) [24]. For participants residing in Singapore, ‘Australia’ was changed to ‘Singapore’ in the Questionnaire [24]. It was decided to use this tool because we knew of no other Australian questionnaire for assessing nutrition knowledge at the time of data collection. Also, the questions were sufficiently generic to apply in a Singaporean context, because none of the statements were of nutritional issues unique to Australia. One of the authors, who is a dietitian of Asian ethnicity, reviewed the questions to ensure that they were still current.
Height and weight were measured in duplicate using the International Society for the Advancements of Kinanthropometry technique [25], with the participant lightly clad: stretched height was recorded using a graph wall chart and headboard to the nearest millimetre and weight using digital scales (Tanita 1618; Tanita, Tokyo, Japan) to the nearest 200 g. When duplicates were >2% apart, a third measurement was taken. Median heights and weights were used to calculate body mass indices (BMI = kg m−2).
Socioeconomic status (SES) was determined using a social prestige scale [26] for paternal occupation, in which a lower score indicates higher SES. If the participant's father was not residing with the participant, maternal occupation was used. Because many of the participants were still in formal education and thus were not financially independent, education level was taken into account to provide a more complete picture of social status.
Statistical analyses
Age, BMI and SES were initially compared across the cultural and diagnostic groups on one-way analysis of variance with post-hoc Scheffé tests. VIA scores were compared using repeated-measures ANOVA followed by pair-wise comparisons with Bonferroni adjustments for multiple comparisons. Multiple linear regression of Nutritional Knowledge Scores was carried out against clinical (ED/control) status, VIA subscale scores, age, cultural group, education level and SES with backwards elimination, using SPSS version 15 (SPSS Inc, Chicago, IL, USA). Interactions between cultural group and clinical status, clinical status and VIA Australian/Western scores, and clinical status and VIA Traditional scores were tested. Age was retained throughout for face validity.
Results
Participant characteristics
Table 1 shows the mean age, BMI, VIA scores, SES, education level and Nutritional Knowledge Scores for the participants. Of the participants with EDs, 71% were diagnosed with AN, 24% with BN and 5% with EDNOS. It was decided to retain the ED East Asian Australian group despite there being only two participants due to the way the data were coded for the analyses by multiple linear regression; the participants were categorized as having an ED (n = 55) and being East Asian Australian (n = 24).
Participant characteristics
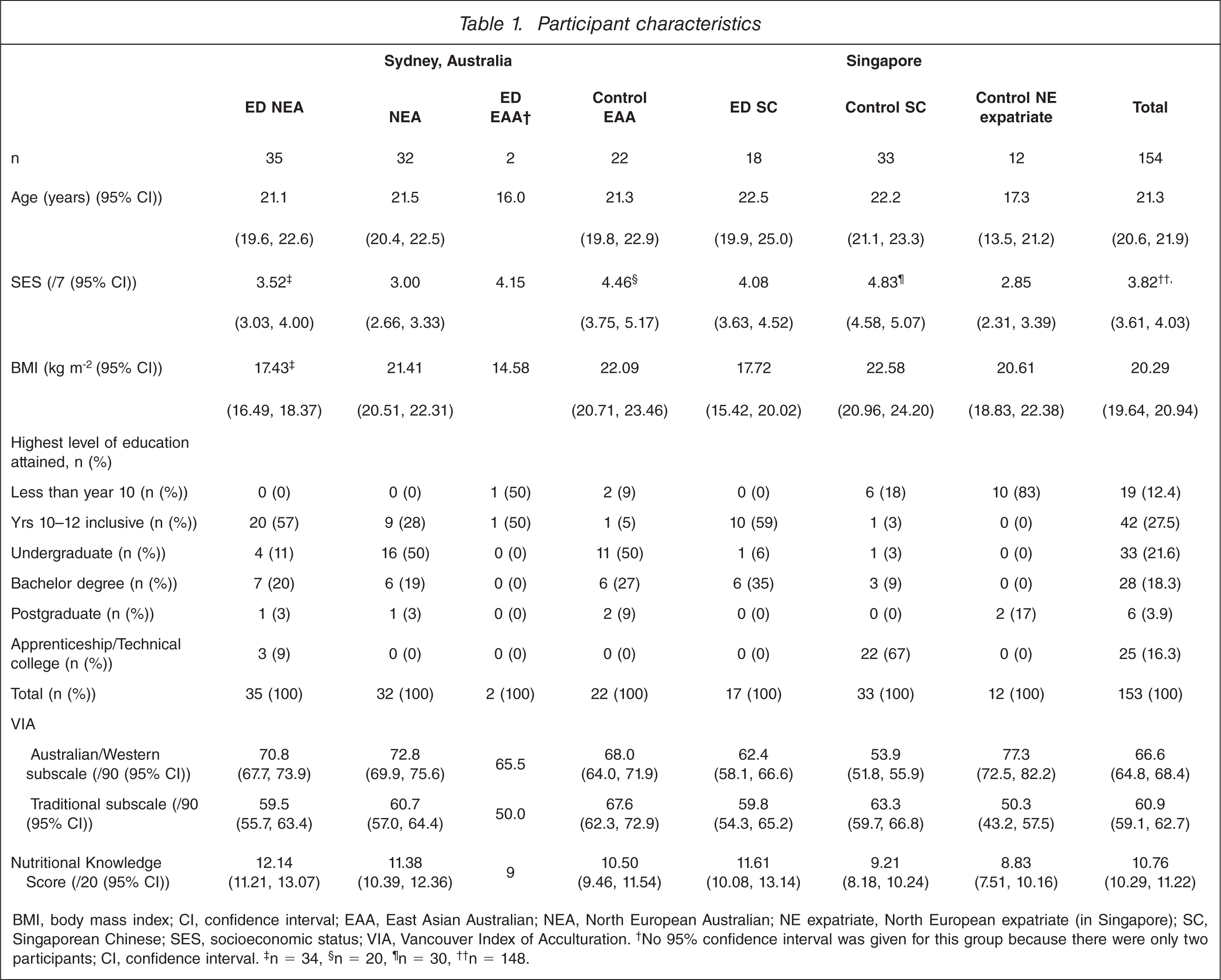
BMI, body mass index; CI, confidence interval; EAA, East Asian Australian NEA, North European Australian; NE expatriate, North European expatriate (in Singapore); SC, Singaporean Chinese; SES socioeconomic status; VIA, Vancouver Index of Acculturation. †No 95% confidence interval was given for this group because there were only two participants; CI, confidence interval. ‡n = 34, §n = 20, ¶n = 30, ††n = 148.
There were significant differences across the groups for age (F6,147 = 3.27, p = 0.005), SES (F6,141 = 10.62, p < 0.001) and BMI (F6,146 = 10.35, p < 0.001). There was also a significant difference between VIA Australian/Western scores and Traditional scores (F1,147 = 28.10, p < 0.001) and significant differences across the cultural and diagnostic groups (F6,147 = 5.51. p < 0.001). The interaction between cultural and diagnostic group and the difference between Australian and Traditional scores was significant (F6,147 = 16.80, p < 0.001). Detailed analyses for age, BMI, SES and VIA scores have been described previously [21]. Education level was not compared across groups due to the large number of cells with few responses.
Nutritional Knowledge Questionnaire score
Table 2 shows the final multiple linear regression model for Nutritional Knowledge Questionnaire scores. None of the interactions was significant. ED status (t147 = 2.33, p = 0.02) and greater acculturation to Western culture (t147 = 2.02, p = 0.045) were associated with higher nutrition knowledge. Cultural group was significant (F3,147 = 2.84, p = 0.04), in that expatriates had significantly lower nutrition knowledge than North European Australians (t147 = −2.75, p = 0.007) and marginally lower knowledge than East Asian Australians (t147 = −1.87, p = 0.06). Age, SES (t133 = −0.26, p = 0.8), VIA Traditional scores (t140 = −0.61, p = 0.5) and education level (F5,141 = 1.67, p = 0.2) were not significant.
Multiple linear regression model for Nutritional Knowledge Questionnaire scores
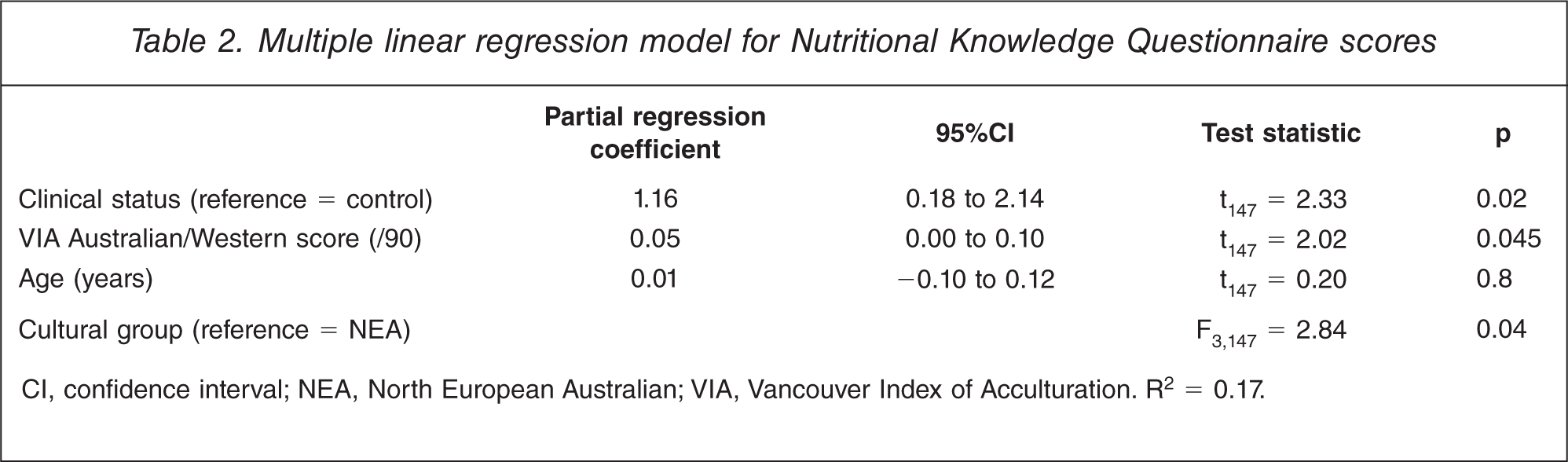
CI, confidence interval; NEA, North European Australian; VIA, Vancouver Index of Acculturation. R2 = 0.17.
Women with and without EDs showed similar themes in the areas in which they had greater nutrition knowledge and the areas in which they lacked knowledge. Knowledge of medical nutrition and food processing and technology was poor. For example, only 4% of those with EDs (n = 2) and 5% of controls (n = 7) correctly endorsed the statement ‘Human milk contains more vitamin C than cow's milk’, this question having the lowest frequency of correct responses. ‘Polyun-saturated margarines are always spreadable immediately after removal from the refrigerator’ was correctly endorsed by 20% of women with EDs (n = 11) and 22% of controls (n = 22); ‘Textured vegetable proteins are being developed as meat substitutes but they contain less fat than meat’ by 18% of those with EDs (n = 10) and 24% of controls (n = 24). Statements on dietary fibre and calcium content were correctly endorsed the most frequently by both groups, for example: ‘Whole milk, skim milk, yoghurt and cheese are all rich sources of calcium’ (n = 54, 98% ED; n = 85, 86% controls); ‘Wholemeal bread contains more fibre and vitamin B than white bread (n = 51, 93% ED; n = 91, 92% controls); and ‘A wholegrain or fortified cereal with milk forms a good basis for an adult's breakfast (n = 49, 89% ED; n = 82, 83% controls).
There was a large difference (29%) in the proportion of women with EDs who correctly identified ‘The purpose of most reducing diets is to provide nutritious meals and reduce the kilojoule intake below the kilojoule output in order to achieve a weight loss of from 500 g to 1 kg weekly’ (n = 39, 71%) compared to controls (n = 42, 42%). The statement ‘Kilojoules are provided by protein, fat and carbohydrates in our diet’ was correctly identified by 89% of those with EDs (n = 49) compared to 69% of controls (n = 68), a difference of 20%.
Discussion
Although women with EDs had statistically significantly greater nutrition knowledge than their control counterparts after adjusting for age, cultural group and acculturation level, the magnitude of the difference was small, at an average of 1 point. In comparison, the Beumont et al. earlier study using the same questionnaire observed that women with AN scored a mean of 14.1, significantly higher than controls at 12.5 [12]. It is questionable whether the difference between women with and without EDs in the current study would be of practical or psychological importance in a clinical setting, and it suggests that saturation coverage of nutritional issues in the media may have diminished any previous difference between those with and without EDs. This is especially so because neither SES nor education level were significant predictors of nutrition knowledge. Those without EDs may have caught up with knowledge. Alternatively, the presumed superior knowledge of those with EDs may simply be a myth and/or confused with nutritional preoccupation.
A more recent study was comparable to the present study, finding no difference between the level of nutrition knowledge in young women with subclinical levels of disordered eating and that of controls [27]. Even earlier studies on nutrition knowledge in women with AN noted that not all had good knowledge and that the knowledge was skewed towards certain topics [5,13, Merriman SH: unpublished data, 2007]. The present study observed a lack of knowledge in food technology, food processing and medical nutrition issues in both women with EDs and controls. A much greater proportion of those with EDs, however, correctly identified statements in regard to weight control and energy sources compared to those without EDs, which is in agreement with the results of previous studies. Laessle et al. found that patients with AN or BN had greater knowledge on macronutrients, fibre and energy compared to young healthy adults, but the levels of knowledge regarding vitamins and minerals were similar [13]; this was echoed by Beumont et al. who found that AN patients’ knowledge of energy content, fibre and dieting were good but that knowledge of public health was low [12]. Merriman found that although patients with AN had similar overall nutrition knowledge scores to controls (insurance company employees), the patients had greater knowledge of carbohydrates and fibre but lower levels of knowledge regarding protein and fat. In Merriman's study, 42% of participants with AN had lower scores on protein compared to controls’ mean scores and 58% scored lower on fibre. Thus, nutritional knowledge in individuals with EDs is selective, and in some areas of nutrition the level of knowledge can be poor and should be targeted in nutrition counselling.
The significant association between acculturation to Western culture and nutrition knowledge concurs with our hypotheses and indicated a potential difference of up to 4 units out of a score of 20, which is somewhat more substantial. The analyses of VIA scores showed differences in the levels of acculturation by cultural group and clinical status, but even after controlling for acculturation and age, a significant difference was observed between expatriate women and their Australian counterparts. It is not clear what this finding indicates, but one possible reason may be the lesser accessibility or availability of nutrition information in Singapore compared to Australia, although lay sources of nutrition knowledge such as those from popular magazines have been described as dubious because they often report extreme or incorrect nutrition information [4,28]. A sample bias could also explain this: namely, the control Singaporean Chinese were nursing staff and thus were likely to have greater access to nutrition information due to their employment compared to other women in the Singaporean community. Although the study sample appears to have been unevenly distributed with regards to education level, which may reduce the applicability of these data, education was not a significant predictor of nutrition knowledge, nor was it a confounder of the remaining variables. It is also possible that the non-significance of SES and education in the present study is due to our modest sample size, because other surveys using much larger study samples (n = 1040) [11] found higher SES to be significantly associated with greater nutrition knowledge.
The small sample size of the present study precluded analysis by ED subtype, where there may be differences in nutrition knowledge [27]. Although the present sample size of ED participants was comparable to those of previous studies [13, Merriman SH: unpublished data, 2007], a larger sample may be more informative, and would also allow for analysis by subtype. Limitations aside, strengths of the present study are the narrow definition of ethnicity and maintenance of a separation between Australian and Singaporean participants and the use of a quantitative measure of cultural affiliation. This is in contrast to studies in which ethnic groups are pooled and where ethnicity is used as an index for cultural affiliations [9]. Culture is a complex construct [16], and using a bi-dimensional measure allows an individual's level of affiliation to both Western and traditional cultures to be taken into account. To our knowledge this is also the first cross-cultural, cross-national study into the nutrition knowledge of women with EDs, contrasting with previous studies such as that of Breen and Espelage in the USA [27] and Merriman in the UK, which did not discuss the potential impact of culture.
Also of interest for future research is further investigation into the nutrition knowledge of health professionals, given concerns that health professionals’ nutrition knowledge levels may not be sufficient [29,30], particularly in those who work in the ED field [3]. The present literature search found numerous published studies into the nutrition knowledge of health professionals over the last three decades: in medical doctors, medical students, nurses and allied health professionals, and in various countries. It is inappropriate, however, to compare studies that have used different questionnaires. The Beumont et al. study, which used the same Nutritional Knowledge Questionnaire, found no difference between the nutrition knowledge of women with AN when compared to psychiatrists and psychiatric trainees, who scored a mean of 14.3 [12]. In another study, also using the same questionnaire, medical professionals scored on average 13.8, nurse trainees 11.0 and dietitians 18.6 [24]. It is essential that health professionals who treat individuals with EDs have adequate nutritional knowledge so that they can confidently respond when patients report nutrition misinformation and can identify that a seemingly well-informed and nutritionally preoccupied patient may not in fact have a good level of nutrition knowledge. Also, by identifying patients’ skewed or distorted views of nutrition, more appropriate targeted interventions can be delivered [3].
In conclusion, the present study has empirically identified a positive association between acculturation to Western culture and level of nutrition knowledge, but minimal differences in the level of knowledge between young women with and without EDs. There may be a difference in knowledge level, however, between women with EDs and the health professionals who treat them. Future studies into nutrition knowledge of individuals with EDs should involve a larger study sample, compare nutrition knowledge across ED subtypes and also include, in parallel, a sample of health professionals (psychiatrists, nurses, general practitioners, psychologists and dietitians) who are involved in their treatment.
Footnotes
Acknowledgements
We thank the hospital and school staff for their assistance in facilitating data collection and all of the participants. The late Pierre Beumont, Professor of Psychological Medicine, University of Sydney, was a significant contributor to the study prior to his death in 2003. This study was partly supported by the Edith Mary Rose Travelling Scholarship and the Faculty of Medicine Postgraduate Scholarship, University of Sydney. Part of this study was presented at the fifth annual conference of the Australian and New Zealand Academy for Eating Disorders, 2007.