
Abstract
Emotion toward anticipated and actual outcomes acts as a vital signal on emotional decision-making, and the Iowa Gambling Task (IGT) can mimic this decision-making process. Pain can impair emotional decision-making behaviors because it captures attention and distracts from the task at hand. Alternatively, pain may facilitate emotional decision-making behaviors by prompting alertness and mobilizing cognitive resources to maximize rewards. The present study investigated the influence of ongoing pain on emotional decision-making behaviors using the IGT. Our study recruited two groups of participants and applied capsaicin (pain group) or control cream (control group) to their forearms. We then compared performances and selections between the pain and control groups. The results revealed that participants successfully learned the required adaptive selection strategy as the task progressed. The study observed a tendency toward optimal choices for both groups under the condition of frequent–small losses. However, we observed a disadvantageous preference for the control group, but not the pain group, when faced with choices with infrequent but large losses. The study implies that a distressing pain experience motivates individuals to adjust goal-directed behaviors to maximize their rewards in a task. Thus, the finding suggests that ongoing pain facilitates emotional decision-making behaviors.
1 Introduction
Decision-making is a complex process that relies on both cognition and emotion. Cool decision-making denotes the use of decision processes associated with executive functions, cognitive abilities, and rationality, whereas hot decision-making indicates decision processes heavily dependent on affective states, emotional feedback, and visceral responses [1–4]. Professionals have considered emotion as a heuristic factor that significantly influences the process of making decisions implicitly and rapidly [5, 6]. Many believe that emotion toward anticipated and actual outcomes acts as a vital signal directing the making of certain decisions [7–10]. Emotional decision-making thus refers to those decision-making behaviors that rely primarily on emotional states or feedback, such as gambling tasks involving uncertainties, rewards, and risks [11, 12].
To explore the effects of emotion on decision-making, the Iowa Gambling Task (IGT) [13] was initially developed to mimic a real life decision-making scenario, including a series of deck selections with multiple trade-offs in an uncertain situation. Participants are required to select one card from four decks, where each card selection yields gains and occasional losses. They were instructed to gain as much as possible throughout the task. Among the four types of decks, two decks (disadvantageous decks) yield high immediate gains but net losses in the long run, whereas another two decks (advantageous decks) lead to small immediate gains but net gains in the long run. Although it can be difficult to articulate which decks are truly advantageous, healthy participants will progressively learn which ones lead to net gain or loss through the feedbacks, and eventually shift to advantageous decks. It is believed that apart from explicit knowledge, the IGT involves the generation of autonomic responses that signal emotional identification with choices already made and with the rewards and penalties received based on those choices [9, 14]. Thus, the IGT is frequently utilized to assess emotional decision-making ability (e.g., see Refs. [15–18]). Many IGT studies have revealed the disassociation between emotional decision-making and cognitive decision-making, with the latter requiring cognitive or executive resources [3, 4]. Therefore, the IGT has been considered a reliable paradigm for assessing emotional decision-making.
Previous studies have demonstrated that pain can influence the ability to make adaptive decisions due to its effects on multiple cognitive functions (for a review, see Refs. [19, 20]). For instance, patients with chronic pain generally exhibited poorer performance in the IGT as compared with healthy individuals [15, 21], as reflected by the increased selection of disadvantageous decks than advantageous ones. The results suggested that chronic pain impairs emotional decision-making, possibly due to failure in the processing of emotional feedback. Beyond experimental paradigms, patients with chronic pain tend to make poor decisions in real life environments as well [22]. It is likely that pain captures the sufferer’s attention and depletes limited cognitive resources, leading to insufficient cognitive resources for making adaptive decisions [23–25]. This evidence predicts that ongoing pain will impair decision-making in the IGT.
Nevertheless, pain may not always interfere with cognitive tasks. For instance, cold pain can help individuals to endure uncertainty and enhance reward-based learning and can facilitate the achievement of long-term rewards over instant benefits [26, 27]. Moreover, pain can serve as an alert by prompting defensive and adaptive behaviors [28, 29], thereby improving cognitive performances. For example, interpersonal neural activities successively increased in a dyad performing a cooperation task with ongoing pain [30]. This result suggests that pain-induced cooperation demands a cognitive control of the coordinating behavior and inference of each other’s cognition. Additionally, pain can increase neural responses in the medial prefrontal cortex to monetary incentives [31], which leads to alterations of the emotional responses to and the cognitive evaluation of reward. Indeed, the medial prefrontal cortex is responsible for integrating emotional signals that lead to an optimal decision [9, 13, 32]. Pain likely promotes adaptive behaviors by prompting alertness, mobilizing cognitive resources, and seeking collaboration to maximize rewards, in order to gain survival evolutionarily. This evidence predicts that ongoing pain will promote decision-making in the IGT.
Although evidence from clinical pain patients suggested detrimental effects of pain on emotional decision-making, comorbidities with clinical pain, such as depression, anxiety, and other emotional distress, may confound the modulatory effects of pain on decision-making [33–35]. Comparatively, experimental pain models deliver well-controlled noxious stimuli and can avoid many confounds presented in clinical data. Indeed, some studies revealed that experimental pain resulted in poor decision-making by adopting cold-stressor task intended to induce a relatively short period of cold pain [36, 37]. These studies, in fact, assessed the priming effects of acute pain on decision-making, with pain being induced before the decision-making task. Nevertheless, the modulatory effects on emotional decision-making induced by tonic pain that lasts a relatively longer time and mimics clinical pain remain unclear.
The present study aims to characterize the impact of ongoing pain in the healthy participant on that individual’s emotional decision-making. We recruited healthy participants and randomly applied capsaicin cream to induce ongoing pain (pain group) or control cream (control group) over the left forearm. Moreover, we employed the IGT to simulate decision-making strategies by factoring in the uncertainty of promises and outcomes as well as rewards and punishments. Overall performances during the task, as well as deck-selection preferences, were compared between the pain and control groups. Considering the impaired decision-making in clinical pain patients, it is likely that healthy participants with ongoing pain will make poorer decisions in the IGT than those in the control group, e.g., they exhibit greater preference toward disadvantageous decks. Alternatively, considering the faciliatory role of pain in reward-based learning and tolerance toward uncertainty in the decision-making process, it is likely that healthy participants with ongoing pain would make better decisions in the IGT than those in the control group, e.g., they exhibit more preference toward advantageous decks.
2 Materials and methods
2.1 Participants
The study recruited a total of 60 participants (female: 30; age: 20.10 ± 0.26 years, mean ± standard error of the mean [SEM]). All participants were right-handed with normal or corrected-to-normal vision. No participants reported any medical conditions associated with acute or chronic pain, cardiovascular or neurological diseases, psychiatric disorders, or current use of any medication. These participants were randomly allocated to either the pain group (n = 30; female: 15; age: 19.97 ± 0.38 years) or the control group (n = 30; female: 15; age: 20.27 ± 0.35 years). The two groups were well matched in terms of age and gender (p > 0.05 for both comparisons; Table 1). All participants provided written informed consent prior to the experiments in accordance with the Declaration of Helsinki. The local research ethics committee approved all the experimental procedures.
Characteristics of the decks.
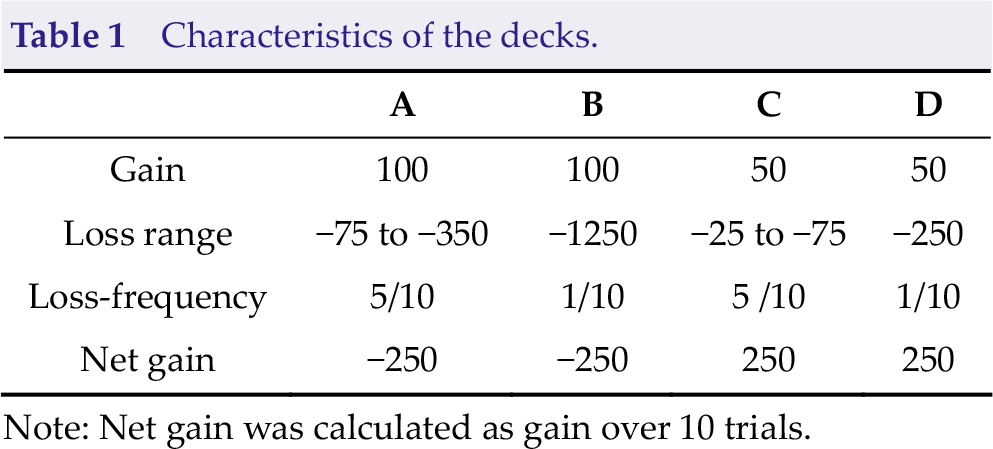
Note: Net gain was calculated as gain over 10 trials.
2.2 General experimental procedure
Upon arrival at the laboratory, the participants completed the positive and negative affect schedule (PANAS) [38] and state anxiety inventory (SAI) [39] to assess their mood and anxiety states, which have been demonstrated to influence performance in the IGT [40, 41]. A capsaicin or control cream was then applied to the left forearm of each participant. For the pain group, 0.3 mL of Capzacin-HP cream (0.1% capsaicin) was applied to a 2 cm × 2 cm area with a cotton swab on the volar side of the left forearm. Later, the area was covered with a plastic film to ensure skin contact, prevent evaporation, and accumulate body heat to produce thermal allodynia [31]. For the control group, the same amount of unscented hand cream was applied to the same 2 cm × 2 cm area.
The task was initiated 25 min after cream application, when the capsaicin cream had produced stable and moderate pain, as demonstrated by previous studies [31, 42]. Subsequently, the participants completed the IGT for assessing emotional decision-making behaviors. Those conducting the experiment used E-Prime 3.0 software (Psychology Software Tools, Inc., Pittsburgh, United States) to control the stimulus presentation in the task. To validate the success of pain manipulation, participants rated their perceived pain over the left forearm and their subjective feeling of unpleasantness immediately before and after the task. Ratings were made using an 11-point numerical rating scale ranging from 0 (no pain/unpleasantness) to 10 (unbearable pain/unpleasantness).
2.3 The Iowa Gambling Task
The task consisted of the presentation of four decks, namely, A, B, C, and D, on a computer screen. The participants were instructed to select one card from any of the four decks to gain as many points as possible, to be associated with their final revenue. The back of each deck looked the same, but the decks differed in composition. Each card in these decks could lead to a gain and occasional loss. Decks A and B could bring significant gains (i.e., 100 points) but expensive losses (i.e., −1250 points per 10 decks). Both decks are deemed disadvantageous, because they produce a net loss of 250 points for every 10 cards. Specifically, Deck A brings frequent but small losses, whereas Deck B leads to infrequent but larger losses. Decks C and D offer small gains (i.e., +50 points) but also smaller losses (i.e., −250 points per 10 decks). Both decks were deemed advantageous, because they produced a net gain of 250 points for every 10 cards. Specifically, Deck C leads to frequent but small losses, whereas Deck D denotes infrequent but significant losses. The task consisted of 5 blocks with 20 trials for each block, in accordance with a given pseudorandom sequence for arranging cards in each deck [13]. The task would shut off automatically after 100 selections, and each type of deck could only be selected a maximum of 40 times. The participants lack knowledge of the maximal number of choices as well as which decks were advantageous or disadvantageous [13]. Figure 1 depicts that the amount of money won or lost was presented on the screen. This amount was updated after each choice.
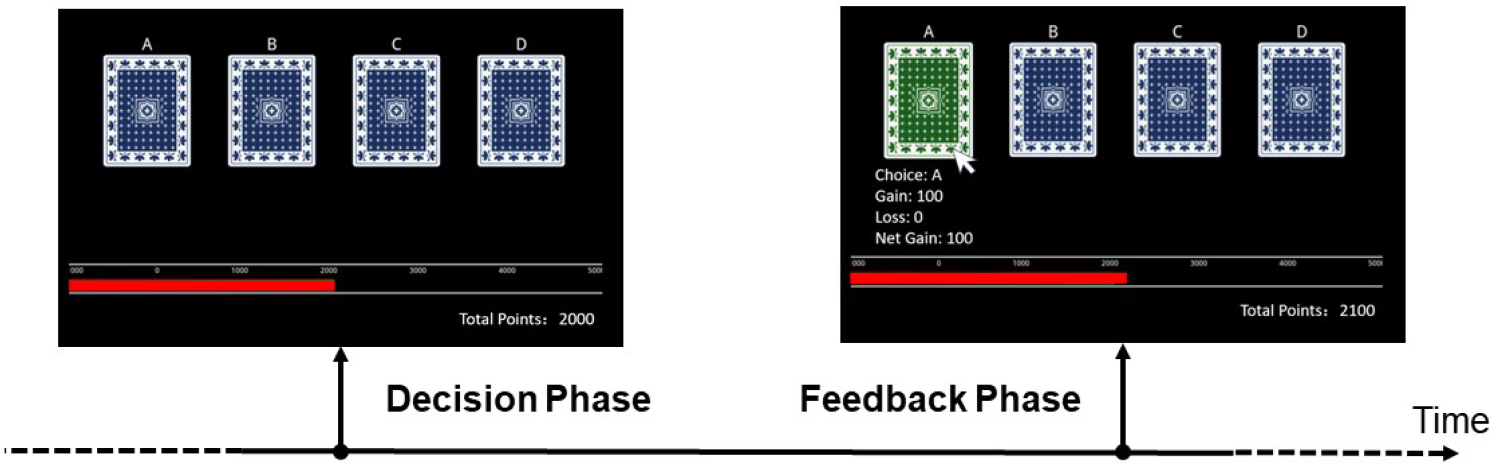
Schematics of the Iowa Gambling Task. At the beginning of each trial, all four decks are folded with an identical appearance. The participants select one card out of four decks (A, B, C, and D) in the decision phase without time restraint. The selected deck is highlighted in green, whereas the other cards are marked blue. The gain and loss of this deck, as well as the net gain, is presented at the bottom. The total points are presented using a progress bar.
2.4 Statistical analysis
We performed statistical analyses using IBM SPSS (version 22; IBM Corp., Armonk, New York, United States). Scores for state anxiety, as measured using the SAI, as well as positive and negative affections, as measured using the PANAS, were compared between the pain and control groups by independent-sample t-tests. To validate whether the capsaicin cream successfully evoked stable pain perception, we used two-way analysis of variance (ANOVA) to compare the subjective ratings of perceived pain and unpleasantness with a between-participant factor of Group (two levels: pain and control) and a within-participant factor of Time Point (two levels: before and after the task).
To quantify performances during the task, we calculated the IGT scores by subtracting the time points of selections of disadvantageous decks (A and B) from those of selecting advantageous decks (C and D). An independent-sample t-test was conducted to examine the differences in the overall IGT scores between pain and control groups. Considering the evidence showing gender differences in pain perception and anxiety with the topical capsaicin model [43], we explored whether pain-induced modulation on deck selection differed between females and males. Hence, we submitted the IGT scores to a two-way ANOVA with between-participant factors of Group (two levels: pain and control) and Gender (two levels: male and female). Then, to assess the dynamic performance along with the progress of the task, scores for the IGT were subjected to a two-way ANOVA with one between-participant factor of Group (two levels: pain and control) and one within-participant factor of Block (five levels: from Block 1 to Block 5). These analyses enabled us to determine the effects of ongoing pain on performance throughout the task.
As illustrated in Table 1, the four decks differed in terms of overall gain/loss and loss frequency: (1) Decks A and B were disadvantageous and could bring net loss, whereas Decks C and D were advantageous and could bring net gain; (2) Decks A and C could bring frequent but small losses, whereas Deck B and D could bring infrequent but large losses. Therefore, these four decks are characterized by two variables: Advantage and Loss-frequency. Arguably, simply treating deck as a four-level within-subject variable would overshadow the main and interacting effects of the containing attributes of decks. Therefore, to further elucidate the effects of ongoing pain on emotional decision-making considering the existent deck attributes, we applied a three-way ANOVA with a between-participant factor of Group (two levels: pain and control) and two within-participant factors of Advantage (two levels: advantageous and disadvantageous) and Loss-frequency (two levels: frequent–small and infrequent–large) to the deck selections. Post hoc comparison was performed only when the main effect or the interaction was significant.
3 Results
As revealed by the independent-sample t-tests, state anxiety (SAI) and the PANAS did not differ between the pain and control groups. Two-way ANOVA revealed the significant main effect of Group on the ratings for pain intensity (F
1,58 = 102.00, p < 0.001,
Demographic and psychometric measures for the pain and control groups.
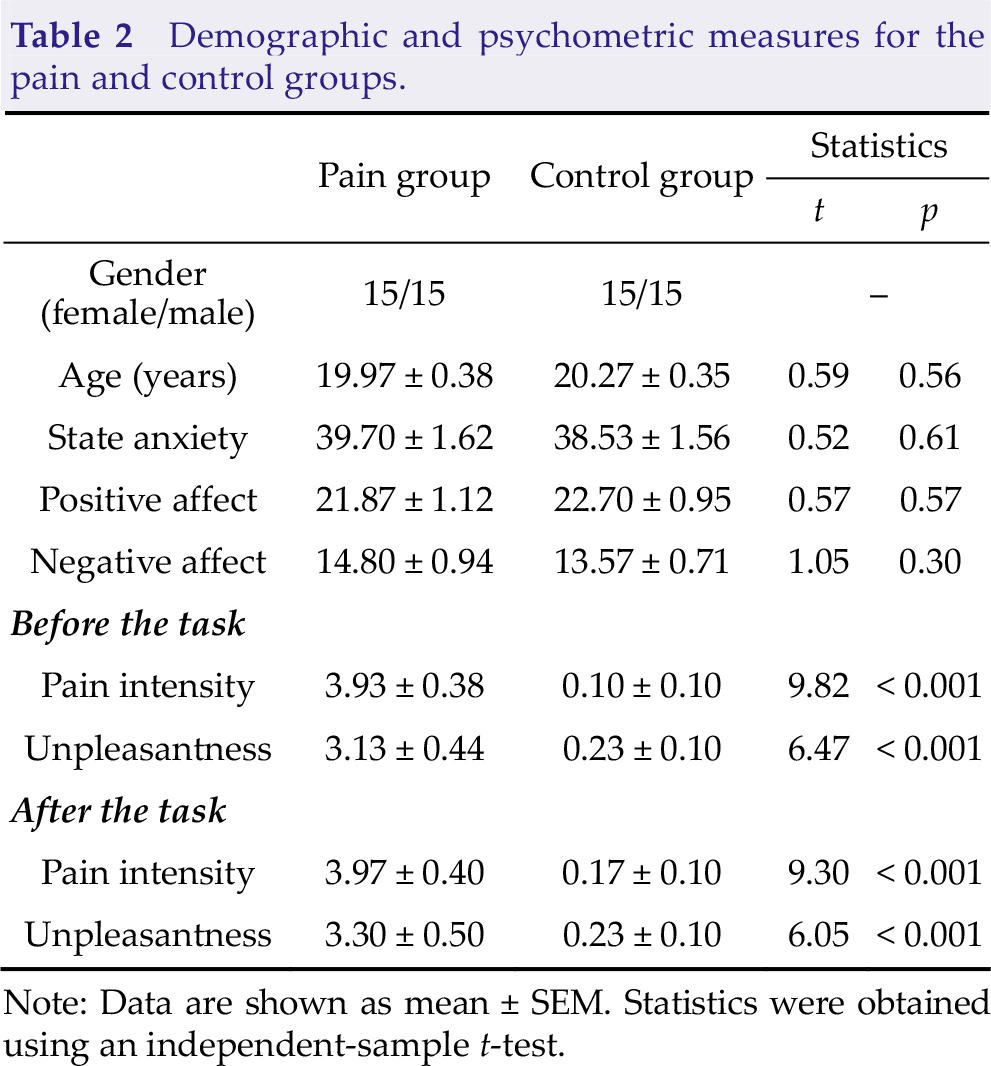
Note: Data are shown as mean ± SEM. Statistics were obtained using an independent-sample t-test.
As revealed by the independent-sample t-test, the overall IGT scores did not differ between pain and control groups (t 58 = 1.16, p = 0.25, Cohen’s d = 0.30). As revealed by the two-way ANOVA with factors of Group and Gender, neither any main effect nor the interaction was significant (p > 0.05). Analysis of the IGT scores considering blocks revealed the significant main effect of Block (F 4,232 = 21.96, p < 0.001, ηp 2 = 0.28), such that the scores for IGT were higher in the last block than in the first block (Block 5 > Block 1, t 232 = 7.72, p < 0.001, Fig. 2). These findings suggested that the participants progressively learned the risk of each type of deck throughout the task and were prone to select advantageous decks. However, either the comparison of two groups or the main effect of Group or interaction was non-significant, which suggested that experimental ongoing pain exerted no overwhelming effects on the IGT performance, acting similarly for females and males.
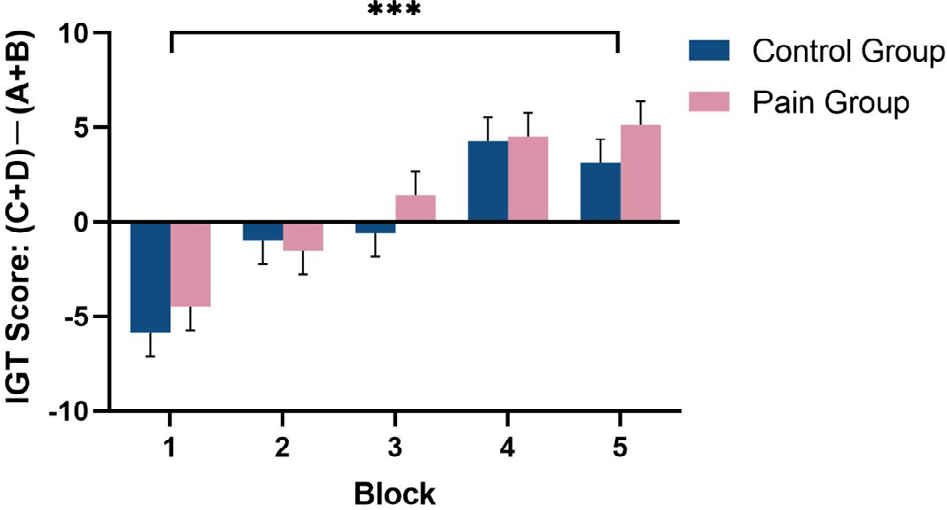
The IGT scores across the five blocks. The IGT scores were calculated as the difference in the times for selecting between advantageous (C and D) and disadvantageous (A and B) decks. Each block consists of 20 trials. The score in the last block was significantly higher than that in the first block for both groups, which suggests an overall advantageous decision-making. Data are shown as mean ± SEM. ***, p < 0.001.
Analysis of deck selection pointed to the significant main effect of Loss-frequency (F
1,58 = 40.86, p < 0.001,
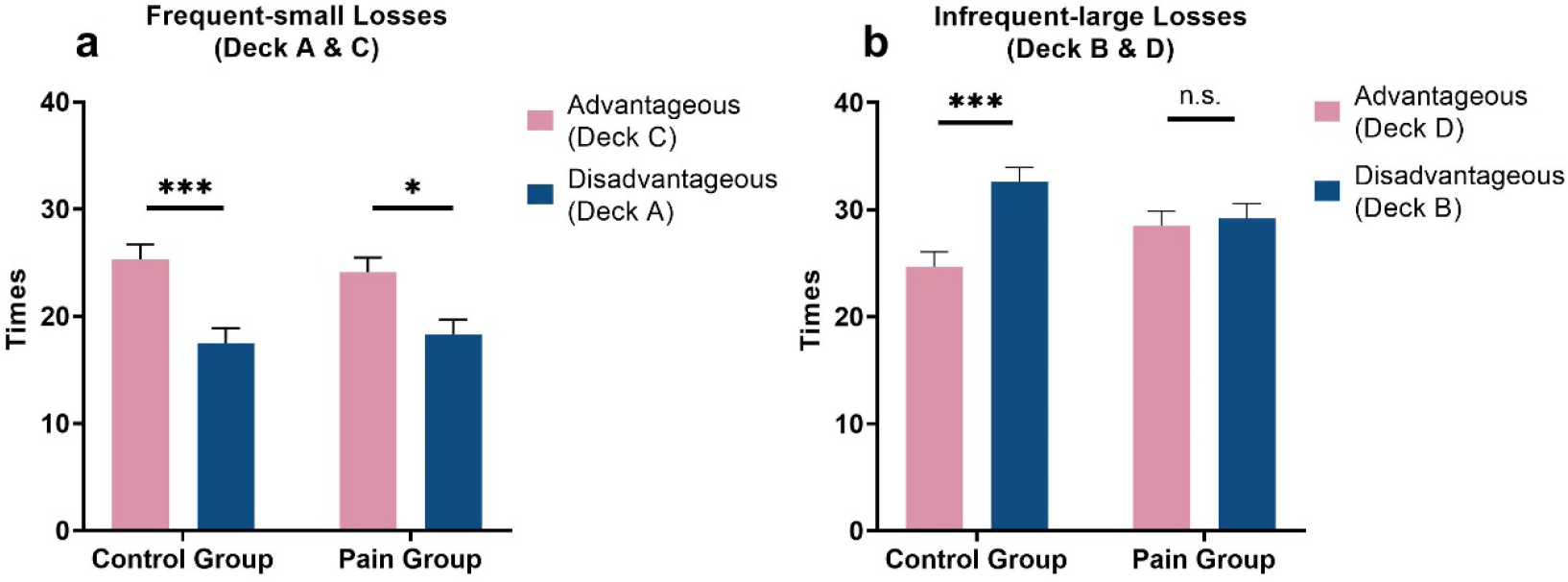
Times of selecting different types of decks. The total average number of times of selecting different types of decks (A, B, C, and D) of the participants in the control and pain groups. Decks A and B are disadvantageous decks that bring net loss, whereas Decks C and D are advantageous decks that bring net gain. Decks A and C bring frequent–small losses, whereas Decks B and D denote infrequent–large losses. (a) For decks with frequent–small losses, the advantageous deck was preferred over the disadvantageous deck in both groups. (b) For decks with infrequent–large losses, the control group, but not the pain group, preferred the disadvantageous deck. Data are expressed as mean ± SEM. ***, p < 0.001; *, p < 0.05; n.s., p > 0.05.
4 Discussion
The present study compared emotional decision-making behaviors between two groups of participants whose left forearms had been spread with capsaicin or control cream. The participants in both groups displayed higher scores in Block 5 than in Block 1 and exhibited a general preference toward advantageous decks. This result indicated the successful learning of the adaptive selection strategy along with the progress of the task. Although the overall scores for the IGT did not materially differ between the two groups, their preference for deck selection was different. For decks with frequent–small losses, the participants in both groups similarly preferred to select advantageous decks. However, for decks with infrequent–large losses, the control group preferred to select disadvantageous decks but not the pain group. These results suggested that ongoing pain promoted adaptive decision-making behaviors when confronted with choices with infrequent–large losses.
Pain is a distressing experience that exerts significant impact on cognition and behavior. Thus, this study adopted the IGT paradigm to assess the effects of ongoing pain on emotional decision-making. Participants in the two groups gradually exhibited preference for the advantageous decks. However, the overall IGT scores were comparable between the two groups. This finding is consistent with those of previous studies, which demonstrated that healthy participants eventually made more advantageous choices than disadvantageous ones although advantageous decks lead to small immediate gains [9, 13, 44]. The lack of difference between the pain and control groups is in contrast to evidence that illustrates impaired emotional decision-making in diagnosed patients with clinical pain [15, 21]. This discrepancy may be attributed to the difference in the nature of clinical and experimental pain. Specifically, clinical pain is more long-lasting and considerably more uncontrollable as compared with experimental pain that often brings a relatively short period of suffering with the assurance that the pain will vanish eventually. Moreover, pain comorbidities are frequently observed in the clinical pain patients, such as depression, anxiety, and other emotional distress [33, 34], which may confound pain modulatory effects on decision-making. Another possibility is the neural plasticity induced by clinical pain [45], particularly the alteration in the prefrontal cortex (involved in multiple cognitive processes), which leads to impairment in decision-making, while experimental pain is unable to cause such morphological alterations in the corticolimbic system. We further explored the differences between the IGT scores among females and males. Women rated the pain higher than men in response to pain induced by topical capsaicin application. Simultaneously, men exhibited more anxiety related to pain [43]. Nevertheless, our data revealed that gender has no moderating role in the effects of ongoing pain on emotional decision-making. The limited sample size (n = 15 per condition) may have led to this outcome. Future studies can further testify to gender differences, if any.
Although the participants generally distinguished the advantages and disadvantages of the four decks in the task well, the frequency of punishment modulated this preference. Frequent losses may facilitate discerning which decision is advantageous between the two decks in the long run. Ongoing pain experience did not influence this facilitative effect, which is consistent with evidence that pain experiences exerted no impairment on numerical ability [22], which may influence performance during the IGT. However, when faced with choices involving infrequent–large losses (Decks B and D), the participants in the control group made more disadvantageous choices that yielded higher immediate gains but a negative net gain in terms of long-term benefits. This result is consistent with that of the “Prominent Deck B” phenomenon observed in healthy participants [46], i.e., more selections made for Deck B (higher immediate gain but negative net gain) than for Deck D (lower immediate gain but positive net gain). Normal participants were often attracted by the immediate gains with high-frequency; however, they disregarded the unfavorable long-term effects, when confronted with a choice between frequent gains and infrequent–large losses. This tendency is known as decision myopia, where learning which deck is ultimately advantageous in such a situation is difficult for participants.
In contrast to the control group, this decision bias was not observed in the pain group, which made comparable selections of advantageous and disadvantageous decks when faced with infrequent–large losses (Decks B and D). Considering the long-term benefits, the pain group inhibited the default biased decision preference and applied a more adaptive decision-making strategy, suggesting the facilitatory effect of ongoing pain on decision-making. This finding was consistent with the evidence of the facilitatory effect of moderate acute stress induced by cold pain on long-term decision-making [26, 27]. This facilitatory impact may result from a stress-induced dopamine release, which may enhance reward salience and improve information updating on action–reward contingencies. It may also facilitate decision-making in terms of optimum benefits [47]. The current findings suggested that ongoing pain motivates individuals to adjust behaviors rapidly, which may result in accumulating resources instead of distracting individuals from a task and resulting in a cognitive decline. Moreover, the result is quite consistent with the evolutionary significance of pain, i.e., it serves as an aversive primary reinforcer that fundamentally facilitates learning processes [48, 49]. For instance, ongoing pain exerts a facilitatory effect on the activities of reward-related neural circuitry, wherein pain increases neural responses to monetary incentives. This notion indicates that pain boosts evaluation toward rewards and promotes the maximization of benefits for survival [31]. Additionally, pain can serve as a beneficial factor in promoting cognitive control and emotional regulation [29]. Many studies also demonstrate pain-related facilitatory effects on cognition, such as selective attention [50], concentration [51], and response inhibition [52]. These effects on cognitive processes may fundamentally underlie the facilitatory effects of pain on adaptive decision-making behaviors during the IGT.
Although we provided behavioral evidence for the effects of pain on emotional decision-making, the underlying neural mechanisms warrant future studies. Pain has long been considered a typical physiological stressor, which activates the hypothalamic–pituitary–adrenal axis, resulting in neurohormonal changes with notable impacts on brain activities. Indeed, Wang et al. illustrated a pain-induced modulation in response to rewards, which led to further alterations in emotional arousal and cognitive evaluation of rewards [31]. Scholars proposed that the prefrontal cortex plays a key role in decision-making under uncertain scenarios, particularly those that involve the processing of emotional signals and optimal decisions [9, 13, 53]. A plausible explanation is that pain promoted adaptive decision-making behaviors by increasing the activation of the prefrontal cortex during the IGT. Thus, we recommend that future studies test this hypothesis by adopting neuroimaging techniques.
5 Conclusion
In summary, this study demonstrated the facilitatory effect of ongoing pain on emotional decision-making behaviors, as reflected by the buffering effect of pain on “decision myopia” when confronted with infrequent–large losses. Specifically, when faced with decks with infrequent–large losses, the control group, but not the pain group, showed more preferences for the disadvantageous decks. A possible explanation is that ongoing pain facilitates the learning process, motivating individuals to adjust their behaviors to accumulate resources. This finding expands the current understanding of the impact of pain on goal-directed reward-seeking behaviors. However, future studies should investigate the neurophysiological mechanisms underlying this relationship.
Footnotes
Ethical approval
The local research ethics committee approved all the experimental procedures.
Consent
All participants provided written informed consent prior to the experiments in accordance with the Declaration of Helsinki.
Conflict of interests
All authors declare no conflict of interests.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 31871127), the Features Innovative Projects of Guangdong Province Ordinary University (Grant No. 2019KTSCX149), and the Shenzhen Basic Research Project (Grant No. 20200812113251002).
Authors’ contribution
Conception and design of the study: WP. Data acquisition: CL and SZ. Data analysis: CL, SZ and WP. Drafting the manuscript: CL and WP. Writing-reviewing and editing: CL, SZ and WP. All authors reviewed and approved the final draft of the manuscript.