
Abstract
People often experience two types of pain: social pain and physical pain. The former is related to psychological distance from other people or social groups, whereas the latter is associated with actual or potential tissue damage. Social pain caused by interpersonal interactions causes negative feelings in individuals and has negative consequences to the same degree as physical pain. Various studies have shown an interaction between social pain and physical pain, not only in behavioral performance but also in activities within shared neural regions. Accordingly, the present paper reviews: (1) the interaction between social pain and physical pain in individuals’ behavioral performances; and (2) the overlap in neural circuitry as regards the processing of social pain and physical pain. Understanding the relationship between social pain and physical pain might provide new insights into the nature of these two types of pain, and thus may further contribute to the treatment of illnesses associated with both types of painful experience.
1 Introduction
Pain is a negative experience involving sensory, emotional, cognitive, and social dimensions [1, 2]. In real life, people often experience many different kinds of pain, including experiences of physical and social pain that share underlying commonalities [3]. Social pain is defined as “the painful experience of actual or potential psychological distance from other people or social groups” [4], whereas physical pain is “an unpleasant feeling and emotional experience associated with actual or potential tissue damage” [1]. Generally, physical pain is most frequently elicited by direct damage, and social pain typically comes in the form of sights or sounds, often through stimuli with purely symbolic meanings (i.e., words, gestures, facial expressions, etc.) [2].
Physical pain is a multi-dimensional experience, including sensory-discriminative, affectivemotivational, and cognitive-evaluative components [5]. The emotional component is especially related to the unpleasant experience of physical injury [6]. Similarly, people always use the words “pain” and “heartbreak” to describe their feelings when they experience negative social interactions [7]. In fact, the social pain caused by interactions causes negative emotions in individuals, and has negative effects, to the same extent, as physical pain [6, 8]. It seems that physical pain elicited by a noxious stimulus is typically short-lived, yet social pain may last longer [9].
As we know, individuals with persistent pain are always vulnerable to negative psychological and social consequences [10]. Various studies have focused on the modulating factors of pain perception, yet not enough studies have paid attention to the interaction between social pain and physical pain. Some studies have shown that social pain and physical pain can affect each other in terms of perception, and share some common pain-related regions [11, 12]. Exploring the relationships between social pain and physical pain will help to understand the mechanism of pain perception and to improve targeted clinical treatments. This paper will review studies on the interaction between social pain and physical pain from behavioral and neural evidence that will provide important insights into the nature of pain.
2 Interaction between social pain and physical pain
Both pain overlap theory (which claims that social pain rode onto the existing pain circuitry developed to signal a bodily threat or harm [2, 4]) and social pain theory (which was based on the idea that the possibility of being separated from important social entities poses a critical challenge to our survival [2, 13]) underlie the links between social pain and physical pain [14]. The risk of damage to social relationships and physical damage were threats to human survival during evolution, during the time when it was very important to respond to these threats in a timely manner [15]. It is well-known that the pain system related to physical injury formed in the early stages of human evolution [16]. However, social life gradually became more and more important for people’s survival during the course of human civilization [13]. The detection of social threats, therefore, developed in relation to the same functional system [13]. People’s reactions to social and physical pain may overlap and interfere with each other [4, 13]. In fact, there is evidence to support these opinions.
2.1 Social pain affects the perception of physical pain
It has been found in many studies that social pain can affect the perception of physical pain. For instance, experiencing social exclusion can trigger physical pain [17]. Eisenberger’s study showed that the experience of social exclusion increases sensitivity to pain elicited by noxious stimuli [18]. Those people who felt more pain due to social exclusion also reported more painful responses to heat stimuli. Consequently, the reduction of the experience of social pain or loneliness can also reduce the experience of physical pain [19]. During surgery, for example, those who had more social support tended to experience less physical pain [20]. Interestingly, there is a study showing that female participants in long-term romantic relationships reported reduced perception of pain when they received heat stimuli amidst social support conditions [21]. Participants reported significantly lower pain ratings when they were holding their partner’s hand, or viewing a picture of their partner, compared to the control condition of holding a stranger’s hand. These findings show that social interactions may be capable of interfering with the experience of physical pain [11]. A recent study carried by Karayannis et al. tested this hypothesis using a cross-lagged longitudinal analysis of people with persistent pain. They found that social isolation affects pain interference and physical function over time, suggesting that therapeutic interventions, including strengthening social connections, might contribute to reducing the effect of physical pain [22].
2.2 Physical pain strengthens social pain
Generally, physical pain is associated with actual or potential tissue damage [1]. It is a basic symptom of many diseases [23], and was shown as being associated with insomnia, depression, and even suicide [24]. It has various negative effects on many aspects of people’s psychology, physiology, work, and life. As expected, there are commonalities between social pain and physical pain. Published studies reveal that individuals who are more sensitive to physical pain are more sensitive to social pain [25], and that increased physical pain can also increase social pain [11]. Eisenberger et al. found that participants who were exposed to endotoxins reported increased feelings of social disconnection when they were asked to report hourly on their feelings in the Cyberball social exclusion task after receiving endotoxins [12], implying that social pain and physical pain have a parallel effect on the social–physical pain overlap. Consistent with this evidence, variations in the pain-related receptor could predict dispositional sensitivity to social pain [26]. For instance, the mu-opioid receptors in neural regions involved in physical pain showed greater reactivity to social rejection [26].
2.3 Complicated relationships
Relationships between social pain and physical pain are more complicated. However, in contrast to studies showing that social pain can lead to increased sensitivity to physical pain, some studies have found that social pain may also have a numbing effect on physical pain [27, 28]. MacDonald and colleagues proposed that both physical pain and social pain can stimulate the body to enter a state similar to analgesia in order to help us to escape and avoid further injury when we face serious threats [13]. According to the pain overlap theory and the social pain theory, social pain could also trigger numbness in the body [13]. A series of studies conducted by DeWall and Baumeister showed that increased social pain reduced an individual’s perception of physical pain [29]. These seemingly contradictory results are quite possible. The body’s response to harmful stimuli is not simply linear, but varies depending on different factors, such as the severity of the injury, as well as the degree of tissue damage [30]. Generally, the perception of pain will increase as the severity of physical injury increases [28]. However, our body will enter a protective state and cannot feel pain when we survive amidst strong and continuous pain [31]. Similarly, our body may respond to very serious social harm by following the same pattern and will show different interference on the perception of pain [32].
A cautious attitude is indispensable to our interpretation, although many studies support the theories on overlap and the commonality between social and physical pain. Over the past 10 years, the overlap theory has faced significant challenges. Recent evidence has found that the gene of the pain-related receptor (e.g., the muopioid receptor) did not moderate social rejection sensitivity in three tasks designed to assess altruism, reciprocity, and trust in humans [33], indicating that past supportive evidence might not be very reliable. Moreover, growing neuroimaging findings have shown that the anatomical neural overlap is not specific to core pain processing brain regions [34]. Many new pieces of evidence prompt a more cautious interpretation of the apparent similarities between social and physical pain. However, exploring the interaction between these two experiences is important in order to understand the nature of pain. Still, more remarkable examples of functional crossover effects were empirically described. Chester et al. showed that social pain can mediate the effect of rejection by prompting greater motivation for social reconnection and would serve a similarly reparative function in relation to social injuries similar to physical pain [35]. Using the pupillometry to test whether being ostracized induces a conflict detection mechanism or social pain response, Sleegers et al. found that participants showed a diminished pupillary reaction to cues of exclusion, but not to cues of inclusion, consistent with the social–physical pain overlap theory [36]. The relationship between the two kinds of pain is too complicated to arrive at a consensus on the relationship between them. Given that neuroimaging studies have propelled overlap theory into the spotlight, we will introduce this next part in detail and provide some supporting evidence.
3 Shared neural circuit of physical pain and social pain
Evidence from behavioral responses supports the hypothesis that social pain and physical pain interfere with the perception of one when the other is present [32]. In fact, behavioral performance stems from the fact that social pain and physical pain rely on a shared neural circuitry [17].
3.1 Pain pathways and pain matrix
Nociceptors in the skin, muscle, and internal organs will generate pain signals after they receive physical, chemical, and inflammatory stimuli [37]. The signals are transmitted to the spinal dorsal root ganglia through the afferent nerve and will arrive at the dorsal horn of the spinal cord [38]. The integration of pain signals takes place initially in the spinal cord. Some signals are transmitted to the motor neurons in the ventral horn and prompt a defensive response through the motor nerves [39]. For example, such impulses would prompt muscle contractions in order to move the body out of the condition that is causing feelings of pain. The left signals continue up through the spinal thalamus bundle and the spinal brainstem bundle and finally arrives at the thalamus [40]. The preliminary integration of sensory information is performed in the thalamus and is then transmitted to the higher-level cortex in the pain matrix [41], such as the primary sensory cortex (S1), the dorsal anterior cingulate cortex (dACC), the dorsolateral prefrontal cortex (DLPFC), and the anterior and posterior insula and other painrelated brain regions, and then further continue to distinguish their components [42, 43]. The DLPFC is connected to the ACC, and they directly project to the periaqueductal gray (PAG), a core component of the descending pain modulatory system [43]. These descending pathways originate in the S1 and the hypothalamus, descending to the medulla and spinal cord [44], and inhibit ascending nerve signals [37]. The descending modulatory system can inhibit pain processing at the level of the spinal cord to induce pain relief [44] (Fig. 1). The pain-related ascending transmission and descending modulation pathways are affected by attention, emotion, and other cognitive factors [45], meaning that psychological factors can influence pain perception.
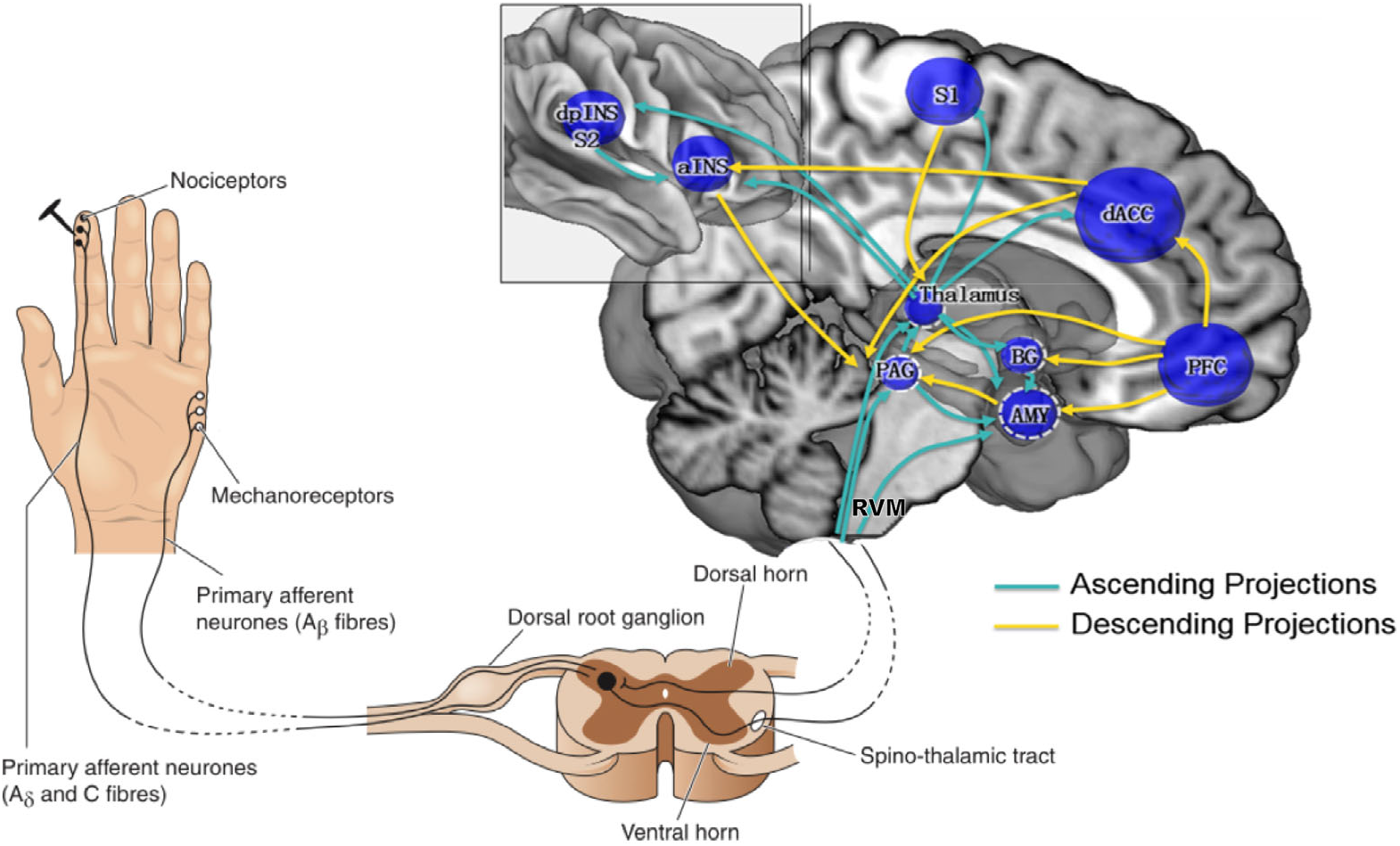
Pain pathways. (Modified from Ref. [43])
3.2 Overlap between physical pain and social pain
Some functional magnetic resonance imaging (fMRI) studies provide supporting evidence for the interaction between social pain and physical pain. It was found that physical pain and social pain rely on shared neural circuitry [6, 17] (Fig. 2), suggesting that the experience of physical pain and social pain may have the same neurological basis. Indeed, the neural activity in the “pain matrix” is functionally heterogeneous and part of it carries information related to both painfulness and intensity/salience [46, 47]. Negative experiences based on social pain can activate the brain areas related to the emotional components of physical pain [48]. The dACC, as an important area selective for pain using neurosynth [49], may be activated during individual experiences of social exclusion [50 –52]. The pregenual anterior cingulate cortex (pACC) is a key brain area involved in physical pain and social pain, which is responsible for processing unpleasant emotions caused by physical pain and negative emotions caused by social events [6]. Studies have shown that individuals taking acetaminophen (a common pain inhibitor) show reduced dACC activity during social rejection [29], implying a positive correlation between social pain and other activities in dACC.
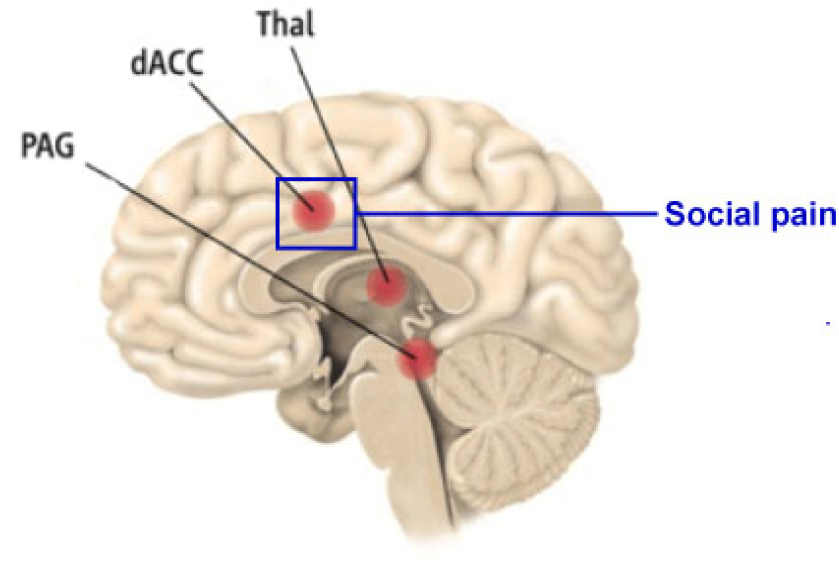
Pain network. (Modified from Ref. [49])
Some other functional brain regions are involved in the processing of physical pain and social pain. For example, the perception of physical pain is mainly coded by the insula, PAG, and the dorsal inner thalamus [53, 54]. It was shown that the right ventral prefrontal cortex (RVPFC) is related to coding the negative emotional experience accompanied by pain [55, 56]. In particular, the RVPFC is more capable of reappraising social pain compared with physical pain [57]. It seems that increased or decreased social pain could alter physical pain in a parallel manner, meaning that social pain might lead an individual to feel increased physical pain. These shared functional brain regions provide evidence for the interaction between social and physical pain.
Although overlap theory holds a mainstream position in the issues about the interaction between social pain and physical pain, a growing number of studies offer some challenges. Iannetti et al. detailed concerns with the fMRI-based overlap, suggesting that previous findings were not enough to distinguish pain from other stimuli due to activations in the pain matrix elicited by noxious stimulus involved in cognitive processes, including orienting attention and detecting of any salient events [34]. Salomons et al. even questioned whether there was a specific pain matrix. They compared the activities in the pain matrix in pain-free individuals and patients, and found no significant difference across the entire pain matrix or in key pain matrix regions [58]. Of course, some studies have successfully separated fMRI-pattern representations underlying physical and social pain at the gross anatomical level [59]. This innovative work reminds us to be more cautious in applying these theories to clinical treatments, and underlies the notion that more targeted research is needed in order to understand the interaction between these two types of pain.
4 Discussion
The interaction between social pain and physical pain reflects mutual perception not only in behavioral performance but also in shared common brain regions related to pain. Recent theoretical and methodological advances in social and cognitive neuroscience have improved the understanding of the interaction between social and physical pain. This understanding may provide new insights on the contributions to the treatment of mental illness issues that link both types of painful experiences. It could help to reduce individual experience of pain in two ways: by reducing physical pain with social support and by increasing feelings of social connections with reduced physical pain [3].
Two questions remain concerning the interaction between social pain and physical pain. First, a further understanding of the commonalities between social pain and physical pain is needed. According to previous findings, it seems that physical pain is a kind of psychological phenomenon modulated by attention and expectation, whereas social pain is a biological phenomenon related to survival in social life [3]. No doubt there is an inseparable relationship and commonality between the two types of pain which helps human beings to adapt to the environment. Are there internal connections between the two, or are they two different types of pain experience with common roles? Further studies of this issue are needed to help understand the nature of each kind of pain. Second, do these overlapping regions (e.g., dACC) play broader roles as a neural alarm response to negative experiences or threats, instead of uniquely responding to the saliences of social pain or physical pain? We still need to examine whether there are salient areas responding to social pain and physical pain, respectively. Future studies need to pay more attention to these fundamental issues in order to bring new insights to targeted treatment.
Footnotes
Conflict of interests
All contributing authors have no conflict of interests to declare.
Acknowledgements
This paper is jointly supported by the Scientific Foundation of Institute of Psychology, Chinese Academy of Sciences (No. Y9CX432005), and the National Natural Science Foundation of China (No. 81871436).