
Abstract
Empathy for pain is a hotspot in the field of empathy research because of its specific cognitive and neural mechanism. Currently, studies of empathy for pain can be classified into two categories based on the body regions receiving the painful stimulus, i.e., empathy for face pain and empathy for body pain, which conveys painful information based on individuals’ faces or body parts, respectively. Although the existing evidence revealed differences between these two kinds of pain empathy regarding the underlying cognitive and neural mechanisms, the current studies tend to confuse these findings. Therefore, we summarized the differences between empathy for face and body pain, mainly regarding the behavioral reactivity tendency, brain activations, and electrophysiological (EEG) signals. These differences probably stem from the fact that the human face contains more emotional information, while other body parts contain more perceptual information. Thus, future studies should identify the distinctions between empathy for face and body pain, to explore further how empathy for face pain is affected by the facial information of others and focus on empathy for face pain in individuals with psychopathological disorders. Furthermore, the specific reasons for these distinctions and their underlying neuromechanisms deserve to be further reviewed.
1 Empathy for pain
Empathy is considered to be the psychological process via which individuals perceive or imagine the emotional states and experience partially the feelings of other people [1]. Empathy for pain is a typical form of empathy, which is defined as the manner in which individuals perceive, estimate, and respond to the suffering of others [2]. Empathy for pain is commonly observed in daily life and has evolutionary meaning for individuals, as it promotes the building of prosocial behaviors and the development of interpersonal relationships.
Because of its specific cognitive and neural mechanism, researchers have paid significant attention to empathy for pain and rendered it a popular topic among the studies of empathy. According to a meta-analysis of functional magnetic resonance imaging (fMRI) studies, brain regions, including the anterior cingulate cortex (ACC), the anterior insula(AI), the amygdala, and several other areas are activated while people observe others in painful scenes [3]. These brain regions, which are considered as the pain matrix, i.e., a nervous system related to the processing of self-pain, are considered to include an emotional component and a sensory component. The emotional component of empathy for pain represents the unpleasant feelings caused by perceiving others’ pain, and the sensory component means the location and the intensity of the reaction to others’ pain [4]. Based on the findings of eventrelated potential (ERP) studies, there are two basic neural-processing stages of empathy for pain in the time domain. The first one is the earlier automatic processing stage (before 380 ms), which reflects the perception of others’ pain and the sharing of others’ feelings. The second one is the later cognitive evaluation stage (after 380 ms), which includes higher evaluations of others’ stations and action preparations [5].
However, the neural responses to pain empathy processing are affected by multiple factors, such as the experimental paradigms adopted [6] and attention constraints [7]. In addition, these studies are likely to neglect the discrepancies in neural activities caused by the body parts that receive the painful stimulus. In one of our recent studies, we used images showing faces receiving painful stimuli as experimental materials and found that different neural responses were elicited under different attention cues (the subjects’ attention was directed to the pain cues or non-pain cues) [8]; in contrast, there was no such discrepancy when images showing body parts (hands or feet) receiving painful stimuli were used as experimental materials [9]. This suggests that the empathy for pain in the faces or body parts of others may occur via distinct cognitive and neural mechanisms.
2 Empathy for face and body pain
Most previous studies explored the cognitive and neural mechanisms of empathy for pain in the visual modality by having the participants observe the suffering of others in laboratory experimental conditions. In summary, two main types of empathy for pain were detected, depending on the images that were used to show others’ pain in those previous experiments, as follows. (1) Empathy for face pain. The observers estimated pain information from others’ faces. As shown in Fig. 1, the images showing neutral faces receiving painful stimuli depicted faces being pricked by a needle, while the images showing neutral faces receiving non-painful stimuli depicted faces being touched by a cotton swab at the same location (e.g., Ref. [8]). (2) Empathy for body pain. The observers estimated pain information based on the injury of others’ body parts, e.g., accidental injuries to hands or feet in daily life [2]. As shown in Fig. 2, the images showing body parts receiving painful stimuli depicted hands or feet accidentally hurt by a knife or pricked by a needle, while the images showing body parts receiving non-painful stimuli depicted a similar scene without any information of pain.
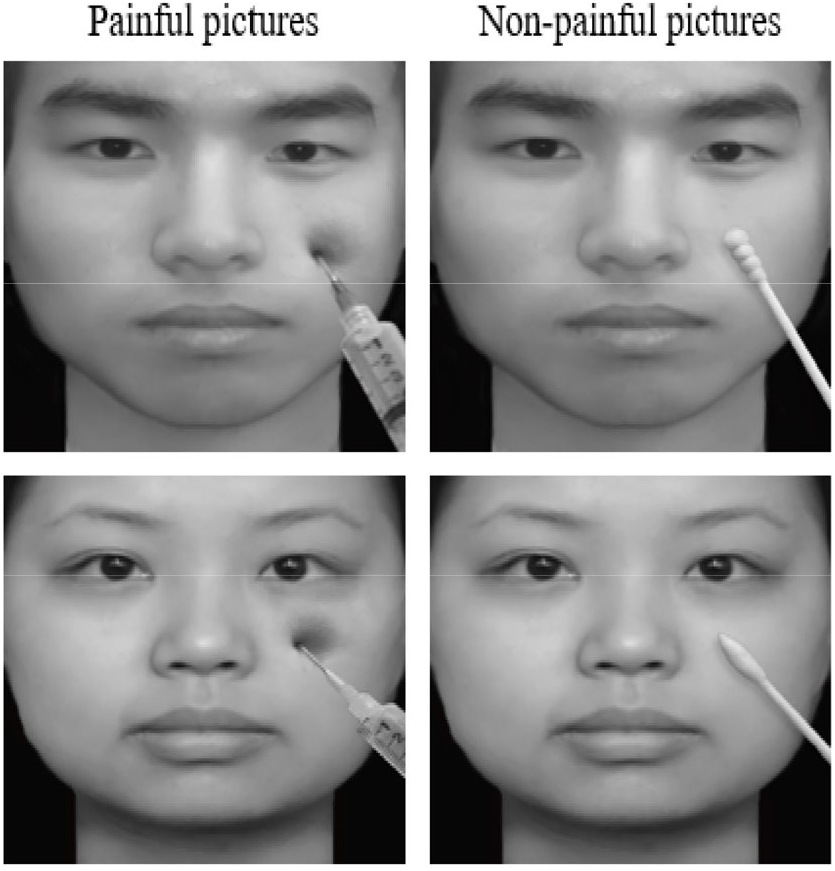
Images used to assess empathy for face pain. Left panel: images showing neutral faces receiving painful stimuli. Right panel: images showing neutral faces receiving non-painful stimuli. Reproduced from Ref. [8] with permission of the authors.
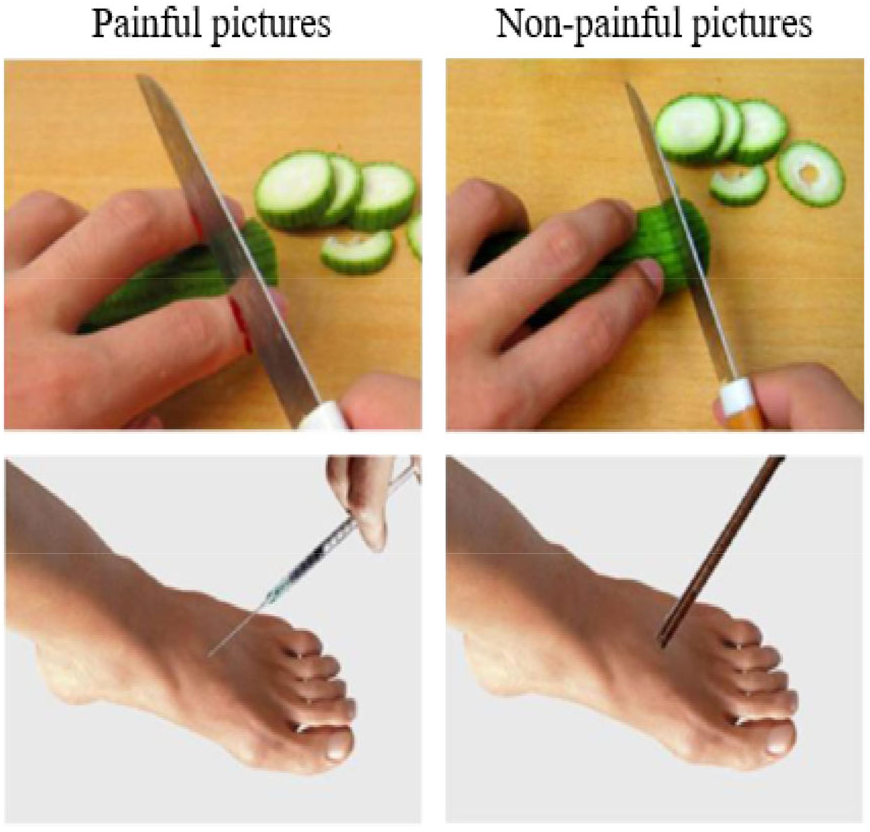
Images used to assess empathy for body pain. Left panel: images showing body parts receiving painful stimuli. Right panel: images showing body parts receiving non-painful stimuli. Reproduced from Ref. [2] with permission of Springer.
However, individuals may exhibit different empathic behavioral and neural responses to others’ faces and bodies. For instance, one study found a greater amount of activation over the right ventral premotor area while watching others’ facial movement compared with finger movement [10]. This result, to some extent, indicated that there may be discrepancies in the processing of others’ faces and body parts. There is also evidence indicating that, during the observation of images showing body parts or faces receiving painful stimuli, a greater amount of activation over the rostral left inferior parietal lobule (IPL) was observed in response to the images showing body parts receiving painful stimuli vs. faces receiving painful stimuli, suggesting that the processing of others’ body pain activates the specific coding of somatosensory information [11]. These lines of evidence are a reminder that the cognitive and neural mechanisms underlying empathy for face and body pain may differ.
However, most of the reported studies of empathy for pain did not distinguish the cognitive and neural responses between empathy for face and body pain, which may add confusion to the findings of several researchers [3, 12]. Therefore, it is necessary to discriminate the mechanisms underlying these two types of empathy for pain, to understand the cognitive and neural mechanisms of empathy more clearly and deeply.
3 Differences between empathy for face and body pain
ERPs and fMRI are the techniques applied more frequently in previous studies to explore the cognitive and neural mechanism of empathy for pain. Therefore, we mainly summarize the differences between empathy for face and body pain regarding the behavioral reactivity tendency, activation of the brain regions, and electrophysiological [i.e., electroencephalogram (EEG)] signals of the observers.
3.1 Behavioral responses
Empathy for face and body pain may differ regarding behavioral responses, which are modulated by multiple factors. In previous studies, participants usually performed the pain judgment task, e.g., judging whether the person in the images or videos is experiencing pain or not [2, 13]; or the subjective feeling judgment task, e.g., rating their subjective emotional reactions in response to others’ pain [14, 15].
A study of empathy for body pain reported that participants were more accurate and faster in judging images showing body parts receiving painful stimuli compared with images showing body parts receiving non-painful stimuli [9]. However, a study of empathy for face pain showed that the reaction time to the images showing faces receiving painful stimuli was slower than that recorded for the images showing faces receiving non-painful stimuli [8].
Regarding the subjective feeling judgment task, previous studies have reported higher pain intensity ratings and self-unpleasant levels among participants in response to images showing faces receiving painful stimuli compared with images showing faces receiving non-painful stimuli; however, this discrepancy was modulated by the racial information transmitted by the face areas [16]. In turn, studies of empathy for body pain found that the skin color of the body parts affected the participants’ unpleasant ratings associated with images showing body parts receiving painful stimuli, that dark-colored skin causing a higher level of unpleasantness vs. fair-colored skin [17]; however, there was no discrepancy in the pain rating scores among the different types of body skin [18]. This indicates that the group information transmitted through the face and body may be different. Moreover, these lines of evidence suggest that there may be discrepancies among the individual empathic behavioral responses to the images showing body parts or faces receiving painful stimuli.
3.2 Activation of brain regions
Empathy for face and body pain is also related to the activation of different brain regions. The findings of previous fMRI studies showed the activation of distinct areas of the brain between empathy for face and body pain among individuals who were engaged in a similar task, e.g., the pain judgment task. A study of empathy for body pain reported that judgment of others’ body pain activated the ACC, the paracingulate cortex, the right middle frontal gyrus, and several other areas [7]. In turn, a study of empathy for face pain revealed that images showing others’ faces receiving painful stimuli induced a greater amount of activation over the ACC than images showing others’ faces receiving non-painful stimuli did [19].
Another study compared directly the activation of brain regions during the response to images showing others’ body parts and faces receiving painful stimuli, and found that the body images activated a greater number of sensorimotor regions than face images did, including the midline frontal and parietal cortices and the amygdala. In addition, the images showing others’ body parts receiving painful stimuli caused a stronger activation over the left IPL area compared with images showing faces receiving painful stimuli [11]. The differences in the brain areas activated in these experiments indicate that empathy for body pain may cause the brain to encode more soma-motor information, while empathy for face pain may cause more encoding of emotional information.
3.3 Electrophysiological signals
3.3.1 ERP components
The ERP technique is widely used to explore the neural response underlying empathy for pain regarding the time domain because of its high time resolution. In previous studies of empathy for body pain, the N1, P2, and N2 components over the frontal parietal lobe reflected early emotion sharing and pain perception, while the P3 and LPC (late-positive) components over the parietal occipital lobe reflected late cognitive evaluation [9, 20]. These ERP components have been proven to be good indicators of empathy for body pain. The results of a meta-analysis of 40 ERP studies in this field suggested that the centro-parietal P3 and LPC components are relatively stable components that reflect the latestage processing of others’ pain, while the N1 and N2 components probably reflect early-stage processing [12].
However, in addition to the role of the abovementioned ERP components in empathy for body pain, empathy for face pain may also induce N170, a specific component of facial processing [21]. The N170 component over the temporal occipital region reflected the processing of facial structure and the recognition of facial spatial relationships [22]. Moreover, the findings of a recent study of empathy for face pain suggested that greater amplitudes of N170 were induced when participants were instructed to pay attention to facial cues compared with pain cues [8], which indicated that empathy for face pain may be modulated by top-down attention to the pain cues. Another study showed that, after priming with the faces of other people, images showing others’ body parts receiving painful stimuli induced larger early N1 and late P3 components compared with images showing body parts receiving non-painful stimuli [23], whereas smaller N1 and larger P3 components were observed after priming with the faces of friends compared with strangers [24]. These lines of evidence illustrated the relationship between the neural processing underlying the empathy for face and body pain.
3.3.2 Time-frequency analysis
The results of the time-frequency analysis showed that theta oscillations at 3–8 Hz and alpha oscillations at 9–14 Hz reflect the emotionsharing and cognitive control processing of empathy for pain, respectively [25], and the individuals’ perception of others’ body pain relates to the primary somatosensory cortex. A study of the ˜10 Hz neural vibration of the primary somatosensory cortex found that greater suppression is caused by images showing others’ body parts receiving painful stimuli than images showing body parts receiving non-painful stimuli [26].
In addition, the mu suppression induced by the images showing body parts receiving painful stimuli is modulated by emotional states [27], which suggests the existence of a discrepancy between empathy for body and face pain over neural concussion. Some studies have analyzed mu suppression at 8–13 Hz within 2000 ms after the presentation of images showing body parts and faces receiving painful stimuli, indicated that images showing others’ body parts receiving painful stimuli induce a greater mu suppression than images showing body parts receiving non-painful stimuli do; however, there was no difference between the images showing others’ faces receiving painful and non-painful stimuli [28]. Therefore, these results suggest a discrepancy in the neural concussion induced during the processing of empathy for face and body pain.
4 Explanation of the differences observed in empathy for face and body pain
As mentioned above, the differences in the neural mechanisms underlying empathy for face and body pain were caused by discrepancies in the presentation of painful stimuli in the images or video clips. One explanation of this finding is that different cognitive information is transmitted by the two categories of empathy. The images showing faces receiving painful stimuli contain more emotional information, while the images showing body parts receiving painful stimuli contain more perceptual information, which affects the observers’ subjective empathy for pain processing. However, there may be an interaction between pain perception information and emotional information processing. Han and colleagues used video clips of emotional faces with pain (being pricked by a needle) or non-pain (touched with cotton swabs) as stimulation materials to explore the processing mechanism of empathy for face pain under different expressions (happy, neutral, and painful) [19]. They found that, when individuals observed video clips showing faces receiving painful stimuli with happy and neutral expressions, the activation over ACC areas was weakened, whereas the activation over the secondary somatosensory cortex areas was enhanced. These findings suggested that the use of emotional faces as a background to present a painful stimulus can affect the emotional and perceptual responses associated with pain.
Other studies reported that the activation over the left dorsolateral prefrontal cortex associated with cognitive evaluation in the limbic system was enhanced when primed with the negative emotional faces [29], indicating that the empathic processing of others’ pain is possibly influenced by the emotional information transmitted by the faces.
5 Summary and future study
In summary, several lines of evidence from previous studies indicate the presence of discrepancies between empathy for face pain and body pain regarding behavioral responses, the activation of processing regions in the brain, and EEG signals. Possibly, different cognitive information is transmitted by faces and body parts, thus affecting the perception of pain. Moreover, the N170 ERP component (a specific component of facial processing) was induced in the neural processing of empathy for face pain. In addition, a greater number of activated sensorimotor-relevant regions (such as IPL areas) and discrepant mu suppression were observed during the neural processing of empathy for body pain, but were absent during the neural processing of empathy for face pain. This may be explained by the fact that human faces contain more emotional information, while the body parts contain more perceptual information; however, more specific reasons need to be explored. Distinguishing the mechanisms underlying empathy for face and body pain can promote our understanding of the cognitive and neural mechanism of empathy. In particular, it may promote our understanding of the characteristics of empathic neural processing in people with psychopathological disorders. Moreover, it is necessary to pay attention to the following aspects in future research in this filed.
First, although several studies have begun to focus on the differences between these two types of empathy for pain, there is still insufficient evidence to explain it at the level of neural processing. Therefore, painful scenarios can be reasonably set up in future studies to allow the direct comparison of the discrepancies between the two types of empathy for pain from a broader range of aspects.
Second, face is an important part of human appearance, and it can also transmit other social information in addition to emotional information, such as trustworthiness [30] and attractiveness [31]; moreover, it plays a significant role in social communication in our daily lives. Therefore, the impact of other facial features on empathy for pain can be explored in future research, thus promoting our understanding of the neural processing mechanism of empathy for face pain.
Third, individuals with psychopathological disorders, such as autism spectrum disorders (ASDs), exhibit empathy deficits in their daily lives [32] and have abnormal face processing patterns [33]. A study of the empathy for pain among individuals with autism found no discrepancies over the neural response of the empathy for body pain between these individuals and the control group under different attention cues [9]; however, differences were detected between the two groups regarding empathy for face pain [8]. Hence, future studies should explore further the mechanisms underlying the group-specific differences regarding empathy for face and body pain.
Finally, this review has also some limitations. One is that, the constructions of experimental materials used in previous studies are inconsistent, as multiple cues appeared on the images or video clips, and pain-induction methods should be further considered when discussing the different processes underlying empathy for face and body pain, in which the perceptual factors on the images could be controlled well. The other one is that, few studies have focused on the distinctions between empathy for face pain and body pain, with most findings being restricted to healthy individuals, which may have led to the lack of an in-depth explanation of these phenomena and to unfounded conclusions.
Although this article summarizes the distinctions between empathy for face and body pain regarding the painful stimulus and behavioral and neural responses, obviously, it does not represent a complete literature review. More specific explanations for the differences observed and the neuromechanisms underlying them deserve to be reviewed further.
Footnotes
Conflict of interests
All contributing authors have no conflict of interests to declare.
Acknowledgement
This work was supported by the Project Commissioned by the 13th Five-year Plan of Chongqing Education Science in 2019 (No. 2019-WT-28).