
Abstract
Surgical revascularization may be beneficial in patients with ischemic stroke caused by intracranial stenosis or occlusion who are ineligible for thrombolysis.
Objective
To evaluate the outcome of superficial temporal artery to middle cerebral artery (STA-MCA) bypass in ischemic stroke caused by intracranial artery stenosis or occlusion.
Methods
We retrospectively studied successive case series of 19 patients who underwent surgical treatment between 2013–2017 of STA-MCA bypass. Surgical procedure was performed for the patients with acute ischemic stroke who were ineligible for thrombolysis.
Results
Of the 19 patients enrolled, symptom aggravation occurred during medical treatment, the patients were ineligible for thrombolysis despite being within 8 hours of symptom onset. Bypass significantly improved National Institutes of Health Stroke Scale scores, mean patient age was 78.05 years (range, 39–78 y). However, male 11 (57.95%) out of nineteen patients were presented with left-sided-lesions while female 8 (42%) had right-sided lesions with significant infarction growth by diffusion weighted imaging achieved, after surgical maneuver. No major complications occurred intraoperatively, in contrast to 2 (10.5%) minor manifestation were suffering minor complications probably they included the remote infarction (posterior cerebral artery territory). Pooled analysis with our patients showed a significant neurological improvement and a good outcome in 13 (68.4%) patients without hemorrhage or any other complication, 6 (31.6%) patients with unfavorable outcome (severe disability 2; vegetative state 4, non of them are died 0;).
Conclusion
STA-MCA bypass may be beneficial to patients with acute stroke or stenosis in progress who are ineligible for medical therapy. Furthermore, it appears safe when the infarction is small. These findings indicate that STA-MCA bypass could be considered as a treatment option in selected patients with ischemic stroke caused by intracranial stenosis or occlusion.
Introduction
In developed countries the third mortality and disability cause is Ischemic stroke [1–4]. Majority of ischemic strokes are thromboembolic originally, due to an intracranial artery stenosis or occlusion clotting, blocking blood flow to the brain. Those patients who are suffering from ischemic stroke can be treated pharmacologically with intravenous tissue plasminogen activator (tPA) if patients present within 4.5 hours of symptom onset [5]. Labeling of subtypes of ischemic stroke has had significant studies, but characterizations are difficult to verbalize and their presentation for conclusion in an individual patient is frequently difficult. In the past, categorizations have been based on risk factor profiles primarily, clinical manifestation of the stroke, and findings on brain imaging studies (computed tomography (CT) or magnetic resonance imaging (MRI)) [6]. However, clinical and brain imaging overlap features are not specific for any particular subtype of ischemic stroke. Bamford et al. [7] newly reported the results and probability of recurrent stroke varied significantly by stroke subtype; enormous hemispheric infarcts, mostly ensuing from occlusion of the internal carotid artery or proximal middle cerebral artery, had the worst prognosis. Based on clinical features investigators classified the strokes which forecasted the site and size of the ischemic lesion, but potentially they didn't consider etiology of the stroke. Other researchers have noticed that the etiology of stroke can effect prognosis. Sacco et al. [8] point that higher mortality was among patients with large-artery atherosclerotic lesions than among patients with lacunar stroke. Recurrent strokes are more probable among patients with cardioembolic stroke than patients among with stroke of other causes [9]. Mortality rate is higher after cardioembolic stroke during period of 1-month than that with strokes of other etiologies [10,11]. The Stroke patients with large artery occlusions can be treated with a variety of endovascular techniques in addition to intravenous thrombolysis. Recently several options including intra-arterial thrombolytic, mechanical thrombolysis, and/or embolectomy with devices such as the Merci retrieval system or the Penumbra device are available [12,13]. Therefore, the main management of ischemic stroke is endovascular or medical, rather than surgical. Ischemic stroke caused by thromboembolism due to atherosclerotic plaque in a symptomatic cervical internal carotid artery is surgically treated by carotid endarterectomy.
But there are some ischemic strokes due to vast chronic circumstances that gradually reduce cerebral blood flow in the lack of compensatory indemnity circulation. Bypass surgery, first bypass is done by Yasargil, in 1967, succeeded for an embolism of the middle cerebral artery by means of a superficial temporal artery to middle cerebral artery anastomosis (STA-MCA anastomosis) [14]. Thereafter it has been called extracranial to intracranial bypass (EC-IC bypass). Although bypass moderations have resolved the majority of the occlusion, therefore, we have brought alteration.
Direct Bypass (Direct anastomosis) in which donor artery and an intracranial recipient artery delivering blood flow to the brain (
Indirect Bypass (Combined procedure).

Donor artery anastomosed into intracranial recipientrtery delivering blood flow to the brain. Copyright © 2015, SpringerVerlag Berlin Heidelberg. Permission for this acclimatization has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the interpretation or adaptation.
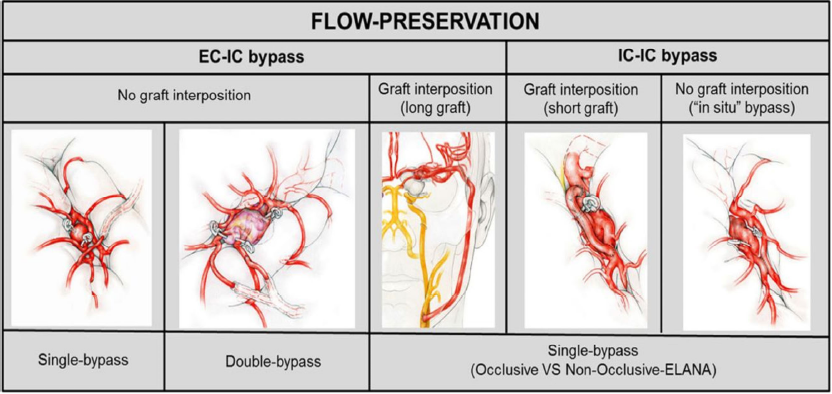
Illustration of flow preservation bypasses. EC–IC indicates extracranial-intracranial; IC–IC indicatesintracranial-to-intracranial [15].
Amended with authorization from Esposito et al. with approval of the publisher.
We retrospectively studied successive case series of 19 patients who underwent surgical treatment between 2013–2017 of STA-MCA bypass. Surgical procedures were performed for the patients with acute ischemic stroke who were ineligible for thrombolysis. To evaluate the outcome of superficial temporal artery to middle cerebral artery (STA-MCA) bypass in acute stroke and stroke in progress, with cortical selective-targeted EC-IC bypasses is presented. All patients were operated on by the senior Doctor Prof. Lukui Chen in Zhongda Hospital Medical Center, affiliated with Southeast University, Nanjing China, over aperiod of 48-month. The characteristics of patients and treatments are detailed in
Demographic data of 19 patients underwent cerebral bypass.
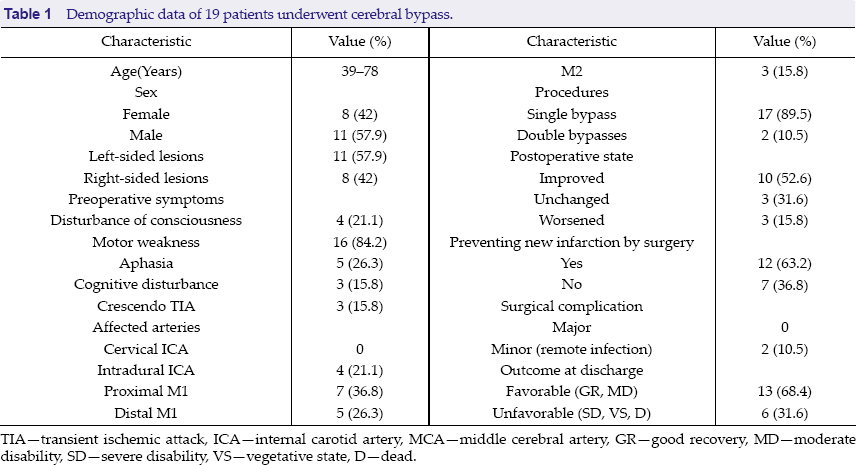
Demographic data of 19 patients underwent cerebral bypass.
TIA—transient ischemic attack, ICA—internal carotid artery, MCA—middle cerebral artery, GR—good recovery, MD—moderate disability, SD—severe disability, VS—vegetative state, D—dead.
Selected patients underwent preoperative computed tomography angiography (CTA) and/or digital subtraction angiography (DSA) with 3-D reconstructions to optimally define the anatomy. Control angiography (CTA or DSA) was performed in the first 12th hours after surgery and follow-up (CTA) was done at 3 months (except in case 5). Functional health of all patients was assessed preoperatively and at 3-month follow-up by modified Rankin Scale (mRS).
The most common operative technique described in the literature is the STA-MCA anastomosis [16–21]. Variations of the EC-IC bypass procedure have also utilized the occipital, auricular, middle meningeal, common carotid, external carotid, and subclavian arteries as donor vessels and the anterior cerebral, posterior cerebral, posterior inferior cerebellar, and superior cerebellar arteries as recipient vessels [16,18,22,23]. The operative procedure used for the bypass is essentially unchanged since reported by Donaghy et al. [24]. Prior to intubation, an arterial line wasinserted for general anesthesia constantly monitor blood pressure. Swan-Ganz flow-directed balloon-tipped catheter was placed percutaneously inneurological unstable patients, to monitor and maintain fluid balance within cardiovascular function closely during and after the operation. Usually the catheter was placed just before the operation in those patients whose heparin anticoagulation had been discontinued several hours prior to surgery. A Foley catheter was inserted to monitor urinary output and to allow the use of osmotic diuretics during the surgery. A lumbar catheter was inserted for intraoperative cerebrospinal fluid (CSF) drainage. It is critical that the CSF drainage should be functional because of the necessity for retraction and elevation of the temporal lobe in order to reach the tentorial incisura. The patients were placed supine with the right shoulder and hip elevated and the head horizontal, hyperextended, and the left side down. The right side was always used to avoid retraction of the temporal lobe on the dominant side. Both anterior and posterior branches of the STA were traced on the scalp with the use of a directional flow Doppler probe. The anterior branch was preferred for use in the anastomosis. It was traced from the area anterior to the pinna to the most distal portion visualized on the angiogram, usually for 8 to 10 cm or more. The scalp was shaved and prepared with povidone-iodine solution in the usual manner. A direct incision was made over the STA (
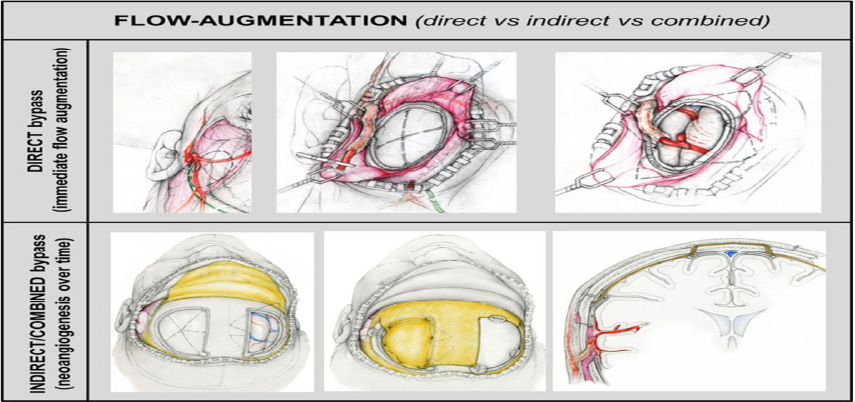
Flow intensification strategies. Left, Direct (superficial temporal artery to middle cerebral artery “STA–MCA”) bypass. Right, Combined revascularization consisting ofunilateral “STA–MCA” bypass plus encephalo-duro-myo-synangiosis and bifrontalencephaloduro- periosteal-synangiosis [15].
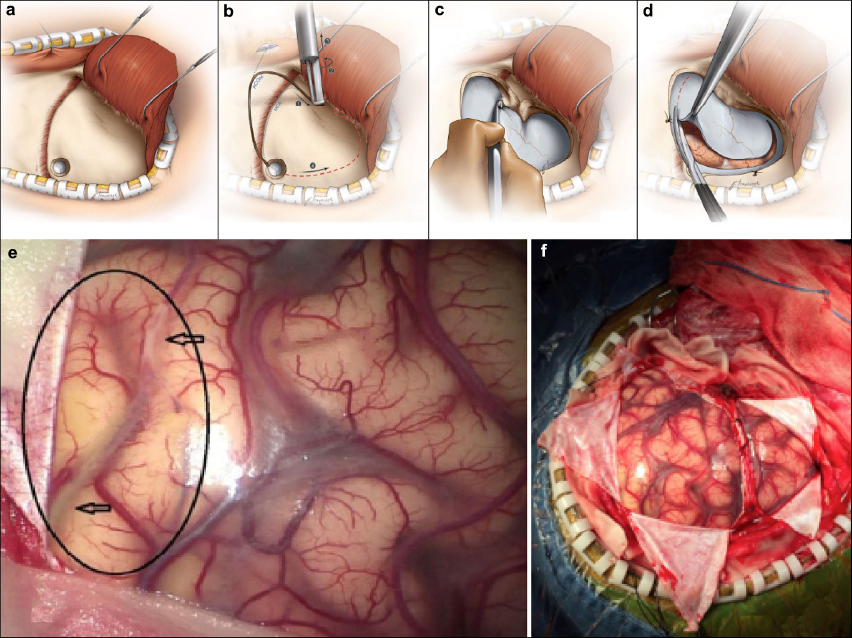
(a) The temporalis muscle was elevated from the bone with Bovie electrocautery and reflected with the scalp flap anteriorly in one musculocutaneous layer; (b) A burr hole was placed just inferior to the posterior aspect of the superior temporal line, abutting the skin incision, and a standard pterional craniotomy flap was elevated and extended just lateral to the midpupillary line; (c) To maximize exposure and minimize frontal lobe retraction, the lateral aspect of the sphenoid ridge was drilled away as far as the superior orbital fissure; (d) The dura was incised by using a C-shaped durotomy; (e) Occluded segment; (f) During surgery.
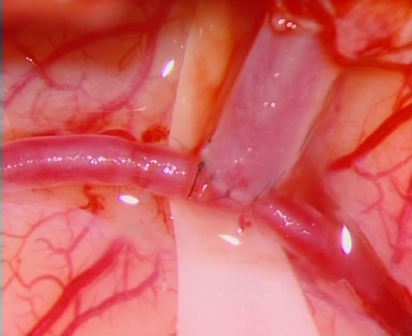
The superficial temporal artery was anastomosed end- to-side to the temporarily occluded segment of the cortical artery.
Clinical and demographic data of 19 patients were summarized in
Complications during periods of perioperative are presented in
Discussion
The surgical effectiveness of endeavor is judged by its ability to favorably influence the natural history of a given disease. Thus, the merit of the cerebral bypass procedure in the treatment of cerebral ischemia must be determined by a comparison with the natural history of cerebrovascular disease. The most important findings of the present study are twofold. First, in patients with ICA occlusion, the flow territory of the EC-IC bypass is smaller compared with the flow territory of the ICA on the contralateral side. Second, cerebral perfusion of the brain tissue supplied by the EC-IC bypass is unchanged compared with tissue perfusion of the contralateral hemisphere and tissue perfusion of control participants.
Several surgical reperfusion methods have been used to treat patients with acute ischemic stroke, or stroke in progress for many decades, but outcomes range from encouraging to disappointing [26]. The most important reason for these mixed results is that patients could not be selected for surgical treatment by multimodal MR or CT, which is usually performed nowadays. Today, using advanced imaging techniques, we can understand the mechanisms of symptom development or fluctuation and select candidates likely to benefit from urgent reperfusion. Efforts to identify potentially salvageable brain tissues using advanced imaging techniques and to increase the proportion of patients with acute ischemic stroke that receive treatment are not limited to endovascular treatment, but are applicable to all types of reperfusion methods, including surgical revascularization. Therefore, we think that the patient selection using multimodal MRI for STA-MCA bypass was the most important factor to achieve the good outcome in our study. The first notable finding of our study and of the pooled analysis is the effect of STA-MCA bypass. Because STA-MCA bypass cannot improve perfusion status in the entire affected area to the previous status immediately after surgery, its main role is to maintain cerebral blood flow in the ischemic region above the level of the threshold of pump failure, which can prevent irreversible damage until sufficient collaterals have been established after major arterial occlusion, and sometimes restore the neurological status. Practically, CT perfusion imaging at 7 days postoperatively showed relatively large areas with MTT prolongation compared with contralateral sides, but tissues at risk (the region with a relative MTT of 145% of that of the contralateral side) were much reduced after STA-MCA bypass. Accordingly, in the present study, ENI was observed in patients within 3 days of bypass surgery, and all patients with ENI that benefited from STA-MCA bypass achieved a good functional outcome. Furthermore, no significant growth in infarction size was observed by follow-up DWI. In our pooled analysis, neurological status was found to be significantly improved by bypass and a good functional outcome was achieved by 83.3% of patients. These findings suggest that STA-MCA bypass may be beneficial to patients with acute stroke or stroke in progress. The second finding of note is the lack of a reperfusion-induced complication of STA-MCA bypass. In the late period beyond the standard time window, high-flow antegrade reperfusion may induce hemorrhage in brain tissue with EIC. Endovascular recanalization showed a high rate of hemorrhage, up to 33.3% in a report for delayed procedures [27]. Compared with blood flow furnished by endovascular recanalization (about 150 mL/min for M1), STA-MCA bypass provides less amount of blood flow (20.60 mL/min), and such a relatively small amount of flow augmentation seems to have less risk for reperfusion-induced hemorrhage. Following STA-MCA bypass in acute stroke, there has been no reperfusion-induced complication in most previous reports [28,29], although one CT-based study reported asymptomatic brain edema and hemorrhage associated with STA-MCA bypass in low-density lesions on preoperative CT scan in 3 and 1 of 19 patients, respectively [30]. We also encountered no surgical complication or hemorrhage in the present study and collective analysis, especially including patients with ischemic stroke outside of the 6 to 8-hour time frame. Therefore, STA-MCA bypass appears to be safe in carefully selected patients with acute stroke or stroke in progress beyond the standard time frame. The infarction volumes for our 5 patients were small, and thus, their natural courses may have been benign. However, all patients showed a moderate to severe neurological severity just before surgery and, especially, no patients with mild severity in the acute stage showed symptom aggravation and infarction progression, despite maximum medical therapy. Several authors concluded that this stroke in progress is associated with a poor outcome [31]. The European Progressing Stroke Study Group reported that patients with neurological deterioration showed a significantly higher rate of poor outcome (77%) than patients without neurological deterioration (30%) [32]. Additionally, one prospective study demonstrated that for each 10 cm, 3 of infarction volume growth, the odds ratio for achieving an excellent outcome by mRS and the Barthel Index was 0.52 and 0.64, respectively [31]. These results indicate that stroke progression worsens the prognosis of patients with ischemic stroke. Therefore, we believe that reperfusion treatment was urgently needed to prevent more aggravation and impact on recovery in patients enrolled in our study. The present study has several limitations. Its major limitations are its retrospective nature, and the lack of a control group. According to the treatment protocol at our institute, patients with acute stroke or stenosis in progress are considered for revascularization treatment. Few patients did not undergo any type of reperfusion therapy at our institute and, therefore, it was not possible to recruit controls. In addition, we used MR perfusion for initial evaluations, but during follow-up, CTA was used to check revascularization status, and thus, revascularization improvements observed after surgery were not the result of direct quantitative comparisons. Finally, this study is limited by the small number of patients recruited, and for this reason, the sample size limitation prevents our drawing firm conclusions, thus, we propose that a large prospective study be conducted to confirm the effectiveness and safety of STA-MCA bypass in acute ischemic stroke.
Conclusions
Because cerebral bypass surgery is one of the best selective revascularization method used in acute ischemic stroke caused by intracranial artery stenosis or occlusion, it should be considered as the first treatment technique in cases which require urgent revascularization. However, our series of 19 patients and our pooled analysis demonstrate that STA-MCA bypass may be beneficial to patients with acute ischemic stroke or occlusions in progress in whom medical therapy failed. Additionally, the low flow provided by STA-MCA bypass appears safe in cases with a small infarction. Accordingly, our findings indicate that STA-MCA bypass could be considered a treatment option in selected patients with acute ischemic stroke or stenosis in progress.
Footnotes
Acknowledgements
This research was supported by Southeast University affiliated Zhongda Hospital, Nanjing, China. The authors are thankful for colleagues in Zhongda Hospital who provided insight and expertise that greatly assisted. Especially thanks Professor Chen Lukui for data evaluation and technical assistance with methodology and comments that greatly improved the manuscript.
The authors have no conflicts of interest to declare.