
Abstract
Anaphylactic insults that cause cardiovascular signs and symptoms have been defined as Kounis syndrome, which has been associated with specific triggered anaphylactic reactions. Kounis syndrome has not been described in patients with no evidence of coronary artery disease (type I Kounis) in a scenario of idiopathic anaphylaxis. We reported a case of a 65-year-old white woman with no evidence of coronary artery disease who experienced two myocardial infarctions on separate occasions attributable to idiopathic anaphylaxis.
Case Presentation
A 65-year-old white woman with a history of malignant idiopathic anaphylaxis, presented to the emergency department 20 minutes after injecting herself with epinephrine for an anaphylaxis episode. Malignant idiopathic anaphylaxis concerns patients with the most severe form of idiopathic anaphylaxis that is resistant to standard therapy. Episodes of idiopathic anaphylaxis are not controlled when prednisone is reduced below at least 60 mg every other day or 20 mg daily. 1 The patient's condition was previously stable on daily prednisone 30 mg and Xolair (Genentech, South San Francisco, California), after failed attempts to completely wean her off corticosteroids over a span of several years. Cardiac enzymes showed an initial serum troponin I level of 0.07 ng/mL (reference value, <0.02 ng/mL; range 0.00–0.03 ng/mL) and unchanged electrocardiography. A 3-hour repeated troponin I test result was elevated, at 0.46 ng/mL, and the patient was admitted for observation. Further cardiac workup was not obtained, and the patient was discharged the following day in stable condition.
One month later, the patient presented to the emergency department after experiencing severe substernal chest pain. The pain was described as sudden pressure-like chest pain associated with nausea, dyspnea, diaphoresis, and near syncope. Epinephrine was not administered to the patient. On arrival to the emergency department, the patient's physical examination was unremarkable, with the exception of facial flushing. The chest pain was alleviated with sublingual nitroglycerin, 1-inch nitro paste placed on the chest, and aspirin. Cardiac enzymes showed a troponin level of 0.08 with unremarkable creatine phosphokinase, creatine kinase myocardial b fraction, and creatine kinase myocardial b fraction percent. The D-dimer level was 0.84 mg/L. Results of an echocardiography and further evaluation for pulmonary embolism and acute dissection were negative. The patient was admitted to the hospital for further cardiac evaluation. Her troponin I level peaked at 0.08 ng/mL and trended down, to 0.05 ng/mL. Computed tomography angiography demonstrated the presence of normal coronary anatomy (Fig. 1), without evidence of atherosclerotic changes or stenotic disease. The patient received 3 days of loratadine and famotidine, and did not experience further episodes of chest pain or other anaphylactic symptoms.
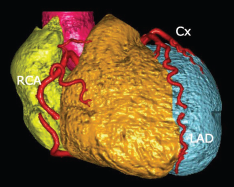
Image of our patient's computed tomography angiogram of the heart demonstrated no evidence of coronary artery disease, which makes this case consistent with the type I variant of Kounis syndrome. RCA = Right coronary artery; Cx = circumflex artery; LAD = left anterior descending artery.
Discussion
Anaphylaxis is an immediate hypersensitivity reaction that causes an immunoglobulin E-mediated release of mast cell and basophil mediators, including histamine, cytokines, prostaglandins, leukotrienes, tryptase, chymase, and platelet-activating factor. These inflammatory mediators act systemically on multiple organ systems, including the cardiovascular system. In addition to peripheral vasodilation, these inflammatory mediators can act directly on the heart and lead to coronary artery vasospasm, ischemia, and/or erosion or rupture of an atheromatous plaque in the presence of an allergic insult.2,3
The mechanism by which anaphylaxis results in acute coronary syndrome in patients with and those without atherosclerosis has been defined. Cardiac mast cells are present in the internal layer and around the coronary vessels as well as between cardiomyocytes in healthy human hearts. Mast cell receptors present on cardiac mast cells mediate the anaphylactic reaction through the activation of a complement and subsequent to anaphylotoxin generation. 4 The release of histamine, tryptase, and chymase through mast cell de-granulation subsequently ensues. In addition, mast cells are found in amounts proportional to the extent of atherosclerotic changes in those with CAD. 4 Coronary arteries with evidence of atherosclerosis are found to be more susceptible to vasoconstriction by catecholamines and histamine. Specifically, atherosclerotic vessels contain twice as much histamine as unchanged adjacent segments, and histamine contracts these diseased vessels 1000 times stronger than healthy vessels. This contraction of vascular walls leads to thrombus erosion or rupture. This increase in mast cells and histamine as well as the heightened allergic response in atherosclerotic vessels may contribute to the apparent increased prevalence of certain types of Kounis syndrome cases.
Conclusion
Three variants of Kounis syndrome have been described in the literature. The type I variant includes patients without a history of CAD who experience coronary vasospasm that results in positive or negative cardiac biomarkers. 5 Type II Kounis syndrome includes patients with preexisting atheromatous disease in which an allergic insult renders the plaque unstable, which causes it to erode or rupture. The last variant of Kounis syndrome, type III, includes patients who experience stent thrombosis secondary to an allergic insult. Although, to our knowledge, no epidemiologic data exist regarding the relative frequency of the various Kounis syndrome types, reported cases often result in the identification of significant coronary artery blockage. In a study of eight patients admitted with acute coronary syndrome after a Hymenoptera insect sting in the preceding 48 hours, all who underwent coronary angiography were found to have at least one coronary artery narrowing of > 70%. 6 In addition to occurring less commonly, type I Kounis syndrome has primarily been reported in the presence of a known, identifiable trigger. To our knowledge idiopathic anaphylaxis that results in a type 1 Kounis has not been reported. We presented a unique case of type I variant Kounis syndrome caused by idiopathic anaphylaxis in the same patient on two separate occasions.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article