
Abstract
Objective:
To investigate the factors that influence oral intake in the first 24 hours following tonsillectomy in children performed for Obstructive Sleep Apnea (OSA) and their impact on dehydration in the 30-day post-operative period.
Methods:
A retrospective cohort study was conducted reviewing the records of 1200 patients who underwent tonsillectomy. Patients were excluded if they were 19 years or older, did not have a diagnosis of SDB (sleep disordered breathing) or OSA (obstructive sleep apnea), or their oral intake was not recorded for 24 hours post-operatively. Primary outcomes were 24-hour post-operative oral intake controlled for body weight and post-operative dehydration determined by ED visits or phone calls for dehydration within 30 days post-operatively.
Results:
357 patients were included. Higher BMI (body mass index; r = −.261) older age (r = −.393), longer operative time (r = −.125), longer time under anesthesia (r = −.186), higher apnea-hypopnea index (AHI; r = −.171), higher pain scores (r = −.239), and the presence of a resident (P = .028) were all significantly associated with lower oral intake. Post-operative oral intake did not have a significant effect on post-operative dehydration events (OR = 0.995, 95% CI [0.975-1.015]).
Conclusion:
Our findings suggest that age, BMI, operative time, time under anesthesia, AHI, pain, and the presence of a resident were significantly associated with post-operative oral intake following tonsillectomy. Post-operative oral intake was not associated with dehydration in the 30-day surgical recovery period.
Introduction
Over 500 000 tonsillectomies are performed each year in the United States, the majority of which are performed in the pediatric population. 1 Of those, 67% are performed for obstructive sleep apnea (OSA) and 17% for chronic tonsillitis. 2 The revisit rate to the emergency department (ED) and readmission rate following tonsillectomy in pediatric patients is 4.9% to 10.11% and 1.27% to 16.7% respectively, most commonly for decreased oral intake (16.7%-55.6%), followed by post-tonsillectomy hemorrhage (21.3%-83.3%), and vomiting (2.3%-13.6%).3-8 Poor oral intake post-operatively is widely accepted to occur secondary to pain or post-anesthesia effects such as nausea. 9 It is unclear whether alternative factors such as age, body mass index (BMI), the presence of a resident during surgery, concurrent surgeries performed, pre-operative apnea-hypopnea index (AHI), post-operative pain scores, operative time, time under anesthesia, and device used influence post-operative oral intake. It is also unclear if initial 24-hour post-operative oral intake correlates with rates of dehydration requiring revisit or readmission in the subsequent healing period following tonsillectomy surgery.
Messner and Barbita conducted a prospective cohort study of 200 patients following tonsillectomy, where 100 patients were required to drink 20 cc/kg before discharge and 100 patients did not have to drink before discharge, and they found no difference in rates of dehydration between the groups. 10 Another study by Rohlfing et al 11 found no correlation between post-tonsillectomy oral intake from the end of surgery until discharge and ED revisits, with n = 475, odds ratio = 1.03, and 95% CI = .98 to 1.08. The readmission rate for dehydration following tonsillectomy in children is reported to be between 1.5% and 6%.5,7,8 Several other studies have investigated post-operative oral intake after tonsillectomy and found no correlation with nausea, vomiting, post-operative pain, or dehydration.8,10,11 However, factors such as time under anesthesia, operative time, presence of a resident during surgery, and the effect of these factors on oral intake and ED visits for dehydration have not been significantly explored in the existing literature.10-14
Yin et al 15 investigated children undergoing general anesthesia for a variety of surgeries and found that early oral intake of <5 mL/kg was associated with increased patient satisfaction according to patient administered surveys when compared to no oral intake for the first 4 hours post-operatively. Previous studies on post-operative oral intake following tonsillectomy have reported that the use of dexamethasone in the peri-operative period decreases post-operative pain, nausea, and vomiting, and increases oral intake, suggesting that a correlative relationship between pain, nausea, vomiting, and 24-hour oral intake might exist.12-14
The purpose of our study was to examine factors that may impact oral intake in children in the first 24 hours following tonsillectomy performed for OSA or sleep disordered breathing (SDB). In addition, we investigate whether any of these factors, including 24-hour oral intake post-operatively, impact ED revisit rates and office phone calls for dehydration following tonsillectomy. We hypothesized that older age, higher BMI, and higher pain scores would be correlated with decreased oral intake. Furthermore, we believed that decreased 24-hour post-operative oral intake would be associated with higher rates of dehydration in the month following tonsillectomy, defined as an ED visit or documented office phone call for dehydration.
Methods
After obtaining approval from the Cooper University Hospital’s Institutional Review Board, a retrospective review was conducted using the division of otolaryngology’s tonsillectomy registry database. The database included records of all patients who underwent tonsillectomy at our institution from July 2016 to December 2021. About 1200 records were reviewed from the database to determine patients for inclusion in this study. Patients were excluded based on the following criteria: age 19 years old or older, indication for tonsillectomy other than OSA or SDB, and same day surgery discharge without 24-hour post-operative admission or subsequent record of oral intake.
Data collected included oral intake measured in mL of liquid consumed per kg of bodyweight, demographics such as age, gender, weight (in kilograms), insurance status, primary language, preoperative BMI, preoperative AHI, as well as indications for surgery, dexamethasone dose and frequency received, post-operative pain score, tonsillectomy instrument used, time under anesthesia, operative time, presence of resident during surgery, anesthetic agent used, and whether concurrent procedures were performed (cerumen disimpaction or myringotomy tube placement). All patients underwent an extracapsular tonsillectomy as opposed to the intracapsular tonsillectomy or tonsillotomy. Nearly all patients had adenoidectomy performed concurrently, so adenoidectomy was not investigated as a predictor for 24-hour oral intake. Additionally, the incidence of post-operative dehydration was collected either by a documented phone call from a parent reporting decreased oral intake, or an ED visit for decreased oral intake or signs of dehydration.
Post-operative pain scores were calculated using both the Wong Baker FACES and FLACC pain scales and were collected and recorded by nurses or providers. Both scales are rated 1 to 10 in terms of severity. The FACES scale uses a sheet of paper with faces that allows patients to identify the face that represents their level of pain. 16 FLACC assesses pain by visualizing the patient’s face, legs, activity level, cry and consolability for signs of discomfort and rates each category 0, 1, or 2, making the highest possible rating a 10. 17
Regarding intraoperative data, each patient’s surgical report was reviewed to record operative time and time under anesthesia. Operative time was described as the time from the incision until the end of surgery, usually marked by completion of orogastric tube suctioning. Time under anesthesia was described as the time from induction of anesthesia to extubation. Using flowsheets that document oral intake, each patient’s 24-hour post-operative oral intake was calculated to determine intake in mL/kg. Anesthetic agent and dexamethasone dose and frequency were obtained from the medication administration records; post-operative dexamethasone is standardized within the pediatric tonsillectomy post-operative order set at our institution which includes 2 doses of 0.2 mg/kg every 6 hours. For any patients whose weight exceeded the maximum allowable dose of decadron, a max of 10 mg was administered every 6 hours. Antibiotics are not routinely given intraoperatively during tonsillectomy and thus were not recorded as part of this study.
Descriptive statistics were calculated using SPSS 27 (IBM, Armonk, NY). Correlation coefficients were obtained between oral intake and BMI, age, operative time, time under anesthesia, pain scores, and AHI with the Spearman Rho Correlation. Mann Whitney-U tests were performed to determine the relationships between oral intake and the presence of a resident, the surgical device used, and the concurrent performance of other procedures including myringotomy, and cerumen removal (categorical values). Independent t-tests were also performed to determine the relationship between BMI and age. Logistic regression was performed and odds ratio (OR) estimates with 95% confidence intervals (CI) were calculated to assess the association between 24-hour oral intake and the presence or absence of post-operative dehydration.
Results
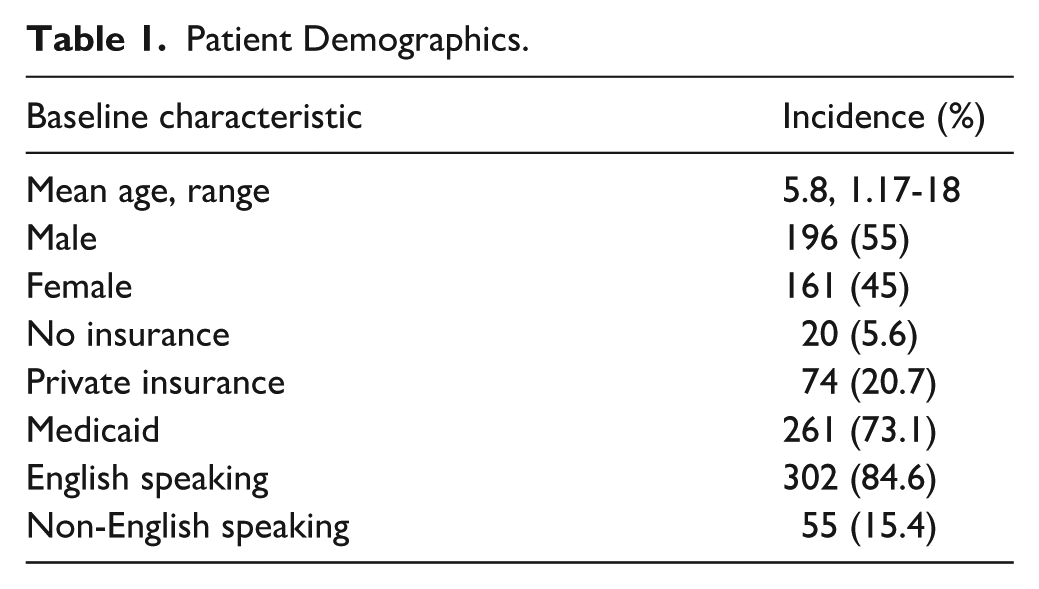
A total of 357 patients met inclusion criteria. This included 196 (55%) males and 161 (45%) females. The age ranged from 14 months to 18 years, with an average age of 5.8 years. 261 (73%) patients had Medicaid, 74 (21%) had private insurance, and 20 (6%) were uninsured. There were 302 (85%) English speaking subjects and 55 (15%) whose primary language was something other than English including Spanish (n = 48), Portuguese (n = 4), Korean (n = 1), Turkish (n = 1), and Vietnamese (n = 1). The demographics of our study population can be seen in Table 1. Sixty-nine patients (19.3%) underwent concurrent myringotomy and 20 (5.6%) underwent cerumen removal, and 350 (98%) patients underwent adenoidectomy. Oral intake was recorded in mL/kg.
Patient Demographics.
Patient and Perioperative Factors
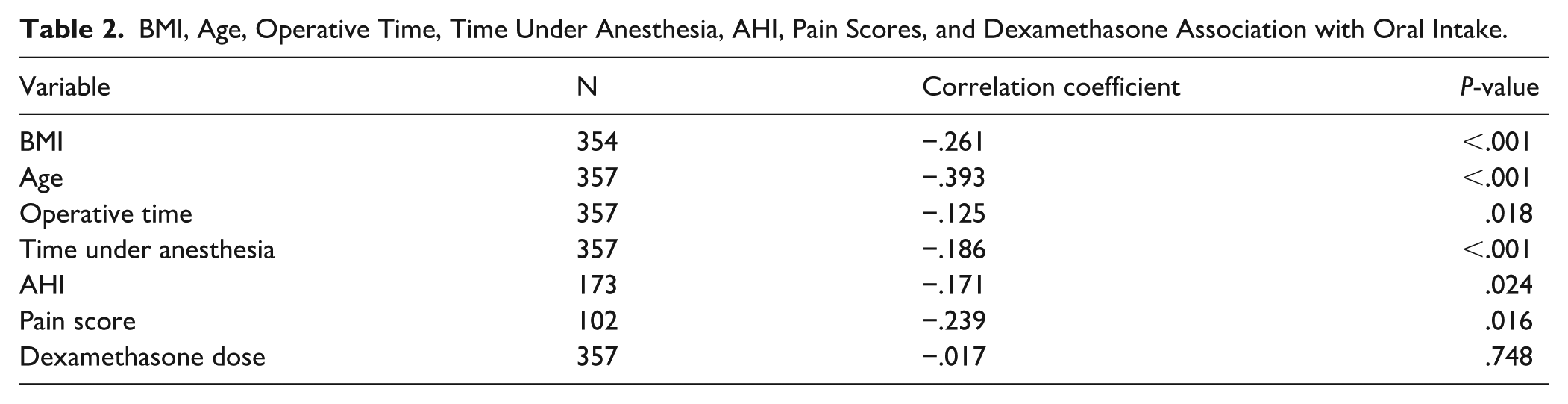
A higher BMI and older age were associated with a lower volume of oral intake per body weight (correlation coefficient r = −.261 [P < .001]; r = −.393 [P < .001], respectively). A longer operative time and longer time under anesthesia were both significantly associated with a lower oral intake with correlation coefficients of −.125 (P = .018) and −.186 (P < .001), respectively. A higher AHI was statistically significantly associated with a lower oral intake with a correlation coefficient of −.171 (P = .024). Post-operative pain scores were recorded for 102 patients (29%) using either the Wong Baker FACES score or the FLACC score. Higher pain scores were significantly associated with decreased oral intake, with a correlation coefficient of −.239 (P = .016). The number of dexamethasone doses administered to patients was not correlated with oral intake (r = −.017 [P = .748]). These values can be seen in Table 2.
BMI, Age, Operative Time, Time Under Anesthesia, AHI, Pain Scores, and Dexamethasone Association with Oral Intake.
Surgical Factors
For 59 (16.5%) of the tonsillectomies in our cohort, a resident was present in the case. The presence of a resident was associated with a lower oral intake, with a median intake of 19.6 mL/kg in the group with a resident present and 25.8 mL/kg in the group without (P < .028; Table 3). The presence of a resident was associated with a longer operative time, as median operative time for the group with a resident present was 30 minutes, while the median operative time for the group without a resident present was 25 minutes (P < .001). Increased operative time was significantly associated with decreased oral intake.
Presence of a Resident, Device Used, and Additional Procedures Association with Oral Intake.
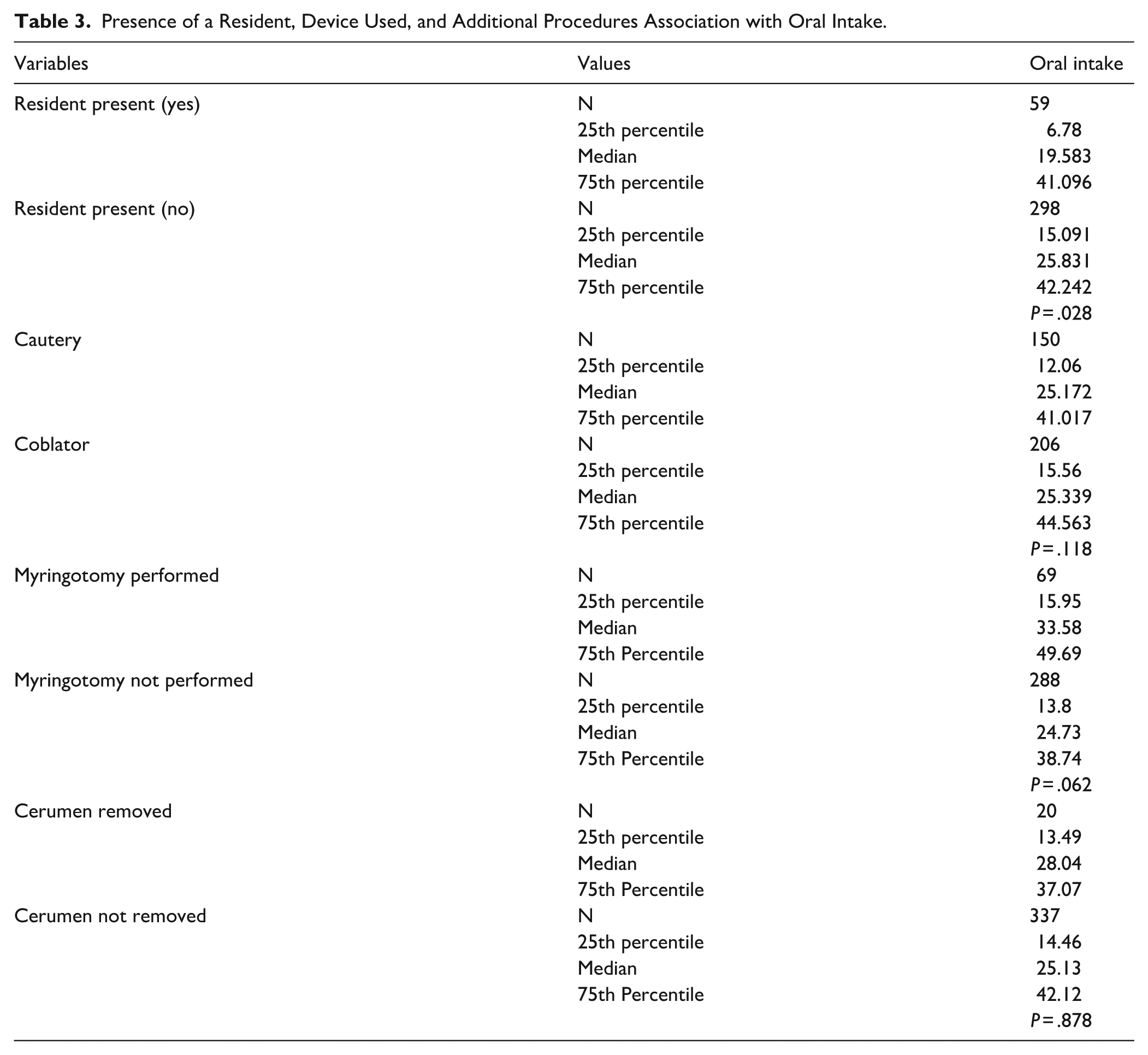
A coblator was used in 206 (58%) tonsillectomies while cautery was used in 150 (42%). There was no significant difference in oral intake between these 2 groups, as the median oral intake was 25.3 mL/kg for the coblator group and 25.2 mL/kg for the cautery group (P = .118; Table 3). Operative time also did not differ between groups (P = .554).
The performance of concurrent surgeries did not have a significant impact on oral intake. Myringotomy tube placement was performed in 69 (19%) of our patients concurrently. Those with myringotomy tube placement had a median oral intake of 33.6 mL/kg while those who did not had a median oral intake of 24.7 mL/kg (P = .062). Twenty (6%) of our patients underwent cerumen removal with tonsillectomy, with a median oral intake of 28 mL/kg, while those who did not undergo cerumen removal had a median oral intake of 25.1 mL/kg (P = .878).
Dehydration
Odds ratios (OR) were calculated to examine the association between volume of oral intake and presence of dehydration events. A total of 20 patients (6%) met our criteria for dehydration, which included ED visits and post-operative phone calls related to dehydration in the 30 days following surgery. Of these, 15 patients came to the ED, while 5 patients contacted our office via phone. The amount of 24-hour post-operative oral intake did not have a significant effect on post-operative dehydration events in the subsequent recovery period (OR = 0.995, 95% CI [.975-1.015]). Additionally, there was no significant difference when this group was broken down into ED visits (OR: 0.987, 95% CI [.961-1.013]) or phone calls (OR: 1.01, 95% CI [.983-1.039]) as seen in Table 4.
Univariate Analysis of Oral Intake and Dehydration.

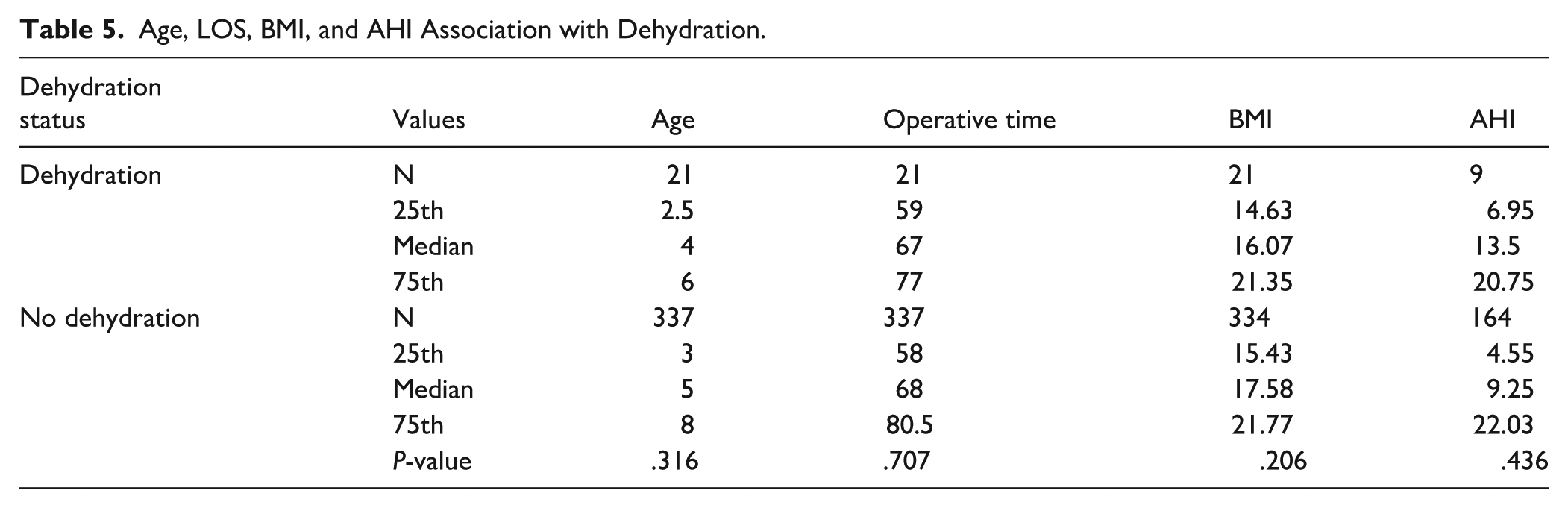
Age, operative time, BMI, or AHI were not significantly associated with dehydration. For patients who presented with dehydration compared to those without dehydration, median age (4 years vs 5 years, P = .316), LOS (67 minutes vs 68 minutes, P = .707), BMI (16 vs 18, P = .206), and AHI (13.5 vs 9.25, P = .436) were all similar (Table 5).
Age, LOS, BMI, and AHI Association with Dehydration.
Discussion
The purpose of this study was to identify the factors that impact oral intake in the first 24 hours following tonsillectomy performed for OSA in children, as well as factors associated with dehydration after the initial 24-hour post-operative period. Results from this analysis can yield insight into factors that can be modified to increase oral intake following tonsillectomy, and potentially improve post-operative pain and patient satisfaction as they relate to oral intake.
Higher BMI and older age were both associated with lower oral intake. As BMI increases in children, their oral intake, as measured in mL/kg, tends to decrease. This is likely due to an incongruent fluid intake to weight ratio as BMI increases. 11 Increasing age is also associated with lower oral intake. This is consistent with a previous study that investigated oral intake following tonsillectomy. 11
A higher level of post-operative pain measured with the Wong Baker FACES score and the FLACC score was associated with lower oral intake. Oropharyngeal pain causing decreased oral intake is a recognized driver of morbidity in children following tonsillectomy.18,19 Additionally, Yin et al 15 found that increased early oral intake increases patient satisfaction post-operatively. These findings suggest that oral intake is a surrogate marker for immediate post-operative pain control and satisfaction post-operatively.
It has been well documented that the use of peri-operative dexamethasone 0.5 to 1 mg/kg improves oral intake following tonsillectomy when compared to children who did not receive dexamethasone.20-24 Kang et al 25 found that intraoperative dexamethasone 0.5 mg/kg decreases post-operative pain and decreases post-operative nausea and vomiting. All of the patients included in our study received intraoperative intravenous decadron 0.1 mg/kg, so it was not possible to compare the oral intake of patients who did not receive decadron. In addition to intraoperative decadron, our patients received 1 to 4 doses of post-operative decadron 0.1 mg/kg every 6 hours while admitted. The number of additional doses of decadron was not significantly associated with changes in oral intake.
Longer time under anesthesia and longer operative times were both correlated with lower oral intake. Studies have shown that longer time under anesthesia is correlated with higher rates of post-operative nausea and vomiting, and this can lead to lower oral intake. 26 The use of intraoperative decadron has shown to be effective for decreasing post-operative nausea and vomiting; however, prolonged time under anesthesia still increases the risk of developing nausea and vomiting even when administering decadron. Pediatric patients typically underreport nausea secondary to anesthesia, so these effects can have an impact even when it is not reported by patients and may present as a refusal of oral intake. 27
Due to the association between operative time and time under anesthesia, separate analyses were conducted regarding oral intake versus operative time and oral intake versus time under anesthesia. Both longer time under anesthesia and longer operative times were significantly associated with lower oral intake, with longer time under anesthesia having a stronger correlation (−.186 vs −.125).
The presence of a resident during surgery was correlated with lower oral intake when compared to patients who had surgery with no resident present. Prior studies have shown that residents take a longer time to perform tonsillectomies than attending physicians alone. 28 This leads to longer time under anesthesia, and this can result in more nausea and less oral intake.
Increased AHI was correlated with lower oral intake. A higher AHI has been associated with longer operative times, longer time under anesthesia and longer hospital stays. 28 Additionally, Cahali et al 29 found that higher AHI is correlated with larger tonsil volume. This suggests that patients with higher AHI might have larger tonsils and larger resection pockets, leading to more post-operative pain, longer operative time, and more time under anesthesia.
There was no association between instrument used during tonsillectomy and oral intake. It has been reported that monopolar use is associated with shorter operative times than the coblator, though there was no difference in operative time or oral intake related to coblator use in our study. 30 Neeraj et al 31 performed a study with 45 patients and found that there was no significant difference in pain measured with a patient administered pain scale when comparing monopolar and bipolar.
The concurrent performance of myringotomy tube placement seemed to increase post-operative oral intake (median intake 33.6 mL/kg with tube placement vs 24.7 mL/kg without), although this was not statistically significant (P = .062). Rohlfing et al 11 also found no significant association between concurrent myringotomy tube placement and oral intake. Additionally, the concurrent performance of cerumen removal was not significantly associated with oral intake.
Initial 24-hour post-operative oral intake did not have a significant effect on dehydration events in the 30-day post-operative recovery period as measured by parent phone calls and ED revisits. About 1.7% of patients in our study were readmitted for dehydration. This confirms what prior studies have reported.10,11 In a separate analysis, our study also found that the factors that influenced oral intake in the initial 24-hour post-operative period including age, BMI, LOS, and AHI were not associated with post-operative dehydration in the 30-day post-operative recovery period as measured by parent phone calls and ED revisits. This suggests that immediate post-operative oral intake is not predictive of the overall post-operative course, and that significant post-operative dehydration is mediated by other factors such as non-adherence to pain medication, presence of OSA, low socioeconomic or Medicaid payer status, and Spanish as a primary language, possibly related to poor translation of post-operative instructions.32-34
There were several limitations to this study. First, it was conducted at a single institution and patients who returned to an ED outside of our institution were potentially missed in the follow up data, however most outside provider notes are available in the electronic medical record. Additionally, oral intake correlated to body mass as a measure of oral intake is an imperfect method of measuring hydration because changes in body mass may disproportionately influence the value of oral intake compared to what is considered adequate intake to maintain hydration. Variability between providers, anesthetic protocols and nurses potentially limit generalizability of the results reported in this study. Finally, this was a retrospective analysis, which predisposes to inherent limitations such as selection bias and missing data.
Conclusion
This study suggests that older age, higher BMI, higher subjective post-operative pain, increased operative time, increased time under anesthesia, and the presence of a resident during tonsillectomy are associated with lower oral intake in the 24 hours following tonsillectomy performed in children for OSA. These factors can be evaluated to predict and modify post-operative oral intake and pain in the immediate post-operative period following tonsillectomy in children, but it should be noted these factors were not associated with longer term post-operative dehydration in the subsequent recovery period following tonsillectomy.
Footnotes
Acknowledgements
We want to thank the Cooper University Health Care Division of Otolaryngology – Head and Neck Surgery for their help on this project.
Ethical Considerations
This study (IRB number 22-153) was approved by Cooper University Hospital’s Institutional Review Board.
Consent to Participate
Consent to participate in this study was waived by the IRB.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The datasets generated and analyzed during this study are available from the corresponding author upon request.