
Abstract
Background
Bilateral congenital choanal atresia that presents in adulthood is rare. There are only eight reported cases in the literature.
Method
We present a ninth case of adult bilateral choanal atresia diagnosed at the age of 20 years. Can a bilateral choanal atresia present so late in life when such a condition is considered incompatible with life?
Results and Conclusion
Clinical details, diagnosis, and surgical steps with a clear depiction of photographs and comparison with all other previously reported cases, which can help novel otolaryngologists in their clinical practice are discussed.
Case Report
A 20-year-old woman with a poor socioeconomic status presented to the outpatient clinic with chief concerns of nasal obstruction, nasal discharge, snoring, anosmia, and mouth breathing since childhood. Her birth history was uneventful; there was a history of episodes of cyanosis in early childhood, with recovery on crying. There was a history of frequent hospital admissions for recurrent pneumonia in childhood. There was no history of trauma to the nose. Results of a clinical examination a revealed long face with overcrowded incisors, a high-arched palate, and hypoplasia of the maxilla. There were no other congenital anomalies.
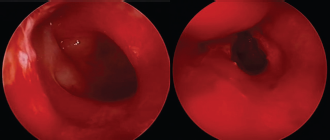
On nasal endoscopy, both nasal cavities were narrow, with absent posterior choanae. Therefore, a diagnosis of bilateral choanal atresia was made (Fig. 1). Computerized tomography of the nose and paranasal sinus showed a thick hypodense sheet of soft tissue completely obliterating the bilateral choanae. There was bowing of the bilateral lateral nasal walls, with thickening of the vomer (Fig. 2).

Nasal endoscopic view of posterior choanae, depicting complete atresia.
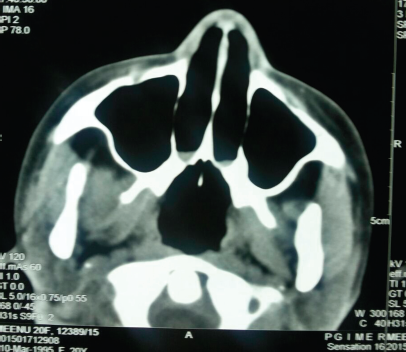
Noncontrast computerized tomography, axial section at the level of posterior choanae, depicting mixed atresia.
An endoscopic choanoplasty was performed in which the membranous atresia was removed by using a microdebrider, and drilling of the vomer and medial pterygoid plates was performed (Fig. 3). A bilateral nasal pack was kept for 5 days. No stenting was done. Thorough nasal douching was advised for the next 2 weeks. At the 3-month follow-up, there were well-patent posterior choanae (Fig. 4). Informed written consent was given by the patient for publication of her case and accompanying images.
Immediate postoperative view of right posterior choana after transnasal endoscopic choanoplasty.
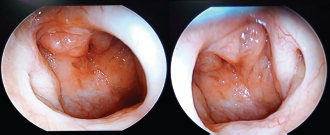
A 1-year follow-up endoscopic photograph, depicting well-epithelized patent posterior choanae.
Discussion
Choanal atresia has an incidence of 1 in 5000 to 1 in 8000 live births. 9 Fifty percent of all patients with choanal atresia and up to 75% of patients with bilateral disease have other associated congenital anomalies. 10 Most common syndromes associated include CHARGE syndrome, Crouzon syndrome, and craniosynostosis. The incidence of mixed atresia is more common than pure membranous and bony atresias 11 as also seen in our case.
Unilateral disease presents most commonly in the later part of life, with nasal discharge and obstruction. Because neonates are obligate nasal breathers, bilateral disease most often presents in the perinatal period, with attacks of cyanosis and apneic attacks. 12 However, in the present case, the parents did not find cyanotic spells, but there were multiple hospital admissions in the patient's childhood. Our patient presented with symptoms of nasal obstruction, discharge, snoring, and mouth breathing, as also noted by Tinoco et al. 1
Nasal endoscopy in our case revealed narrow nasal cavities, thickening of the posterior septum (vomer), medially shrunken lateral nasal walls at the posterior choanae (pterygoid plates), as also noted by other investigators.13,14 Noncontrast computerized tomography of nose and paranasal sinuses helps in assessing the thickness of the atresia and vomer and the position of pterygoid plates, and to distinguish between membranous and bony atresia; it also helps to know the status of the paranasal sinuses.
Transnasal endoscopic choanoplasty was attempted in our patient. The membranous atresia was initially cleared by using a microdebrider. Bony atresia was drilled by using a 2.5-mm cutting burr under direct visualization. 2 The thickened vomerine bone and medial pterygoid plates were drilled until proper visualization of the Eustachian tube opening. The role of a stent is controversial. Some investigators advocate its supremacy. 2 Aksoy et al. 3 used mitomycin C after choanoplasty. In our case, neither of these adjuvants were used. In the postoperative period, the nasal pack was removed after 5 days, and the patient started with nasal douching for 2 weeks. Our patient was followed up for 3 months, and nasal endoscopy revealed well-patent posterior. Of the eight documented cases of bilateral choanal atresia1,3–8,14 in the literature, only one patient had restenosis, which required revision surgery. 4
Conclusion
Bilateral choanal atresia is considered incompatible with life. Early surgical intervention in neonatal period is necessary for survival. Adult bilateral choanal atresia is a rare entity. Bilateral nasal obstruction, recurrent sinusitis, snoring, and mouth breathing are usual symptoms at the time of presentation. Nasal endoscopy and preoperative computerized tomography helps in planning surgery. Endoscopic transnasal choanoplasty is the criterion standard treatment. The exact role of postoperative stenting and the use of mitomycin C are controversial
Footnotes
The authors have no conflicts of interest to declare pertaining to this article