
Abstract
Background
Allergic inferior turbinate hypertrophy is one of the most common causes of nasal obstruction. Several surgical methods can be used for the reduction of allergic inferior turbinate hypertrophy refractory to medical management. Herein, we share our experience with a potassium titanyl phosphate (KTP) laser, which is a relatively novel technique for turbinate reduction.
Objectives
To evaluate the efficacy of KTP laser turbinate reduction in terms of symptomatic improvement and its effect on nasal mucociliary clearance.
Methods
This study was conducted in the Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India, from November 2012 to July 2013. Thirty patients with inferior turbinate hypertrophy refractory to medical management were selected. A KTP laser was used at 6 W in continuous mode, with a spot size of 0.6–1 mm, and energy delivered through a 400–μm optical fiber. A follow-up was done at 1 week, 1 month, and 3 months. All the values (both by the Sino Nasal Outcome Test scoring system and saccharine transit time) were assessed before surgery and at each follow-up visit.
Results
The patients showed significant differences in the symptoms (p < 0.0001) at each follow-up. The mean saccharin transit time showed significant prolongation during the first week and first month after surgery, which indicated adverse effects on the mucociliary system (p < 0.0001). This, however, was a temporary effect, and the mean saccharin time returned to normal limits (17.96 minutes) at the third postoperative month. The mean operative time was 11.62 minutes. The procedure was not associated with any serious intra- or postoperative complications.
Conclusion
KTP laser turbinate reduction is a safe, effective, and minimally invasive procedure in the treatment of allergic inferior turbinate hypertrophy, with a minimal effect on the nasal mucosa. It can be done as an office procedure, with minimal complications.
Over the years, various surgical procedures, such as turbinectomy, turbinoplasty, radiofrequency volumetric tissue reduction, and laser-assisted turbinoplasty, have been advocated for hypertrophy of the inferior turbinate, with the goal of increasing the nasal patency and preserving the mucosa.3–5 An ideal procedure for allergic rhinitis should reduce the symptoms and preserve the nasal mucosa. This prospective study was undertaken to evaluate the efficacy of potassium-titanylphosphate (KTP) laser turbinate reduction in the treatment of ITH secondary to allergic rhinitis and to assess its effect on nasal mucociliary clearance in a south Indian population. The advantages of laser surgery are lack of bleeding, high precision, less intraoperative time, and good healing of the wound. 6 Different types of lasers are used in the medical field, such as carbon dioxide laser, neodymium-doped yttrium aluminium garnet laser, argon laser, diode laser, and KTP laser. This study used a KTP laser for turbinate reduction.
Methods
Our study was a descriptive study. The study protocol was reviewed and approved by the Ethical Committee of Jawaharlal Institute of Postgraduate Medical Education and Research. The treatment procedure was explained to all the patients, and written consent was taken. All adult patients who attended the Otolaryngology outpatient department of Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, from November 2012 to July 2013, with ITH due to allergic rhinitis refractory to medical treatment were included in the study. Patients with bleeding diathesis, acute respiratory tract infections, previous nasal surgeries or trauma, gross deviation of nasal septum, associated sinonasal disease, malignancy of the nose and paranasal sinuses, and comorbidities (e.g., uncontrolled diabetes mellitus and hypertension) were excluded from the study.
A history of persistent nasal obstruction, nasal discharge, and with other symptoms of allergic rhinitis were noted. All the patients received medical treatment in the form of topical nasal decongestants, antihistamines, and topical steroid nasal spray for at least 12 weeks. The patients who had persistent symptoms after 12 weeks were considered as refractory to medical treatment. All the patients underwent a general examination and a detailed otorhino-laryngologic examination. A diagnostic nasal endoscopy was done by using 0° and 30° endoscopes (Karl Storz Endoscopy India Pvt Ltd, New Delhi, India) for evaluation of hypertrophied turbinate and to exclude other pathologies. The absolute eosinophil count and serum immunoglobulin E levels were assessed for all the patients. Patients with symptoms suggestive of allergic rhinitis, such as sneezing, watery nasal discharge, and nasal obstruction; endoscopic signs, such as pale boggy turbinates and watery discharge; peripheral eosinophilia; and elevated serum immunoglobulin E levels, were considered to have allergic rhinitis and were included in the study.
The symptoms of nasal obstruction, headache, sneezing, nasal discharge, and hyposmia, were assessed based on the Sino-Nasal Outcome Test (SNOT) scoring system: 0, no problem; 1, very mild problem; 2, mild or slight problem; 3, moderate problem; 4, severe problem; 5, problem as bad as it can be. The effect of laser on mucosa was assessed by using the saccharine transit time, which was measured by placing a saccharin crystal on the anterior surface of the inferior turbinate on one side of the nasal cavity with the patients in a seated position. The patients were instructed to indicate when they had a sweet taste in the mouth. The time taken from the initial placement of the saccharin to the time they had the sweet taste in the mouth was noted.
KTP laser turbinate reduction was carried out as an outpatient procedure with the patient under local anesthesia. The nose was decongested with cotton pledgets soaked in 4% lignocaine and 1:50000 adrenaline. The patient was placed in the supine position with the head elevated by ~15°. Under aseptic precautions, local infiltration was given on each side with 2–3 mL of 2% lignocaine with 1:200000 adrenaline along the entire length of the inferior turbinate (Figure 1). KTP laser parameters were set to 6 W at continuous mode to generate spot size of 0.6–1 mm, and energy was delivered through a 400–μm optical fiber. The laser tip was held at the contact with the mucosa surface and ~4–5 passes were made along the surface of inferior turbinate in an anterior to posterior direction, each ~1 mm wide (Figure 2). The patients were discharged the same day, after a period of observation in the postoperative room. No nasal packing was required.

Right inferior turbinate being infiltrated with local anesthetic solution.
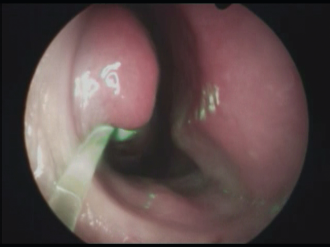
Mucosal passes being made on right inferior turbinate with KTP laser.
Postoperative analgesics were given for 2–3 days, antihistamines for 4 days, and topical nasal decongestant drops for 4–5 days. Antibiotics were not routinely prescribed and were reserved for postoperative complications, e.g., acute sinus infection, bleeding. Follow-up was done at 1 week, 1 month, and 3 months after surgery. At each follow-up visit, nasal obstruction, nasal discharge, sneezing, headache, and hyposmia were assessed by using the SNOT scoring system, and the saccharin transit time was measured (Figure 3). All the data were analyzed by using Statistical Package for the Social Sciences version 19.0, for Window statistical software (SPSS Inc., Chicago, IL). For all the tests, a p value of <0.05 was taken as significant.

A shrunken right inferior turbinate at 3 months after surgery.
Results
All 30 patients completed the study. There were 11 male and 19 female patients. The most common age group was 18–33 years (46.7%); the mean age was 34 years. The most common symptoms were nasal obstruction, nasal discharge, and sneezing, followed by headache and hyposmia (Table 1). SNOT scores assessed for each symptom before surgery and at each follow-up visit are depicted in Table 2. The Wilcoxon matched-pairs test was used to find if any significant difference in SNOT score existed between the pre-and postoperative follow-up after 1 week, 1 month, and 3 months. The difference between the preoperative SNOT score and the score at each visit was significant for all the symptoms (p < 0.0001).
Frequency of symptoms before surgery

SNOT score for each symptom

SNOT = Sino-Nasal Outcome Test.
The preoperative mean saccharin transit time was 17.10 minutes, which showed significant prolongation in the first week and first month after surgery (p < 0.0001). It, however, returned to a normal value of 17.96 minutes in the third postoperative month (Table 3). The mean duration of surgery was 11.62 minutes. There were no major or minor complications during surgery, apart from a burning sensation in the nose during the procedure, which was noted in three patients. The most common complication noted in the early postoperative period was crusting, which persisted in a few patients for up to 1 month (Table 4). Overall, there was improvement in the symptoms of nasal obstruction, nasal discharge, sneezing, headache, and hyposmia in 73.33, 83.33, 76.67, 73.68, and 77.78% of patients, respectively (Table 5).
Mean saccharin transit time at each visit

Postoperative complications at each visit

Number of patients who obtained symptom relief at 3 months

Discussion
Inferior turbinate laser treatment has been popularized as a therapeutic alternative treatment for patients with persistent nasal obstruction and hypertrophy of the inferior turbinates. Laser turbinate reduction in allergic rhinitis cannot be expected to cure allergy, although some relief of symptoms from allergy is to be expected. A KTP laser has a wavelength of 532 nm, which is within the visible range. The laser beam has an emerald green color, which is effectively absorbed by pigments such as hemoglobin and melanin. The laser beam interacts with these pigments and produces a localized coagulation, which makes the laser highly effective in highly vascularized tissue such as the turbinate. In this study, we used a KTP laser to reduce the turbinate hypertrophy and assess its postoperative effects on various symptoms of allergic rhinitis. There are few studies that demonstrate the effectiveness of KTP laser turbinate reduction in reducing the symptoms with ITH.7–13
The mean duration of our procedure was observed to be 11.62 minutes, which was in accordance with the finding of the study conducted by Orabi and Sen, 12 that the mean intraoperative time of KTP laser turbinate reduction was 12.7 minutes. All the patients showed statistically significant improvement in all the symptoms after surgery. Nasal discharge and sneezing were relieved in 83.33% and 76.67% of the patients, respectively, at the end of the 3-month follow-up period. The relief in nasal discharge and sneezing may be attributed to destruction of highly vascular submucosa and transection of nerve fibers, which are branches of postnasal nerve, respectively. These findings correlated with the previous studies on KTP laser; 73.33% of the patients were relieved of nasal obstruction, which may be due to the scar tissue of the lasered turbinate preventing the rapid congestion and decongestion swings of the turbinate as proposed by Fukutake et al. 14
At the 3-month follow-up period, 73.68% of patients were relieved of headache. The improvement in headache could be attributed to a decrease in septoturbinal headache owing to the loss of contact between the septum and the turbinate, and reduction in chronic nasal stuffiness and discharge. These results were similar to a study conducted by Matteo et al., 15 who compared radiofrequency turbinoplasty with traditional surgical techniques and found relief from headache by 66–69% in both groups. Improvement in perception of smell, which may be attributed to the improvement in nasal patency after surgery, was found in 77.78% of patients. Elwany and Harrison 5 showed similar improvement in hyposmia after inferior turbinectomy.
This study was novel in assessing the effect of KTP laser turbinate reduction on nasal mucociliary clearance. We found that the average saccharine transit time was prolonged at the end of the 1-week and 1-month follow-up periods but returned to near preoperative values by the end of the 3-month follow-up period. This finding may be attributed to the initial scarring produced by the laser on the surface of inferior turbinate. Janda et al. 16 found that there was no significant variation in saccharine transit time in comparison with the preoperative measurements 1 year after diode laser treatment on turbinate.
Three patients experienced a burning sensation in the nose during surgery, which may have been due to insufficient local anesthesia, which was the sole intraoperative complication. Crusting was the most common postoperative complication observed overall as well as in the first week. Crusting at the end of first week was observed in 46.67% of the patients, in 16.66% by 1 month, and none by the third month. This could partly be ascribed to incidental injury to septal mucosa caused by scattered laser energy or direct mucosal trauma from instrumentation. 7 Intranasal irrigation was done for all the patients with crusting. Two patients had blood-stained discharge and minimal pain, which could have been due to the manual dislodgement of crusts.
Conclusion
KTP laser–assisted turbinate reduction showed promising results in reducing the symptoms of allergic rhinitis and can be performed as a day care procedure, with minimal complications. Although nasal mucociliary clearance was temporarily impaired in the initial postoperative period, it returned to normal thereafter. Thus, KTP laser–assisted turbinate reduction this procedure can be considered as a safe, effective, and minimally invasive procedure for turbinate reduction in allergic ITH.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article